
Abstract
We performed a long-term follow-up examination in children and adolescents with migraine and tension-type headache (TTH) in order to investigate the evolution of clinical features and headache diagnoses, to compare International Classification of Headache Disorders (ICHD)-I and ICHD-II criteria and to identify prognostic factors. We re-examined 227 patients (52.4± female, age 17.6 ± 3.1 years) 6.6 ± 1.6 years after their first presentation to a headache centre using identical semistructured questionnaires. Of 140 patients initially diagnosed with migraine, 25.7± were headache free, 48.6± still had migraine and 25.7± had TTH at follow-up. Of 87 patients with TTH, 37.9± were headache free, 41.4± still had TTH and 20.7± had migraine. The number of subjects with definite migraine was higher in ICHD-II than in ICHD-I at baseline and at follow-up. The likelihood of a decrease in headache frequency decreased with a changing headache location at baseline (P < 0.0001), with the time between baseline and follow-up (P = 0.0019), and with an initial diagnosis of migraine (P = 0.014). Female gender and a longer time between headache onset and first examination tended to have an unfavourable impact. In conclusion, 30± of the children and adolescents presenting to a headache centre because of migraine or TTH become headache-free in the long-term. Another 20–25± shift from migraine to TTH or vice versa. ICHD-II criteria are superior to those of ICHD-I in identifying definite migraine in children and adolescents presenting to a headache centre. The prognosis is adversely affected by an initial diagnosis of migraine and by changing headache location, and it tends to be affected by an increasing time between headache onset and first presentation.
Introduction
Recurrent primary headaches may have a considerable impact on the quality of life of children and adolescents due to unpredictable headache attacks facultatively associated with further symptoms such as nausea, vomiting, photo- and/or phonophobia. As a consequence of the headache, (psycho)social functioning may be impaired in various areas including family, peer group, friends, leisure time activities and working capacity and productivity at school or at work (1, 2). Information on the prognosis of primary headaches is therefore essential.
The prevalence of migraine in children and adolescents has been examined in a large number of papers. Studies applying the International Headache Society (IHS) criteria reported prevalence rates between 3% and 11% (3–7). Epidemiological data on tension-type headache (TTH) in young subjects have become available in recent years only and suggest prevalence rates between 10% and 24% (6–8).
Longitudinal studies with follow-up examinations of headache sufferers over years are required to acquire information about the long-term course of primary headaches. Questions which can be answered by those studies are the proportions of subjects who (i) become headache-free, (ii) improve, remain stable or deteriorate with respect to headache frequency, duration, and/or symptomatology, and (iii) continue to have headache of the same type or change from one type to another. In addition, longitudinal studies allow identifying prognostic factors.
Recently, several studies on the long-term course of primary headaches in children and adolescents have been published (9–18). The epochal follow-up examinations of children with pronounced migraine performed by Bille (9) covering an observation period of 40 years have demonstrated a considerable variability in the long term course, including permanent remissions, relapses after headache-free periods over many years as well as continuing or worsening of the original symptoms. Around the age of 50, more than half of the patients still had migraine attacks. Another important point in Bille's study is the considerable recall bias (e.g. 41% of the subjects asked at middle age could not remember that they had had aura symptoms at younger ages). Three additional longitudinal studies (10–12), including 64–181 patients and covering follow-up periods of between 3 and 10 years, focused on migraine. A large epidemiological study (13) examined the prevalence of ‘headache disturbing the daily activities’ without providing precise headache diagnoses. One clinic-based study (14) focused on patients with definite migraine and TTH according to the criteria of the IHS another one (15) was restricted to subjects with migraine and TTH not fulfilling the IHS criteria. Two recent studies dealt with chronic daily headache (16) and idiopathic headache in children under 6 years of age (17), respectively. A large Italian multicentre study (18) included all forms of migraine and TTH, but the follow-up period was 3 years only.
The percentage of subjects who became headache-free varied considerably in these studies and ranged between 5% and 45% (10, 12, 14, 15, 18). Studies providing detailed headache diagnoses suggest that up to one-quarter of the patients may evolve from migraine to TTH or vice versa (10, 12, 14, 15). Among the prognostic factors, an early age of onset (11), psychosocial stressors (10) and psychiatric comorbidity (19) may be related to an unfavourable outcome, whereas the importance of gender remains unclear (10, 14).
