
Abstract
Somatization, anxiety, depression and personality disorders are common features of many patients with chronic headaches. Intensive short-term dynamic psychotherapy (ISTDP) is a brief therapy method developed specifically to treat patients with this cluster of somatic problems, symptoms and maladaptive behaviours through focusing on how the patient handles emotional experiences. It also contains a direct method of assessing the somatic discharge pathways of both emotions and anxiety, thus allowing direct observation of somatization in the case of many chronic headache sufferers. In this review, we summarize the extant literature on emotional factors in headache, review the evidence for short-term dynamic therapies in somatic problems and describe the assessment and treatment method of ISTDP we use routinely with chronic headache sufferers.
Introduction
Somatization, herein defined as the translation of emotions into the development or worsening of somatic problems or complaints, is a massive burden on patients, physicians, the healthcare system and society in general, accounting for a major proportion of family physician and specialty medical visits, as well as excessive tests, medications and hospital use (1, 2). Furthermore, it is a major cause of disability, corporate financial loss and probably contributes to early mortality (3, 4).
Although no test exists to confirm whether emotional factors are contributing to an individual's headache, diverse research suggests that many patients with recurrent headache have somatization of emotions as a component of their problems. One study of a general German population found that 19% of people were sufferers of recurrent headaches that were felt to be manifestations of somatization (5). Headache in this sample was the most common presentation of somatization found in their survey. Yucel et al. (6) found that alexithymia, or problems identifying and feeling emotions, was strongly associated with recurrent headache. Wise et al. (7) and Just et al. (8) have described how many headache sufferers are psychologically distressed, but that poor insight into emotional processes or alexithymia prevented the detection and treatment of these factors. Just et al. went further to state there is a need for the development of specific assessment methods to detect relevant emotional and psychological factors in headache sufferers.
Specifically, headache sufferers have been shown to have difficulty regulating anger (9). Many headache patients tend to turn anger inward towards themselves (10, 11). This effect was experimentally illustrated when migraine patients and controls were subjected to an anger-provoking situation. The migraine patients exhibited significantly less overt anger behaviour and experienced a significantly greater rise in pulse pressure than controls in the anger-provoking situation (12). Nicholson et al. (13), looking at headache patients vs. matched non-headache controls, found that anger turned inward was the most predictive of headache. Almost half of their sample of headache sufferers scored highly on anger-in, compared with only one-sixth of the matched no-headache control group. The internalization of anger and/ or trouble identifying anger has been found in high rates in patients with conditions such as irritable bowel syndrome (IBS), depression and hypertension, which are often comorbid with headache (14).
Although methodological limitations in these studies preclude definitive statements about the causative role of emotions, it is important to develop and research methods to detect somatization and manage it when present in these patients. Historically, somatization has been diagnosed by indirect methods such as history, checklist, speculation or exclusion when other problems are ruled out (15). Similar methods are also used routinely to assess psychological factors in headache patients (16). The limitation of these methods is the high risk of type 1 and type 2 diagnostic error where emotional causative factors are falsely assumed to be present or absent. Hence, physicians have been appropriately hesitant to make this diagnosis, thereby denying patients treatment for this causative factor.
Fortunately, this problem has been partially addressed through the advent of methods that attempt to evaluate directly the patient's physical responses to emotion-focused interviewing (17). These methods, derived from intensive short-term dynamic psychotherapy (ISTDP), constitute an addition to traditional assessment methods by studying the patient's observable responses to emotional activation (18). In the following review we describe this assessment method as it pertains to patients with chronic headaches and report on a case series treated with these methods. A case illustration will be used to highlight the diagnostic and treatment process. Finally, we will review the limitations of this method and the implications of this for medical assessment and management.
Empirical basis for short-term dynamic psychotherapy
Short-term psychodynamic psychotherapy (STPP) methods appear to be efficacious for a broad range of conditions. Leischsenring et al. (19) found it to have robust, lasting effects compared with controls in a 2004 meta-analysis. In the early 1990s two meta-analyses (20, 21) had similar findings, whereas one (22) found it superior only to non-treatment controls and less effective than other psychotherapies. A 2006 Cochrane review (23) found the treatment showed modest to moderate significant effects that were generally maintained in follow-up. This review included randomized controlled trials (RCTs) of diverse conditions including depression, anxiety, personality disorders, IBS, pelvic pain, dyspepsia and urethral syndrome (24–27). In a single uncontrolled case series of refractory headache patients, Barnat found 75.6% reported their symptoms improved or very much improved after five sessions of brief dynamic therapy provided in the context of multidisciplinary care (28). Seventy-three per cent of patients were generally satisfied with the treatment, and 76.7% felt the referral was relevant.
