
Abstract
We investigated a possible correlation between brain excitability in children with migraine and tension-type headache (TTH) and their behavioural symptomatology, assessed by using the Child Behaviour Checklist (CBCL). The mismatch negativity (MMN) and P300 response were recorded in three successive blocks to test the amplitude reduction of each response from the first to the third block (habituation). MMN and P300 habituation was significantly lower in migraineurs and TTH children than in control subjects (two-way ANOVA: P < 0.05). In migraineurs, but not in TTH patients, significant positive correlations between the P300 habituation deficit and the CBCL scores were found (P < 0.05), meaning that the migraineurs with the most reduced habituation showed also the worst behavioural symptomatology. To the best of our knowledge, this is the first study showing a correlation between neurophysiological abnormality and emotional symptomatology in migraine, suggesting a role of the latter in producing the migrainous phenotype.
Introduction
Headache with onset in childhood represents a matchless opportunity to study headache disorders within a short time of their onset, allowing close monitoring of the child's environment (family, school, etc.), the interviewing of parents (e.g. on their own headache, personal clinical history, child's personality characteristics, headache symptoms), and so on. Although primary headaches have a high prevalence in the paediatric population, the pathophysiology of these diseases still remains obscure. In children and adolescents, the most represented types of primary headache are migraine and tension-type headache (TTH) (1). The International Headache Society criteria (2) state that episodic TTH and migraine are distinct disorders. However, according to the concept of the continuum model there is also the hypothesis that TTH and migraine are part of the same physiological spectrum (3).
The importance of psychological factors in migraine pathophysiology has been suggested by several studies that have shown typical personality traits in migraine children (4–7). However, the psychological factors probably act on a predisposed background that can be determined genetically (8–11). An increasing number of studies on migraine show functional abnormalities of the central nervous system neurons, which result in an altered cerebral cortex excitability (11). The main neurophysiological marker of this abnormal excitability of the cerebral cortex in migraine is represented by a reduced habituation of the sensory cortices to the afferent inputs during the interictal phase (for reviews see (12, 13)). In healthy subjects, due to habituation, the evoked potential (EP) amplitude tends to decrease during repetitive sensory stimulation. In migraine, experimental studies aiming at the investigation of EP modification after repetitive stimulation have shown a lack of habituation in both children and adults (14–23).
In adults, the phenomenon of reduced EP habituation is thought to be specific to migraine, it being absent in TTH patients (19, 23, 24). This suggests a different pathophysiology between migraine and TTH. In children, EP habituation has rarely been compared between migraineurs and TTH patients, and the results disagree (16, 25, 26).
In the present study, we aimed to investigate the possible correlation of emotional symptomatology with abnormal brain excitability in children with migraine and TTH compared with healthy subjects. Children's behavioural symptomatology was assessed by means of the Child Behaviour Checklist (CBCL), a device by which parents may rate a child's problem behaviours and competencies (27). Brain excitability was evaluated by measuring the habituation of two auditory event-related potentials (ERPs): (i) the mismatch negativity (MMN), which is believed to reflect the automatic central processing of a novel stimulus and is independent of attention (28); and (ii) the P300 potential, which is released after a conscious perceptual decision (29, 30).
Materials
Subjects
Thirty-eight subjects participated. All of them and their parents gave informed consent. Eighteen patients had migraine without aura (MoA) (mean age 10.5 ± 2 years, nine male, nine female), and 10 suffered from TTH (mean age 12 ± 2.8 years, four male, six female). They were consecutively chosen from patients referred for consultation at our Headache Centre. Lastly, 10 healthy children were the control subjects (CS) (mean age 11.8 ± 2.5 years, five male, five female). MoA and TTH patients were diagnosed according to the criteria of the International Classification of Headache Disorders, 2nd edn (ICHD-2) (2). All of them had had the first headache attack at least 1 year before being included in our study. Clinical characteristics of our headache patients are summarized in Table 1. We ensured that they did not suffer from any other neurological or internal disease. The ERP recordings were performed no sooner than 72 h after the last headache attack. Moreover, in no patient did a headache attack follow the ERP recording in the next 72 h. No patient took any drug during the 72 h before the ERP recording was performed. In selecting the CS, children whose first- or second-degree relatives suffered from migraine were excluded. All the children had normal hearing. Neither CS nor patients had ever had a previous psychological screening.