The considerable variation in the results of these studies is due to marked methodological differences concerning study population, diagnostic criteria, duration of follow-up and outcome measures. Among the six studies applying the IHS criteria, only one included more than 200 patients (18) and one covered a follow-up period of more than 5 years (14).
The aim of this longitudinal study was to examine the evolution of the clinical features and headache diagnoses in a large sample of children and adolescents referred to a headache centre for migraine or TTH. In addition, we wanted to compare the diagnostic criteria of the second edition of the International Classification of Headache Disorders (ICHD-II) (20) with those of the first edition (ICHD-I) (21), and finally, we intended to analyse possible prognostic factors of migraine and TTH in children and adolescents.
Patients and methods
In a previous study we examined the applicability of the IHS criteria in a sample of 437 children and adolescents who had been referred to a headache centre (22). For the present follow-up examination we excluded 28 patients who had secondary (n = 26) or unclassifiable headaches (n = 2) and we tried to contact all others (n = 409). In total, 227 of these patients (55.5%) were available for follow-up. One hundred and seventy-eight patients could not be reached, because they did not respond to three phone calls and a letter or because their current address and phone number were not available. The parents of two children refused participation in the follow-up study and two adolescents had died, one in an accident, the other of bone cancer.
In the present study, we used the same semistructured questionnaire as in the first one (22). In short, this questionnaire covered biographical data, age, sex, family headache history, duration of the headache history, frequency and duration of the headaches as well as the location, quality and intensity of the pain, the influence of physical activity, occurrence of nausea, vomiting, photo- and phonophobia, and the occurrence and duration of neurological symptoms (22–24).
The questionnaire incorporated all items required for diagnosing headache according to the criteria of ICHD-I and ICHD-II (20, 21). The patients were interviewed alone or in the presence of a parent by one of three physicians with at least 2 years of neuropsychiatric experience. Children and adolescents who no longer suffered from headaches and those who could not visit the clinic for the follow-up examination were interviewed by telephone. Two supervisors (C.W-B., C.W.) discussed each patient with the doctor in attendance and were responsible for the final diagnosis, which they reached together.
Patients were classified as headache-free if they had no headaches during the 12 months preceding the follow-up interview. To characterize the general course of the headaches between baseline and follow-up, we evaluated the number of patients with a favourable prognosis. This included headache-free patients and those reporting a reduction in headache frequency of ≥50%.
For statistical analysis, χ2 and Wilcoxon tests were used to compare the baseline findings in patients with and without follow-up. McNemar tests and Wilcoxon tests were calculated to compare the one-digit ICHD-II diagnoses, the headache characteristics and associated symptoms at baseline and at follow-up in patients with persisting headache. The analysis of factors predicting the presence and frequency of headache at follow-up comprised all patients of the follow-up group and included the following variables: age at onset of headache, at baseline and at follow-up, sex, time from onset of headache to baseline and from baseline to follow-up, headache characteristics and one-digit ICHD-II diagnoses at baseline and family history of headache. Predictors for the presence of headache at follow-up were assessed with univariate logistic regression analyses. Predictors for the change in frequency from baseline to follow-up were assessed with linear regression analyses correcting for the covariate frequency at baseline, which had a significant influence in all analyses and is not reported separately. All variables showing a significant association at the 5% level were included in a multivariate regression analysis. To account for multiple testing, we report which findings remain significant after Bonferroni correction. The two-sided significance level was set to 5%.
Results
Baseline data
Comparing the baseline data of subjects with and without follow-up showed no differences in age, sex, age at onset of headache, frequency, location and quality of headache, aggravation of headache by physical activity, nausea, vomiting, photophobia, phonophobia and aura symptoms, one-digit ICHD-II diagnoses or family history of headache. Three variables differed at the 5% level. In detail, the time between onset of headache and baseline as well as the headache duration were shorter in follow-up patients (median time since onset 24 vs. 36 months, P = 0.035; median duration 4 vs. 5 h, P = 0.013) and headache was less often severe (56% vs. 69%, P = 0.008). After Bonferroni correction for 17 tests, however, these differences failed to reach the level of statistical significance.
