
Abstract
The aim was to assess whether women suffering from migraine are at higher risk of developing hypertensive disorders in pregnancy. In a prospective cohort study, performed at antenatal clinics in three maternity units in Northern Italy, 702 normotensive women with singleton pregnancy at 11–16 weeks' gestation were enrolled. Women with a history of hypertensive disorders in pregnancy or presenting chronic hypertension were excluded. The presence of migraine was investigated according to International Headache Society criteria. The main outcome measure was the onset of hypertension in pregnancy, defined as the occurrence of either gestational hypertension or preeclampsia. Two hundred and seventy women (38.5%) were diagnosed with migraine. The majority (68.1%) suffered from migraine without aura. The risk of developing hypertensive disorders in pregnancy was higher in migraineurs (9.1%) compared with non-migraineurs (3.1%) [odds ratio (OR) adjusted for age, family history of hypertension and smoking 2.85, 95% confidence interval (CI) 1.40, 5.81]. Women with migraine also showed a trend to increased risk for low birth weight infants with respect to women without migraine (OR 1.97, 95% CI 0.98, 3.98). Women with migraine are to be considered at increased risk of developing hypertensive disorders in pregnancy. The diagnosis of primary headaches should be taken into account at antenatal examination.
Introduction
Migraine is a recurrent primary headache disorder (1), representing one of the commonest neurological disorders in adult women (2). According to the American Migraine Prevalence and Prevention study, the 1-year prevalence of migraine in women is about 17.1%, rising to 24.4% during childbearing years and decreasing after menopause (3).
Gestational hypertension (GH) and preeclampsia (PE) are disorders occurring during pregnancy. They usually start after 20 weeks' gestation and are associated with poor outcomes. PE complicates 3–7% of all pregnancies and is a leading cause of maternal and perinatal morbidity and mortality worldwide (4).
Migraine and PE share some common pathophysiological features related to vascular function, platelet activation and enhanced clotting.
A number of studies have shown weak evidence of the positive association between headache and PE in pregnancy (5–15). The main methodological limitations of the above studies were the use of retrospective designs and/or the lack of standardized criteria for the diagnosis of migraine and PE. Thus, we conducted a prospective, multicentre, cohort study to investigate whether the presence of migraine is associated with an increased risk of the onset of hypertensive disorders during pregnancy.
Methods
From March 2004 to December 2006, women attending antenatal booking at three maternity units in Northern Italy were enrolled. We included Caucasian women with singleton pregnancy at a gestational age of 11–16 weeks. Women with a positive history of GH or PE, a history of recurrent abortions (three or more), chronic hypertension, diabetes or any other chronic systemic disorder were excluded.
Women were interviewed by three researchers who had previously been trained in headache diagnosis according to the International Classification of Headache Disorders criteria (ICHD-II) (1). As part of the training, the three researchers applied the criteria to selected cases of migraine to gain practice in asking questions and reporting the answers. A semistructured questionnaire was also used to facilitate the interview and the collection of data. Details about the questionnaire are reported in a previously published paper (14). During the interview a clinical examination was also performed and the following information was recorded: age, years of education, parity, family history of PE and other hypertensive disorders, and smoking habits. Body mass index (BMI) was also calculated. All women eligible for the study were then followed up.
The diagnosis of migraine was based on ICHD-II criteria. Attacks and/or headache lacking one of the features needed to fulfil all the criteria for migraine with aura or migraine without aura were coded as ‘probable migraine’. Since some of the patients suffering from migraine with aura could also present attacks of migraine without aura, for the purposes of the current study we diagnosed only prevalent cases of migraine. All the diagnoses of migraine were independently reviewed by a senior researcher (G.A.). In case of disagreement, consensus was reached by discussion.
The diagnosis of GH was made if the patient had been normotensive before becoming pregnant and had a blood pressure (BP) of ≥ 140/90 mm Hg after 20 weeks' gestation, measured at least twice and at least 6 h apart. PE was diagnosed if hypertension associated with significant proteinuria ≥ 300 mg in a 24-h urine specimen occurred after 20 weeks' gestation, in previously normotensive and non-proteinuric women (16).
The primary outcome of the study was the onset of hypertension in pregnancy, defined as the occurrence of either GH or PE. Secondary outcomes were: (i) preterm delivery, defined as a birth occurring before 37 completed weeks of gestation; (ii) low birth weight, defined as the weight at birth < 2500 g; (iii) small for gestational age, defined as a newborn whose weight is below the 10th centile for their gestational age (17) in the absence of congenital malformations or chromosomal abnormalities, recent cytomegalovirus infection, or maternal substance or alcohol abuse; (iv) fetal losses, defined as spontaneous interruption of pregnancy. The exposure was migraine.