Clinical characteristics of headache patients

TTH, tension-type headache.
ERP recording
For ERP recording, subjects were comfortably seated in a quiet room. In all children the MMN recording always preceded the P300 recording.
Auditory stimuli were sinusoidal tones (10 ms duration, 2 ms rise and 2 ms fall time, 85 dB sound pressure level of intensity), presented binaurally via headphones (Medelec Synergy, Oxford Medical Instruments, Ltd, Abingdon, UK). Frequent 750-Hz tones and deviant 500-Hz tones were presented with a probability of 85% and 15%, respectively, with an interstimulus interval of 1 s.
ERPs were recorded from three electrodes on the scalp, located at T3, T4, Cz positions of the 10–20 system. Electrooculogram was monitored by an electrode placed in the outer cantus of the right eye. The nose served as reference for all electrodes. We are aware that the MMN is better recorded on the frontal region, but we chose to put our midline electrode at Cz vertex, since this position is suitable to record both the MMN (31) and the P300 response. EEG was recorded with a sampling rate of 1024 Hz. The analysis time was 1000 ms, including 100 ms of prestimulus delay. The amplifier bandpass was 0.1–30 Hz (24-dB roll off) (Medelec Synergy, Oxford Medical Instruments). An automatic artefact-rejection system excluded from the average all runs containing transients exceeding ± 150 μV at any recording channel. The mean rejection rate was 5%.
MMN recording
Participants underwent three successive blocks (see below) of about 330 acoustic stimuli. During the recording, children were instructed to pay no attention to the acoustic stimulation and to read a novel. Subjects were informed that they had to summarize the novel in a short briefing following the stimulation.
P300 recording
Children underwent three successive blocks (see below) of about 200 acoustic stimuli. During the recording, children were instructed to count the number of infrequent tones mentally. Subjects were informed that the precision of their counting would be verified in a short briefing following the stimulation. Averages in which a counting mistake exceed 10% were not considered in the data analysis.
ERP habituation
To test the ERP habituation, three consecutive blocks were recorded for both the MMN and P300 potentials, each block being separated from the following one by a time interval of 5 min. After the MMN recording end, the P300 recording began after a time interval of at least 10 min.
ERP analysis
In MMN recording, difference traces, obtained by subtracting the frequent stimulus ERP from the deviant stimulus ERP, were obtained. A negative deflection, showing an average latency of around 139 ms in healthy subjects, was identifiable in Cz trace. The distribution of this deflection (negative on Cz trace, positive on temporal traces) was consistent with the typical distribution of the MMN (Fig. 1). The peak latency of the MMN and its amplitude from the baseline were measured.

Mismatch negativity (MMN) and P300 recordings (I, II and III block) in three representative subjects (one control subject, one migraineur, and one tension-type headache patient). Whereas both MMN and P300 amplitude are reduced in amplitude from the first to the third block in the control, no amplitude reduction can be observed in the patients.
In P300 recording, a large positive potential, showing an average latency of around 317 ms in healthy subjects, was identifiable in all scalp traces, but reached its maximal amplitude on Cz vertex. The widespread distribution of this wave was consistent with that of the P300 potential (Fig. 1). The peak latency of the P300 and its amplitude from the baseline were measured.