Characteristics of follow-up patients
The mean interval between the first study and the follow-up study was 6.6 ± 1.6 years (range 5–8 years). The mean age of the patients at the time of follow-up was 17.6 ± 3.1 years (range 11–26 years); 119 patients (52.4%) were female and 108 (47.6%) were male. Seventy percent of the patients had a favourable prognosis, i.e they were either headache free during the 12 months before the follow-up investigation or they reported a decrease in headache frequency of ≥50%. Among 34 patients with chronic daily headache, including eight patients with chronic migraine, four with probable chronic migraine, 15 with chronic TTH and seven with probable chronic TTH, 31 (91%) had a favourable prognosis. Twelve of these patients became headache free, 14 had headache on ≤4 days per month and five patients on 5–12 days. Among the latter, headache duration was ≤4 h and intensity was mild in three patients each.
Regarding headache therapy, we provided education to all patients and parents as well as recommendations for recognizing trigger factors and modifying lifestyle. All patients kept a headache diary and were seen at least twice after the first consultation. Non-pharmacological prophylactic treatment was started if headache frequency in the diary showed no meaningful improvement. In the rare cases of ineffectiveness of the non-pharmacological measures, pharmacological prophylaxis was used. This was necessary in less than 5% of the subjects and consisted most frequently of flunarizine for frequent migraine attacks given over a period of 3 months. Acute medication was taken by 67% of the patients.
Headache diagnoses
All diagnoses are based on the criteria of ICHD-II. Of the 227 patients included in the follow-up examination, 140 (61.7%) had migraine and 87 (38.3%) had TTH at the time of the first investigation. At follow-up, 69 patients (30.4%) were headache free for at least 1 year, 86 patients (37.9%) had migraine, and 72 (31.7%) had TTH. The detailed diagnoses according to ICHD-II are shown in Table 1.
Headache diagnoses according to the 2nd edition of the International Classification of Headache Disorders (ICHD-II) at baseline and at follow-up in 227 children and adolescents presenting with primary headaches to a headache centre

Comparing the migraine diagnoses according to ICHD-II with those according to ICHD-I (Fig. 1) demonstrated that the number of patients fulfilling all but one criterion of migraine (i.e. probable migraine according to ICHD-II and migrainous disorder according to ICHD-I, respectively) was reduced by 60% (from 50 to 20) at baseline and by 58% (from 19 to eight) at follow-up. This improvement of the sensitivity is mainly due to the reduction in the minimum duration of migraine without aura from 2 h in ICHD-I to 1 h in ICHD-II. A few patients shifted to definite migraine, since ICHD-II allows bilateral pain location in children with migraine.
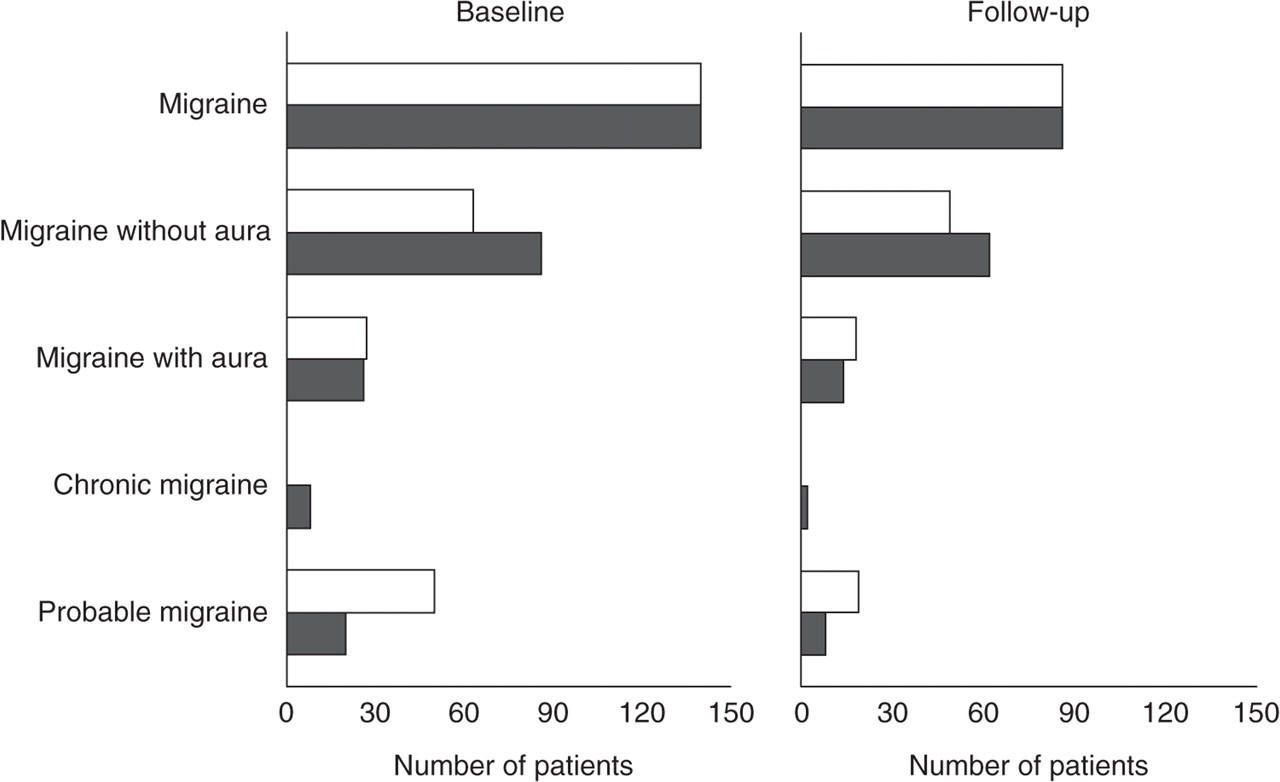
Comparison of migraine diagnoses according to International Classification of Headache Disorders (ICHD)-I (□) and ICHD-II (▪).