Davanloo's ISTDP in specific has been the subject of 16 clinical studies. Among these are six RCTs, including one studying its effects on immune factors (29), one for pelvic pain/urethral syndrome (27), one for panic disorder (30) and three for personality disorders (31–33). A controlled trial of 77 emergency department patients with medically unexplained symptoms found a 69% (P < 0.001) reduction in emergency visits the year after being provided ISTDP, whereas an untreated control group had a non-significant increase in emergency use (34). Case series research has found ISTDP effective and cost-effective, yielding reduced hospital admissions and physician use with mixed psychiatric samples (35, 36) and reduced hospital days with treatment-resistant depression (37). One case series found significant improvement in chronic back pain (38), whereas another found significant improvement in functional movement disorders as rated by blinded raters (39). The assessment interview for ISTDP has been found effective in reducing symptoms, including somatic symptoms, in a mixed psychiatric/psychosomatic sample (40). Thus, within the limitations of this mixture of case series and RCT research, ISTDP and, more broadly, STPP methods appear effective in patients with conditions that may coexist with recurrent headache (28).
While formal outcome research in ISTDP for headache sufferers is required, the method appeared to be effective in helping patients with chronic headache in a naturalistic study (35). In this published series of consecutively treated psychiatry out-patients, 29 (33%) complained of recurrent unexplained headaches (35, 41). Twenty (69%) were female and the average age was 41 years. Sixteen (55%) had comorbid IBS. They were on a total of 23 psychotropic medications, and seven were disabled from work for an average of 54 weeks. In treatment averaging 19.7 sessions, patients experienced normalization on the Brief Symptom Inventory (42), when ratings went from 1.36 (
Somatic pathways of emotions
Davanloo studied the observable physical and verbal concomitants of expressed emotions in the context of ISTDP therapy with a series of several hundred patients over the past 30 years (43). This set of somatic and expressive patterns is now used clinically as a norm to compare with a patient who may be somatizing rather than experiencing his or her emotions. For example, rage is observed as an internal energy sensation, heat or ‘volcano’, which rises from the lower abdomen to the chest, neck and finally to the hands with an urge to grab and do some form of violence. Guilt about rage is experienced with upper chest constriction or even pain, intense painful feeling with waves of tears and with thoughts of remorse (43). Inspired by Davanloo, others have gone on to replicate his main findings by studying case series (35, 36, 44, 45). Gaillard (46), a noted neuroscientist, and Neborsky (47) among others have made efforts to describe the probable neurobiological correlates of the treatment process including emotional experiencing. This type of case-based, descriptive research is one facet of diverse, ongoing efforts to understand and explain the links between bodily responses, emotions and neurobiological events (48).
The following descriptions of techniques and phenomenology are based on the above-noted case series, which constitute now > 2000 case studies, each with several to dozens of emotional experiencing episodes. Note that the main findings in this research, namely anger being inhibited and directed somatically, parallels that of the above-cited research in anger dysregulation in headache sufferers (9–13).
When and why somatization occurs
When feelings are frightening, conflicted, or deemed unacceptable they generate anxiety and defence mechanisms that act to blanket this anxiety (Fig. 1). This is usually the fate of emotions in children traumatized, abandoned or neglected by loved ones, who then have feelings of love mixed with rage and guilt about the rage. When these mixed feelings are unconscious to the patient, the subsequent anxiety and defences are also outside of awareness or unconscious (49). In essence, the rage or anger is turned inward into somatic symptoms both to protect the other person from the rage and to serve as a form of self-punishment for having the rage to begin with. Thus, the child develops the pattern of turning anger inward and is thus prone to somatic complaints, including abdominal pain, headache, depression, personality problems and other conditions (50). When later life events raise the threat of emotional pain and abuse, the rage is ‘turned inward’ into acute or chronic anxiety and somatization. The other person in the relationship is safe from the rage, but the process exacts a high toll for the adult sufferer through the range of symptoms and behaviours required to contain these emotions (43). As noted above, independent research (9–13) suggests that emotion dysregulation and self-directed anger may be relevant factors in headache sufferers, although one study (10) found no correlations between anger dysregulation and headache severity or frequency. Considering headache sufferers as a group, this remains a possible contributor to symptoms (9–13) that needs to be evaluated on a case-by-case basis.

The relationship between unconscious feelings, anxiety and defences.