Psychological evaluation
The assessment tool was the CBCL/4–18 (27). The CBCL is a parent-rating scale to assess competences, emotional and behavioural problems in children and adolescents aged 4–18 years; it is an easy-to-administer measure that takes about 20–30 min to complete. The questionnaire consists of two parts: ‘Competences’ and ‘Emotional and Behavioural Problems’ scales. In the first section, social competence is covered by three scales: Activity scale, Social scale and School scale. According to the main aim of our study, we administrated only the second section of CBCL, because it deals with internalizing and externalizing disorders. Multivariate analyses have identified two main group problems: ‘Internalizing scale’ (anxious and inhibited behaviour) and ‘Externalizing scale’ (aggressive and antisocial behaviour). The second section assesses the psychological profile by a dimensional approach. Parents judge 118 items, according to different categories (each scored from 0 to 2): ‘not true’ (0), ‘somewhat true’ (1) or ‘always or often true’ (2). Items are grouped in eight narrow-band subscales: ‘Withdrawn’, ‘Somatic complaints’, ‘Anxious/depressed’ (these first three scales are summarized under ‘Internalizing scale’), ‘Delinquent behaviour’, ‘Aggressive behaviour’ (summarized under ‘Externalizing scale’), ‘Thought problems’, ‘Social problem’ and ‘Attention problems’ (designated as neither ‘Externalizing’ nor ‘Internalizing’). Thirty-three items that could not be assigned to any of these scales are called ‘Other problems’. The sum of all items forms the ‘Total score’. Studies on the reliability and validity of the CBCL have been extensively summarized in the Achenbach manual (27). The CBCL was administered only to the mother, as the parent who usually spends more time with the children. The mother was invited to fill the CBCL, while her child was being submitted to the neurophysiological examination in another room. According to Achenbach (27), we would exclude from the study the patients whose mother omitted more than eight items of the questionnaire.
Statistical analysis
Neurophysiological results
MMN and P300 latencies and amplitudes recorded in the first block were compared among the three groups (migraineurs, TTH patients and CS) by means of one-way
Psychological results
As suggested by Achenbach himself for statistical analysis, we considered the raw scores, which can reflect greater differentiation among non-deviant subjects than T-scores can on these scales (27). Moreover, our analysis was aimed at seeking a correlation between the behaviour characteristics and ERP habituation, whereas a deep investigation of possible psychological disorders, evinced better from the T-scores than from raw scores, was beyond the scope of the present study. The CBCL total scores obtained in the three groups of subjects were submitted to one-way
Correlation analysis
To assess whether there was a correlation between the neurophysiological data, the ERP habituation in particular, and the behaviour symptomatology of our subjects, we performed a series of correlation analyses between the habituation index of both the MMN and the P300 potentials and the total CBCL scores. If statistical significance had been reached, the habituation index would have been correlated with the CBCL subscores. Pearson coefficients were computed.
Statistical significance was fixed at P < 0.05.
Results
ERP amplitude and latency
Neither the MMN nor the P300 latencies were different among the three groups of subjects (F 2,34 = 2.76, P = 0.07 and F 2,34 = 1.7, P = 0.19 for the MMN and the P300 potential, respectively).
There was no difference in either the MMN or the P300 amplitudes among the groups of subjects (F 2,34 = 0.28, P = 0.76 and F 2,34 = 1.68, P = 0.2 for the MMN and the P300 potential, respectively).
MMN and P300 latencies and amplitudes in the first block are shown in Table 2.