Of the 140 patients with migraine at the time of the first examination, 36 (26%) were headache free, 68 (49%) were still suffering from migraine, and 36 (26%) had shifted to TTH at follow-up. The evolution of the headache diagnoses in subjects initially classified as migraine without aura, migraine with aura, chronic migraine and probable migraine, respectively, is shown in Table 2.
Evolution of headache diagnoses in 140 patients initially diagnosed with migraine

=, Number of patients with identical diagnoses at baseline and at follow-up. Results may not be exact due to rounding.
Of the 87 patients with TTH at baseline, 33 (38%) were headache free, 36 (41%) were still suffering from TTH and 18 (21%) had migraine at follow-up. The evolution of the diagnoses in subjects initially classified as infrequent episodic, frequent episodic, chronic and probable TTH, respectively, is shown in Table 3.
Evolution of headache diagnoses in 87 patients initially diagnosed with tension-type headache

=, Number of patients with identical diagnoses at baseline and at follow-up. Results may not be exact due to rounding.
The percentages of subjects which were headache free at follow-up for at least 1 year varied considerably in the different headache types and was lowest in patients with chronic migraine (one of eight patients) and highest in those with infrequent episodic TTH (three of four patients). In general, the percentages of headache-free subjects were higher in TTH than in migraine, but the difference was not statistically significant (Tables 2 and 3). A shift from migraine to TTH occurred most often in patients initially classified as chronic migraine and least often in those classified as migraine without aura. A shift from TTH to migraine was observed most often in frequent episodic TTH and least often in chronic TTH (Tables 2 and 3).
Considering the shifts between migraine and TTH in many patients, we re-classified post hoc all TTH patients applying the alternative diagnostic criteria given in the appendix of ICHD-II. According to this proposal, at least three pain characteristics (pressing/tightening, non-pulsating quality; mild or moderate intensity; bilateral location; not aggravated by routine physical activity) must be fulfilled and nausea, vomiting, photophobia and phonophobia must be absent. As shown in Fig. 2, the number of patients shifting from migraine to TTH or vice versa did not differ between restrictive and conventional criteria.

Evolution of headache diagnoses and comparison of conventional (TTH-C) and restrictive (TTH-R) criteria of tension-type headache at baseline and at follow-up.
Among patients with persisting headache, the percentage of migraineurs decreased and the percentage of patients with TTH increased from baseline to the time of follow-up (P = 0.039).
Headache characteristics and associated symptoms
During the follow-up period headache characteristics and associated symptoms changed markedly. The detailed evolution of the headache characteristics and associated symptoms is given in Table 4.
Evolution of headache charactersitics and associated symptoms in 227 children and adolescents

=, Number of patients with identical symptoms at baseline and at follow-up.
In the 158 patients with persisting headache, duration, pulsating quality, aggravation by physical activity, photophobia and phonophobia increased, whereas frequency, nausea and vomiting decreased (Table 5).