Diagnosable patterns of somatization
Videotaped case research has shown that emotions are blocked somatically with at least four main patterns: (i) striated muscle tension, (ii) smooth muscle tension, (ii) cognitive-perceptual disruption, and (iv) motor conversion (51). These patterns are a common cause of ‘medically unexplained symptoms’ in neurology clinics (52).
Unconscious striated muscle tension is a neurobiological pathway that proceeds from the thumb, to the hand, up the arms to the neck, face and head, down to the chest and diaphragm, and finally to the legs and feet. It is observable in the seated patient with hand clenching, sighing and even hyperventilation that the patient does not notice. Coupled with this, tension in the frontal, temporal, parietal and occipital regions can produce head pain in an interview. These patients may present with tension-type headache, dizziness, panic attacks, chest pain, fibromyalgia, other musculoskeletal complaints and chronic pain.
Smooth muscle tension results in acute or chronic spasm of blood vessels, gastrointestinal tract, airways and bladder. These patients may present with cardiovascular phenomena, migraine, IBS, hypertension, urinary frequency and bronchospasm. They often have histories of depression, panic, personality disorders and past sexual or physical abuse. Anxiety in this pathway is observable as abdominal cramps, reflux symptoms, flushing and the development of headache symptoms or sensations of aura in the interview. Thus, smooth muscle tension may be a common underlying factor when one sees irritable bowel symptoms with migraine.
Cognitive perceptual disruption is typically observed as visual blurring, tunnel vision, loss of train of thought, and ‘drifting’, where the patient is temporarily mentally absent from the room. Thus, in an interview these patients report blurry vision and become confused when anxious. These patients may experience pseudoseizures, fainting attacks and hallucinatory phenomena. They have chronically poor memory and concentration and may present for assessment of dementia. They are commonly victims and/or perpetrators of partner abuse, have frequent accidents and have transient paranoia. Most have histories of personality disorders and childhood abuse.
Conversion is manifest as localized or diffuse muscle weakness or paralysis. When conversion is active, the person is not having striated muscle anxiety: they appear and are ‘relaxed’ from this perspective, even though they cannot speak or move a limb, for example. This may be acute, such as in the middle of an argument with a loved one, or chronic when subjected to a longstanding infuriating situation such as war or torture. In an interview, these patients will become visibly physically weak and express that they feel weak in one or other region.
The pathophysiology of each of these pathways and their links to strong emotions have been studied through various types of research (53–56).
The total amount of unconscious anxiety present is distributed over these four pathways. Generally, one pathway dominates at any one time, although the same patient may exhibit different pathways in response to greater or lesser degrees of anxiety. When the anxiety is going primarily to smooth muscle or cognitive perceptual fields, the striated muscles are relatively relaxed since the anxiety is going elsewhere. Thus, the findings of no striated tension plus inability to experience emotions coupled with symptoms and signs described above suggest that the unconscious anxiety is being somatized in these routes. However, such a hypothesis is best confirmed by repeating the test or by symptom reduction over one or more treatment sessions. This finding of an inverse relationship between striated muscle tension and smooth muscle has been noted in research of hypertension (57), asthma (58) and IBS (59). This phenomenon is well known in some patients with conversion (see Table 1).
Diagnosable somatization patterns seen in recurrent headache patients (adapted from Abbass 2005)

Defence patterns
This anxiety tends to activate defence mechanisms. Two of the most important are isolation of affect, and repression. Isolation of affect is the awareness of emotions in one's head without the experience of the emotions in the body—or ‘intellectualizing’. Repression is the unconscious process by which emotions are shunted into the body rather than reaching consciousness at all. For example, strong anger and guilt may directly cause diarrhoea, without the person being aware of the emotion of anger itself.
Experiencing emotions overrides somatization
When feelings are being experienced consciously to some degree, then, by definition, they are not being somatized to that degree at that moment (17). For example, when the somatic pathway of rage is activated, it goes up the body in the opposite direction to the anxiety and somatization. At the point of emotional experience, somatization has temporarily been stopped or reduced. At this time both patient and doctor can see ‘what is left’ and ‘what has improved’ as emotional experience supersedes somatization. This allows one to generate testable hypotheses or inferences about emotional causation through this dynamic process.
‘Physical’ examination of the emotional system (see Table 2)
Since the process of somatization is unconscious to the patient, it is diagnosed based upon objective findings of examination rather than on a patient's verbal report. The patient presenting to the doctor with a headache often believes the problem is caused by physical processes, so the history alone is more likely to lead to physical testing and medical treatments than to an examination of emotional factors.