Event-related potential values (first block)
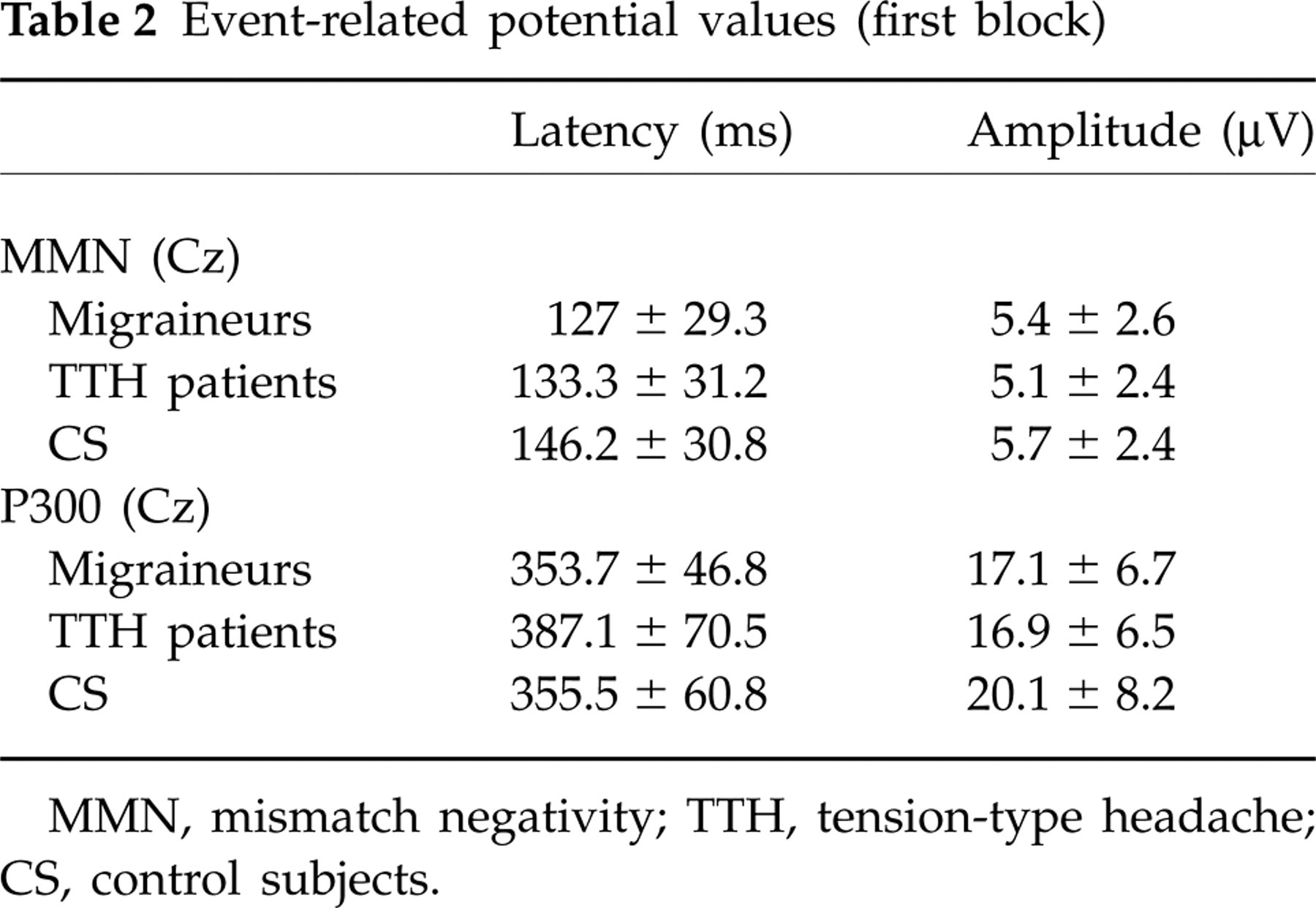
MMN, mismatch negativity; TTH, tension-type headache; CS, control subjects.
ERP habituation
In all groups of subjects, neither the MMN nor the P300 latencies were different between the first and the third blocks (P > 0.05)
In CS, the MMN and P300 amplitudes were significantly lower in the third than in the first block (P = 0.02 and P = 0.04 for the MMN and the P300 potential, respectively). In both migraine and TTH patients, the MMN and P300 amplitudes recorded in the first block did not differ from those obtained in the third block (P > 0.05).
When ERP amplitude habituation was compared in the three groups of subjects, a significant interaction block X group (F 4,105 = 3.58, P = 0.008 and F 4,105 = 2.75, P = 0.03 for the MMN and P300 amplitude, respectively) was found, meaning that the block repetition produced a significantly different effect on the ERP amplitudes of the groups.
An effect of group was found when the habituation indices of both the MMN and the P300 response were compared (F 2,34 = 3.6, P = 0.008 and F 2,34 = 6.71, P = 0.002 for the MMN and the P300 potential, respectively). The post hoc analysis revealed that both the MMN and P300 amplitudes recorded in the third blocks were significantly lower in CS than in migraineurs and TTH patients (P < 0.05). This result shows a higher habituation in CS than in migraine and TTH patients (Fig. 2).