Evolution of ICHD-II diagnoses, headache charactersitics and associated symptoms in 158 patients with persisting headache
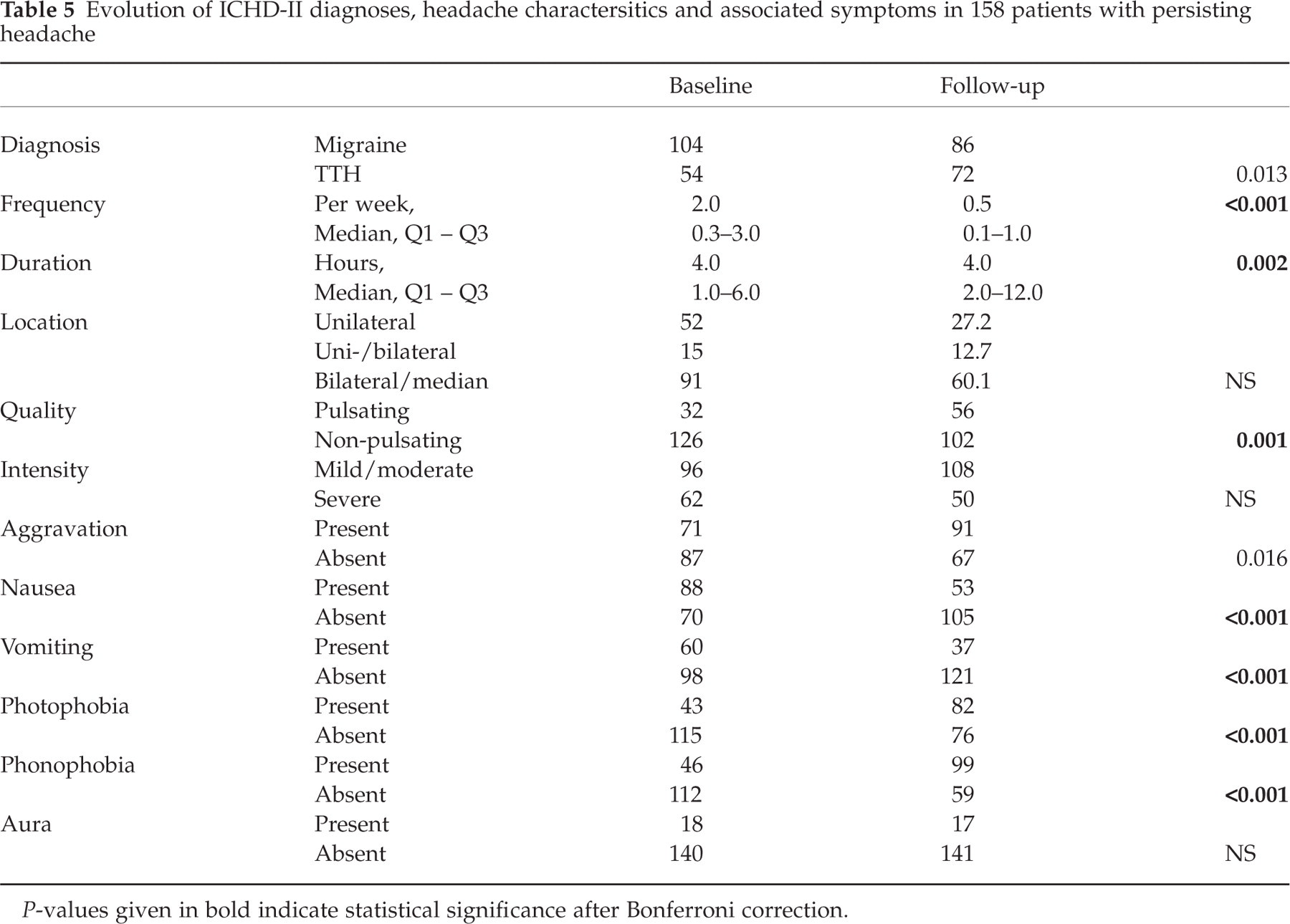
P-values given in bold indicate statistical significance after Bonferroni correction.
Patients with persistent headache and a baseline diagnosis of migraine and TTH reported a decrease in headache frequency by at least 50% in 51% and 68.5%, respectively, whereas they experienced an increase by 50% or more in 24% and 14.8% only, respectively.