The information about outcomes was directly collected at the time of delivery or afterwards, through medical charts review. Data on BP and urinalysis were gathered at each antepartum evaluation, as standard of care in our region. Indications for any medical/surgical intervention (antihypertensive treatment, caesarean section, dilation and curettage, induction of labour, etc.) were collected from hospital diaries. All data were carefully checked at the post-partum interview, which was conducted 6–10 weeks after the delivery, either directly or by telephone.
Information on changes in headache pattern and drug intake, namely triptans, was also collected, at that time with specific questions and trusting in the woman's report. All patients diagnosed as migraine sufferers were instructed to record migraine attack and analgesic use in a personal diary. A ≥ 50% reduction in the number of attacks was classified as an improvement and complete cessation of attacks as a remission, whereas a migraine worsening was defined as an increase of medication in pregnancy (either painkillers and/or triptans).
The protocol was approved by the Local Ethics Committees in October 2003 and written consent was obtained from each subject after being informed about the study and before participation.
Statistical analysis
The following considerations were taken into account to estimate the sample size. The prevalence of migraine during reproductive age in women has been estimated to be around 25% (3), and a further 5% should be added also to consider women suffering from probable migraine (18). Prevalence of hypertension in pregnancy has been estimated to be 10% (19). According to the previously mentioned studies (5–15), the risk of hypertension in pregnancy in women with migraine has been shown to be higher compared with that observed in women not suffering from migraine. However, these estimates ranged widely among these studies (20). Our hypothesis was that hypertension in pregnancy in women with migraine was at least twice as high as that observed among non-migraineurs. To have 80% power to detect an odds ratio (OR) of 2.2 at the 5% level given a risk of hypertension in pregnancy in women not suffering from migraine of 8% and a ratio of migraine to no migraine of 3:7, we needed a sample size of 643. To allow for patients lost to follow-up or failing to meet the inclusion criteria we decided to enrol 15% more patients, for a total sample size of 739. Association between migraine and hypertensive disorders in pregnancies was expressed as OR from logistic regression model in STATA, release 9.0 (StataCorp LP, College Station, TX, USA). Furthermore, 95% confidence intervals (CIs) around the point estimates were also reported as well as the P-values. A result was considered statistically significant if its P-value was < 0.05. In addition, to take into account possible differences in the distribution of potential confounding variables across the women with or without migraine, multivariate logistic regression analysis was used to provide adjusted OR estimates. In the multivariate analysis we considered only those covariates that had a P-value < 0.1 on univariate analysis.
Results
In total, 753 women were interviewed, 11 of whom were not eligible (they did not fulfil the inclusion criteria). Seven women chose to terminate pregnancy after prenatal diagnosis and 33 were lost to follow-up. Of the 40 women not completing the study, migraine was diagnosed in 14 cases (35%). Thus, data were available for 702 women (Fig. 1), although in two patients information on birth weight was not obtained.

Flow chart of women enrolled in the study.
Migraine was diagnosed in 270 women (38.5%), of whom 184 suffered from migraine without aura, 36 from migraine with aura and the remaining 50 reported a ‘probable migraine’. For statistical purposes the women in the latter group were included in the migraine group.
There was disagreement about the diagnosis of migraine between junior and senior researchers for 11% of the women. In most cases the disagreements were attributable to uncertainty in diagnosis between probable migraine and probable tension-type headache. The senior researcher found additional and alternative diagnostic criteria looking at personal medical charts. When such data were not sufficient to clarify the diagnosis (3% of cases), a balanced mix between the two hypotheses was chosen.