The histograms show the intergroup difference of both the mismatch negativity (MMN) and P300 habituation indices. Note that both the MMN and P300 habituation indices are lower in control subjects (CS) than in migraineurs and tension-type headache (TTH) patients, meaning that the event-related potential amplitude decrease in the third block is higher in CS than in migraine and TTH subjects.
Psychological results
The CBCL total score was not different among the three groups of subjects (F 2,34 = 1.21, P = 0.31).
A significant effect of group was found when we compared the Internalizing and Externalizing scale subscores (F 2,105 = 9.29, P = 0.0002). The difference was due to the Internalizing score, which showed a significant intergroup difference (F 2,34 = 8.77, P = 0.0005), whereas the Externalizing score did not (F 2,34 = 1.79, P = 0.18). Post hoc analysis showed that TTH patients had a significantly higher value than CS (P = 0.008), whereas the Internalizing subscore in migraineurs was intermediate between TTH patients and CS. No interaction group X score was found (F 4,105 = 1.51, P = 0.23). CBCL scores are shown in Table 3.
CBCL values (mean ± standard deviation)
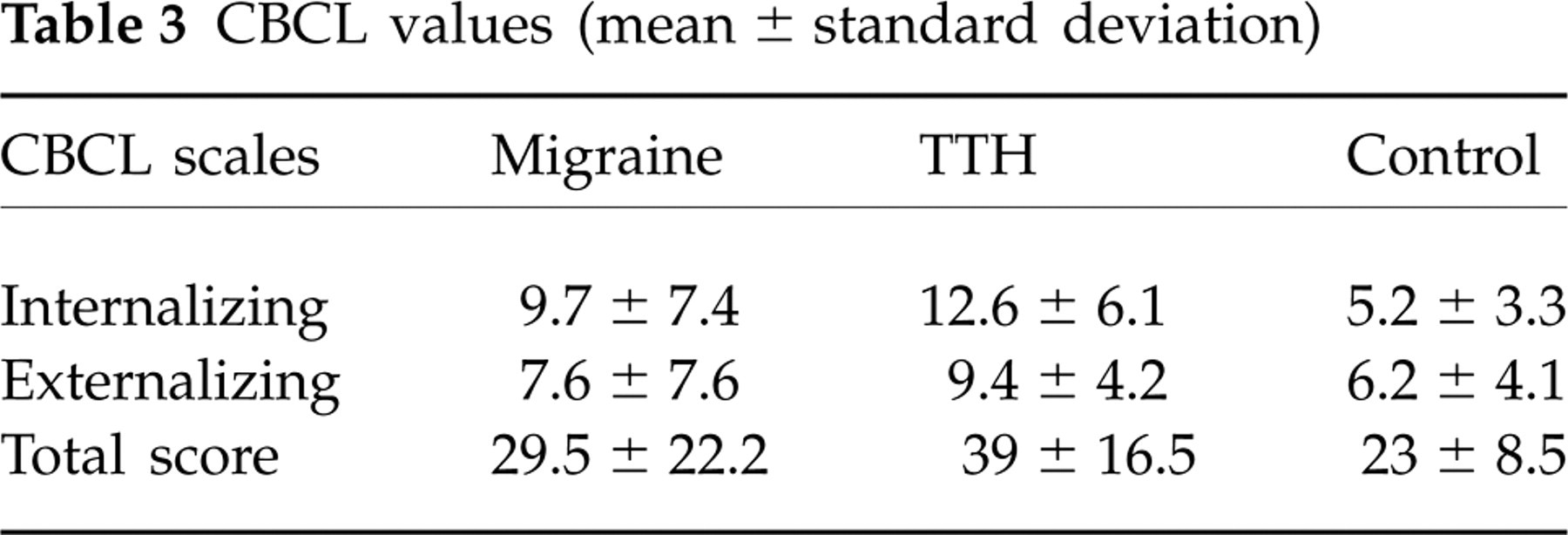
CBCL, Child Behaviour Checklist; TTH, tension-type headache.