Prognostic factors
In patients who were headache-free for at least 1 year, the time between the onset of headache and the first visit at the clinic was significantly shorter than in those with persistent headache (median 18 vs. 24 months, P = 0.016). In contrast, the age and sex of the patients, the duration and frequency of headache, the headache characteristics and the associated symptoms at baseline did not differ in the two groups. A stepwise logistic regression model confirmed these findings, selecting the time since onset of headache (P = 0.017) as the only factor differentiating between headache-free subjects and patients with persistent headache. After Bonferroni correction for 18 tests the result was not statistically significant, however.
The univariate analysis of factors predicting headache frequency at follow-up identified four variables. An increase (or less decrease) of frequency was associated, with female gender (P = 0.04), an initial diagnosis of migraine (P = 0.02), a changing headache location at baseline (P < 0.0001) and a longer time between baseline and follow-up (P < 0.0001). The latter two remained statistically significant after Bonferroni correction for 17 tests. The multivariate analysis identified an initial migraine diagnosis (P = 0.014), the time between baseline and follow-up (P = 0.0019) and changing headache location (P < 0.0001) as independent predictors.
Discussion
This longitudinal study in children and adolescents referred to a headache centre for migraine and TTH showed a favourable prognosis in 70% of the patients. There was a considerable shift from migraine to TTH and vice versa and the headache characteristics changed markedly from baseline to follow-up. Comparing ICHD-I with ICHD-II criteria demonstrated that the proportion of patients with definite migraine was significantly larger in ICHD-II. Evaluating the usefulness of more restrictive criteria for TTH as proposed in the appendix of ICHD-II did not suggest an advantage in differentiating TTH from migraine in children and adolescents. Regarding prognostic factors of migraine and TTH, an initial diagnosis of migraine, changing headache location at baseline and a longer follow-up period were related to an increase (or less decrease) of headache frequency. Female gender and a longer time between headache onset and first examination tended to have an unfavourable impact.
Prognosis of migraine and tension-type headache
Methodological differences concerning study population, diagnostic criteria, duration of follow-up and outcome measures make it difficult to compare the findings of the present study with those of the literature. Comparable to our results, several previous studies have reported that about 30% of children and adolescents with migraine or TTH become headache-free (12, 14, 18), whereas other studies have found remission rates of <5% or >40% (10, 11).
Beside complete remission, the decrease of headache frequency is an important determinant of the prognosis. Dooley and Bagnell (25) reported improvement in 54% of their patients. Guidetti et al. found an improvement in headache frequency and/or severity in 45% and they reviewed previous studies published between 1956 and 1983 reporting an improvement in 37% to 50% of the children and adolescents with migraine and other (primary) headaches, respectively. Differentiating between migraine and TTH, we found a decrease in headache frequency of ≥50% in one of two patients with migraine and in two-thirds of subjects with TTH.
Evolution of headache diagnoses
A shift from migraine to TTH and vice versa was reported previously by other authors and their findings compare very well to our own results (12, 14, 25). In the study by Guidetti et al. (14), 26.5% of the patients initially diagnosed with migraine changed to TTH and 8.3% of those initially diagnosed with TTH changed to migraine. Dooley and Bagnell found a shift in 25.9% and 11.0%, respectively (25). Our study is the first to apply ICHD-II criteria and to differentiate four subtypes of migraine and TTH. The percentages of patients evolving from migraine without aura and migraine with aura into (frequent) episodic TTH or vice versa are similar to those reported by Guidetti et al. (14). Remarkably, all subjects with chronic migraine and chronic TTH, respectively, evolved into episodic headache or became headache free. Out of 15 patients with chronic TTH, none developed definite migraine, whereas three of eight patients with chronic migraine evolved into frequent episodic TTH. This disappearance of migrainous features may correspond to recent findings of Bigal et al. (26) indicating that migraine days decline with the duration of illness in adolescents with transformed migraine. The evolution of probable migraine and probable TTH was examined in only one previous study, which used the ICHD-I criteria and which was published by our group several years ago (15). In this study, 39.7% of the patients with ‘probable migraine’ (migrainous disorder according to ICHD-I) retained this diagnosis, whereas in the present study none of the patients had probable migraine at follow-up. This difference can be explained by the longer follow-up period in the present study increasing the chance of evolving into definite migraine and by an improvement in the sensitivity of the diagnostic criteria for migraine in ICHD-II compared with ICHD-I.