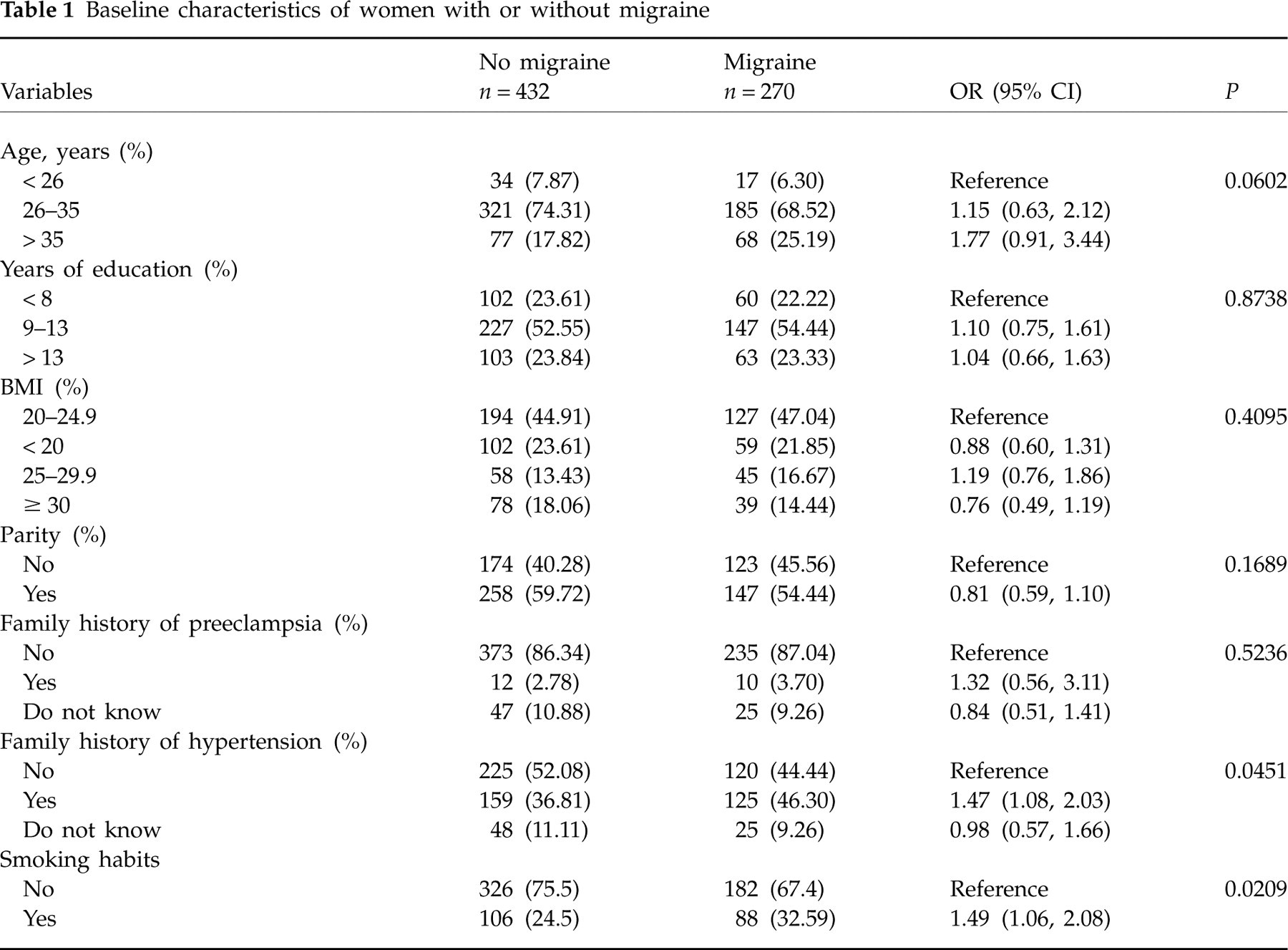
Women with or without migraine did not differ in terms of distribution of age, years of education, BMI or parity (Table 1). Although 10% of all the women interviewed could not answer the question about their family history of hypertension (11% among migraineurs and 9% among non-migraineurs), family hypertension (in either first- or second-degree relatives) was found to be more frequent in women with migraine compared with those with no migraine (46% vs. 37%, respectively). The former also showed a higher rate of smokers (33% vs. 24%).
Baseline characteristics of women with or without migraine
Thirty-seven women (5.2%) experienced the onset of hypertension in pregnancy. GH was diagnosed in 25/702 (3.6%) women in the cohort, and PE in 12 cases (1.7%). Women with migraine had a higher incidence of hypertension in pregnancy (9.1%) compared with those without migraine (3.1%). The unadjusted OR for developing a hypertensive disorder of pregnancy in women with migraine compared with those with no migraine was 3.14 (95% CI 1.57, 6.28). On multivariate analysis, the association between migraine and the onset of hypertension in pregnancy remained statistically significant after adjusting for age, family history of hypertension and smoking (OR 2.85, 95% CI 1.40, 5.81) (Table 2).
Results according to primary and secondary outcomes

∗Adjusted for age, family history of hypertension and smoking habits.