Correlation analysis
In migraine patients, a significant positive correlation was found between the P300 habituation index and the CBCL total score (r2 = 0.31, P = 0.01), meaning that patients with the most reduced P300 habituation showed the worst CBCL scores (Fig. 3). In particular, in Fig. 3 two patients showed a P300 amplitude potentiation in the third block. It is noteworthy that both patients had had their headache onset > 3 years. A significant positive correlation of the P300 habituation index was also found with both the Internalizing (r2 = 0.24, P = 0.03) and Externalizing (r2 = 0.36, P = 0.008) scores (Fig. 3).

Correlations between the P300 amplitude in percentage recorded in the third block, considered as habituation index, and the Child Behaviour Checklist scores (total, Internalizing scale, Externalizing scale) in migraine children.
No correlation between the P300 habituation index and the total CBCL scores was found in either TTH patients (r2 = 0.13, P = 0.3) or CS (r2 = 0.29, P = 0.11) (Fig. 4).

Correlations between the P300 amplitude in percentage recorded in the third block, considered as habituation index, and the Child Behaviour Checklist total score in tension-type headache patients and in healthy children.
The MMN habituation index did not correlate with the total CBCL scores in any group of subjects (r2 = 0.19, P = 0.07, r2 = 0.01, P = 0.76, and r2 = 0.29, P = 0.11 for migraineurs, TTH patients and CS, respectively).
Discussion
The main results of the present study are: (i) the reduced habituation of both the MMN and P300 potentials in children with migraine and TTH, compared with healthy subjects, and (ii) the correlation between the P300 habituation deficit and the behavioural symptomatology in migraineurs, but not in TTH patients.
ERPs in patients with primary headache
The far better known neurophysiological characteristic of the primary headaches is represented by the reduced EP habituation. This phenomenon has been more often demonstrated in migraine patients by using long-latency ERPs, thought to reflect complex cognitive functions and largely influenced by the subject's attention (16, 17, 19, 23, 32). Although short-latency processes, such as the P50 auditory EP gating (32, 33) and the somatosensory EP recovery cycle (34), have also been found abnormal in migraineurs, there is still the possibility that the habituation deficit in these patients is the marker of their inability to divert their attention from repetitive incoming stimuli (16). Whereas in adults the ERP habituation deficit is considered specific to migraine, it being absent in non-migraine headaches (17, 19, 23, 24), in the paediatric age group there is substantial disagreement among different studies. Indeed, whereas Evers et al. (16) showed reduced visual P300 habituation in children with migraine, but not in those with TTH, Oelkers-Ax et al. (26) failed to show any visual EP habituation difference between migraineurs, TTH patients and CS. Lastly, Buodo et al. (25) have even shown that migraine children had a higher P300 habituation compared with healthy controls. In our patients, we found significantly reduced habituation of both the MMN and the P300 response compared with CS. There are two main original conclusions to be drawn from this result. First, in the same subjects we examined the habituation not only of a longer-latency ERP, such as the P300 response, whose amplitude depends on the subject's attention, but also of the MMN, which is a pre-attentive component (28). Our result suggests that the habituation deficit observed in headache patient is independent of attention, thus it probably reflects abnormal brain excitability. There is disagreement about the excitability of the cerebral cortex in migraine (13). Indeed, whereas brain hyperexcitability has been proposed to explain most neurophysiological abnormalities observed in migraine (34–37), according to other authors cerebral cortex hypoexcitability could cause the reduced EP habituation (12, 33, 38, 39). Second, the decreased ERP habituation was found in both migraine and TTH patients. Subjects with migraine in their first-degree relatives may show a habituation deficit as migraineurs (40). However, it is unlikely that this could have determined the ERP reduced habituation in our TTH children, since only three out of our 10 TTH patients had a first-degree familial history of migraine. Our findings suggest that in the paediatric age group the abnormal brain excitability represents a common background for both migraine and TTH, thus supporting the idea that in children migraine and TTH are not distinct entities, but two aspects of the same spectrum of benign headache (3, 41, 42). Whether this result may be extended also to adults cannot be decided from our present results, but this point deserves further investigation in adult migraineurs and TTH patients.