Diagnostic criteria
Previously numerous cross-sectional and few longitudinal studies have compared the ICHD-I criteria with alternative diagnostic criteria of migraine (18, 22). Recently, ICHD-II criteria were compared with alternative ones in children <6 years old (17). This is the first longitudinal study comparing ICHD-I with ICHD-II in children and adolescents and evaluating in addition the usefulness of more restrictive criteria of TTH as given in the appendix of ICHD-II. We were able to demonstrate clearly that the ICHD-II criteria of migraine are superior to those of ICHD-I. The application of the restrictive criteria for TTH, however, was not associated with an increased diagnostic stability, as the number of patients shifting between migraine and TTH was similar with restrictive and conventional criteria.
Evolution of headache characteristics
Regarding the headache characteristics, our study demonstrated marked changes, particularly with respect to the associated symptoms. The prevalence of photo- and phonophobia had increased and that of vomiting had decreased at follow-up. In addition, our study confirms the results of cross-sectional examinations (22–24) suggesting increasing headache duration with increasing age. Details on the evolution of the headache characteristics have been given in few previous studies only (15). Recently, the variability of headache symptoms was studied comprehensively in adults (27). This community-based study showed that the 1-year reproducibility of reporting migraine headache symptoms is only moderate, varies between symptoms, and leads to instability in the formal assignment of a migraine headache diagnosis and to diagnostic drift between headache types. The authors conclude that this finding is compatible with the continuum model of headache, where headache attacks can vary along a severity continuum from episodic TTH to full-blown migraine attacks. In children and adolescents, the changes in headache symptomatology might be explained by the continuum model. However, the impact of developmental factors must also be considered and a persistent change from migraine to TTH without continuous variation along a severity continuum cannot be excluded and requires further longitudinal studies.
Prognostic factors
Evaluating predictors for the presence of headache at follow-up, the time between the onset of headache and the first visit at the clinic was the only variable identified in a univariate regression analysis. Even though the level of statistical significance was missed after Bonferroni correction, this finding suggests that early intervention might improve the prognosis of migraine and TTH in children and adolescents. Regarding an increased headache frequency at follow-up, four predictors were identified, i.e. female gender, a baseline diagnosis of migraine, a changing headache location at baseline and a longer follow-up period. The impact of female gender failed to reach the level of statistical significance on multivariate analysis. Moreover, the reports in the literature are inconclusive, as some authors have found an unfavourable prognosis in females (9, 14) and others in males (10, 18). The finding that the baseline diagnosis of migraine was related to an increased headache frequency at follow-up is in contrast to another study reporting a higher percentage of improvement in migraineurs (14). The prognostic relevance of changing headache location was an unexpected finding and requires further confirmation. There is only one other study in the literature evaluating in detail the prognostic importance of headache characteristics, without revealing any statistically significant result (11). Finally, the relation between an increased headache frequency and an increasing length of the follow-up period seems to reflect the variable course of migraine and TTH characterized by phases with frequent and infrequent attacks and headache-free periods, as demonstrated for migraine patients in the pioneering work of Bille (9).
Limitations of the study
The study was performed in a headache centre and does not allow conclusions about children and adolescents with migraine or TTH from the general population. Even though we used all available sources of information, the number of patients who could not be reached was unexpectedly high. The dropout rate of 44.5% is comparable to another large study with a rate of 38% (18). Possible explanations for the difficulties in reaching the patients are the frequent change to mobile phones, more frequent changes of the telecom supplier, and more frequent changes of the place of residence, reflecting in part the high rate of divorce (in the year 2000, 19 552 divorces affected 18 044 children and adolescents in Austria). Comparing the baseline data of the patients with and without follow-up showed a few differences at the 5% level, but after Bonferroni correction these differences failed to be statistically significant. Finally, the prognostic findings are limited to headache characteristics, since other factors such as psychosocial functioning and comorbidity were not considered.
Conclusion
In the long term, 30% of the patients become headache free and another 20–25% shift from migraine to TTH or vice versa. ICHD-II criteria are superior to those of ICHD-I in identifying definite migraine in children and adolescents presenting to a headache centre. The prognosis is adversely affected by an initial diagnosis of migraine and by changing headache location and it tends to be affected by an increasing time between headache onset and first presentation. Future studies should address the question, whether early therapeutic intervention, particularly in children and adolescents with migraine, has an effect on the long-term prognosis.