†The figures do not total 702 because 17 women had spontaneous abortion and therefore were not considered in the analysis.
On univariate analysis, the OR for GH in migraineurs compared with non-migraineurs was 3.00 (95% CI 1.30, 6.88, P = 0.0079). For PE the OR was 3.21 (95% CI 0.96, 10.76, P = 0.050).
In women with migraine with aura, the onset of hypertensive disorders in pregnancy (4/36, 11.1%) was similar to that in women with migraine without aura (19/184, 10.3%). However, the former showed an increased prevalence of PE (2/36, 5.9%) with respect to the latter (5/184, 2.9%).
Migraine was not statistically associated with any secondary outcomes, although the risk of low birth weight was found to be higher in women with migraine compared with the risk in women with no migraine (6.8% vs. 3.6%, respectively, OR 1.97, 95% CI 0.98, 3.98).
Furthermore, among migraineurs 167 women (68.8%) reported either a disappearance (23 cases) or an improvement during pregnancy (144 cases), whereas in the remaining 97 women (31.2%) the migraine symptoms remained unchanged or worsened. Women whose symptoms did not change or worsened showed an increased risk of developing hypertensive disorders in pregnancy (P = 0.001) (Table 3). Persistence of headache (either unchanged pattern and/or worsening) was similar in women with migraine without aura (70/180, 38.9%) and in those with migraine with aura (12/35, 34.3%). The majority of women did not treat migraine attacks during pregnancy. Paracetamol was the first-line drug, as recommended. Five cases reported the use of triptans at least three times during pregnancy.
Relationship between course of migraine in pregnancy and onset of hypertensive disorders
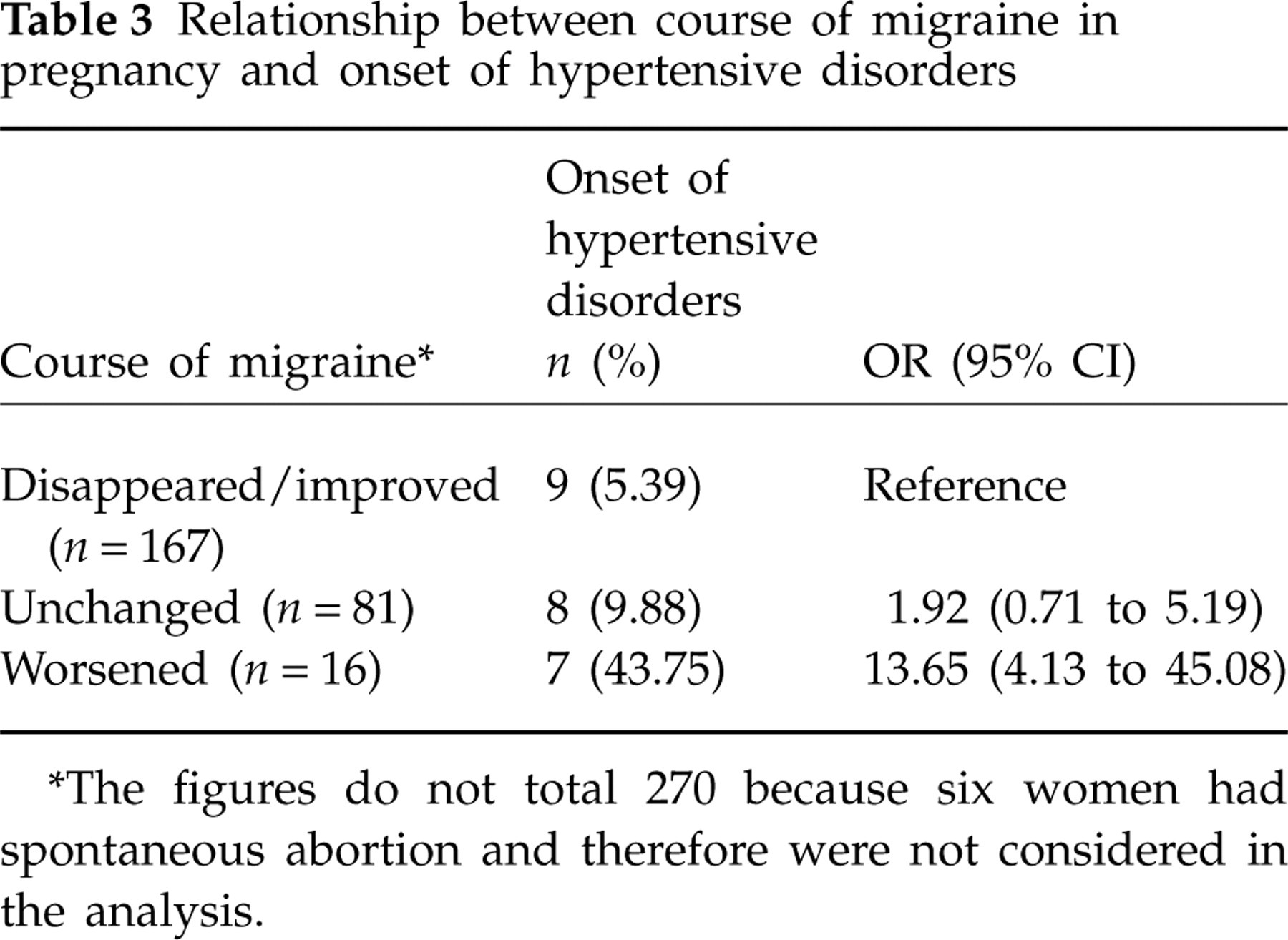
∗The figures do not total 270 because six women had spontaneous abortion and therefore were not considered in the analysis.