Psychological factors in children's primary headaches: do they co-vary with the abnormal brain excitability?
In our patients, the CBCL Internalizing scale score was worse in headache patients than in CS. This confirms previous results in highlighting the role of Internalizing disorders in children with primary headache (41, 43–45). On the other hand, the antisocial and aggressive behaviour (Externalizing) scales identified no more difference between patients and healthy children, showing globally adequate behavioural patterns on externalization. In previous literature there is no agreement on this point, since in children with headache externalizing disorders have been found in one study (46), but not in others (44, 45).
In migraine patients, the CBCL total score showed a positive correlation with the P300 amplitude modification in the third block, assumed as a habituation index. In the same patients, significant positive correlation was found between the Internalizing and the Externalizing scale scores and the reduced P300 habituation. If we accept that the P300 habituation deficit is an expression of abnormal brain excitability, our results mean that migraineurs with the worst CBCL scores have also the most abnormal cerebral cortex excitability. No correlation was found between the P300 habituation index and the CBCL total score in TTH patients and CS. Moreover, no correlation between the MMN habituation index and CBCL scores was found in any group of subjects, even in migraineurs. The discrepant results between the P300 and MMN correlations in children with migraine may be attributed to the pre-attentive character of MMN. Indeed, it is conceivable that the reduced MMN habituation is exclusive expression of altered excitability at neuronal level, independent of higher cognitive influences, whereas several factors, including cognitive and psychological ones, concur with the abnormal cell function in determining the P300 habituation deficit.
Only in migraineurs was a correlation between psychological symptomatology and neurophysiological abnormality observed. This finding may relate to the clinical difference between migraine and TTH (see the ICHD-2 diagnostic criteria, 2004) and to the pathophysiology of migraine. Given that in the present study abnormal brain excitability was found in both paediatric migraine and TTH, the hypothesis can be made that the concomitance of a certain psychological symptomatology is crucial in addressing the phenotypic expression. In other words, in childhood abnormal brain excitability is necessary but not sufficient per se to explain the migrainous characteristics of a headache. Our results suggest that in the migrainous syndrome, with a typically more severe clinical aspect than TTH, the psychological characteristics may have a pathophysiological role. However, caution in the interpretation of our findings is also needed. Indeed, our analysis has shown only a co-variation between neurophysiological data and behavioural symptomatology, preventing us from excluding the possibility that in our migraine patients the aforementioned correlation is a consequence, instead of a cause, of their type of headache.
Methodological limitations
This study has a number of limitations that must be taken into account in interpreting the data: (i) our results derive from children who were clinically referred to our third-level centre for the treatment of primary headache, and they may not be representative of the general population; (ii) the CBCL allows the psychological characteristics of children, not a clinical diagnosis. Further studies are warranted to investigate the psychological conditions using psychiatric or personality interviews; (iii) the CBCL is based on parents' reports, with their subjective point of view. Comparing multiple sources of information may be useful in forming a complete picture of the clinical condition; (iv) our correlation analysis is based on a small sample of subjects, making type II errors possible. Moreover, in the correlation between the neurophysiological results and the CBCL scores of our migraine patients some outliers are present that may contribute to reaching a significant result. This means that our results indicating co-variation between brain excitability and behaviour symptomatology have to be confirmed in a larger population of migraine patients. However, it should be noted that the main outliers were represented by two patients with a P300 amplitude potentiation in the third block, in whom the headache onset was > 3 years. This allows us to hypothesize that increasing the number of patients with a long story of migraine might make the correlation more solid; and (v) lastly, our analysis cannot establish a hierarchic relationship between cerebral cortex excitability and the emotional functioning in our migraineurs, but is limited to merely showing co-variation between these important aspects of the migrainous disease.
Conclusions
This is the first study in which a correlation between psychological symptomatology and neurophysiological features has been found in migraine children. In our opinion, this may be a promising way to solve the long-lasting question about the relative importance of psychological/environmental and organic/genetic factors in migraine pathophysiology. Our results confirm that migraine is probably a multifactorial disease and suggest synergy of both psychological and neurophysiological elements in its pathophysiology.