Discussion
The hypothesis that migraine could be a risk factor for hypertensive disorders in pregnancy has been assessed in a number of studies (5–15). However, due to their methodological weaknesses these studies have provided weak evidence of the association between migraine and onset of hypertension in pregnancy.
This prospective cohort study, in which standard criteria were used, has shown that a positive personal history of migraine represents a risk factor for the development of hypertensive disorders in pregnancy, in previously normotensive women. Migraine increases almost threefold the odds of developing gestational disorders, i.e. either hypertension or PE. Thus, it appears that migraine may be a risk factor comparable in magnitude to other identified risk factors such as older age, obesity and a family history of hypertension (21).
However, this study has some limitations. Despite its large sample size, the number of events was small and did not allow us to perform separate analyses for the risk of PE, which is considered to be an interesting clinical outcome. Another limitation concerns the influence of possible confounding variables, which were not measured in this study. For example, data on thrombophilia, which is strongly associated with severe PE (22), were not gathered.
Along with the development of hypertensive disorders in pregnancy, women with migraine may be at higher risk of delivering low birth weight infants. The use of sumatriptan, a vasoconstrictive agent used for migraine attacks, has been hypothesized as possibly influencing birth weight (23). In our series, however, such a drug was seldom used, and differences in birth weight were not statistically significant.
Although migraine is no longer considered a vascular disorder, epidemiological studies have shown a lifelong association with ischaemic stroke, namely in women of reproductive age (24, 25). This seems to apply preferentially to women suffering from migraine with aura. Our study, however, lacks the power to detect different outcomes of pregnancy between migraine with and without aura.
Other studies have reported that women developing hypertensive complications during pregnancy are at increased risk of hypertension, stroke and coronary heart disease later on in life (19, 26). It could therefore be hypothesized that migraine and GH and/or PE share some characteristics that may increase the lifelong risk of ischaemic disorders. From a biochemical point of view, there are vascular disturbances occurring in both clinical conditions, such as platelet hyperaggregation (27, 28), reduced magnesium availability (29, 30) and decreased prostacyclin production (31, 32).
About 38% of subjects studied here suffer from migraine, a prevalence that appears higher than reported so far in the literature. We believe that this prevalence is not the result of selection bias, as the subjects were recruited from the general population. Rather, we think that the finding is compatible with the age range of the women and with the White ethnicity of the population (3). On the other hand, a prevalence of migraine similar to that found in our study has previously been reported (33).
From a clinical point of view, it is noteworthy that among migraineurs those whose headache did not improve during pregnancy were at higher risk of developing hypertension than those experiencing migraine relief. Although such a result could be usefully exploited in clinical practice as a predictor of the onset of hypertension in pregnancy, these data have to be interpreted cautiously because of their retrospective collection. However, there is general consensus that migraine symptoms are normally relieved in the second and third trimesters (34, 35), and such improvements refer to hormone/opioid production from the placenta (36). In migraine patients who do not experience such relief it is possible to speculate that the lack of metabolic and vascular adaptations in the maternal body account for an uneventful pregnancy.
In conclusion, women with migraine should be considered at increased risk for the development of hypertensive disorders in pregnancy. The diagnosis of primary headaches should therefore be taken into account on antenatal examination.