Examination of the emotional system (adapted from Abbass 2005)
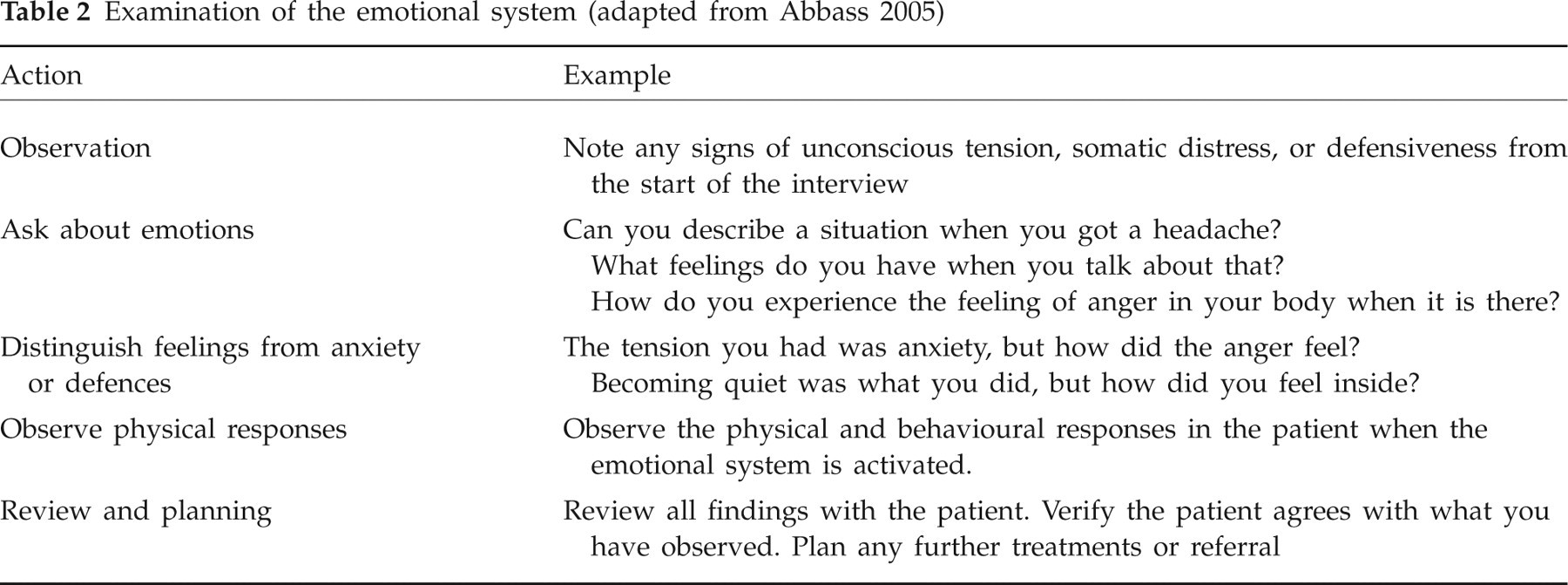
Thus, emotional assessment is much more like performing a physical examination than taking a history. Although there may be clues on history suggesting a patient is somatizing (60), the definitive test is ‘hands on’, observing the patient's direct response to a focused interview process. This assessment progresses from observation to palpation. First, one observes the patient upon coming into the office for the presence of visible unconscious anxiety. Then, in the context of a supportive patient–doctor relationship, one may explore emotionally charged situations. Asking about specific recent events and feelings that were triggered usually mobilizes emotions, giving you and the patient a direct look at how their emotions affect them physically. If a patient is anxious in the office, then one can examine the feelings they experience during the interview.
Interpretation of responses
With this emotionally focused assessment, there will be either a transient increase, decrease, removal of or no change in the somatic symptoms (see Table 3). Removing the symptoms over a few minutes by facilitating emotional experience is the best direct evidence that somatization of these emotions was a factor leading to the somatic symptoms.
Interpretation of responses to emotionally focused assessment (adapted from Abbass 2005)

Review and planning
This interview process is followed by reviewing the findings and management options with the patient. Management options may include another interview, further medical investigations, referral for treatment or follow-up to see the patient's response to the interview itself. If there is no shift in somatic symptoms despite emotional experience, this suggests a physical cause should be sought out.
Case selection
Patients with signs of unconscious anxiety (e.g. hand clenching/sighing, abdominal cramps, mental confusion) in the consultation are prime candidates for this assessment tool. Patients who have histories of anxiety, depressiveness, treatment-resistant headache, other ‘functional’ somatic problems (such as IBS), histories of emotional trauma and personality disorders are good candidates for this assessment method. Patients who appear completely closed to the possibility that emotional factors may be relevant in their case should be handled cautiously to prevent confusion and treatment misalliance. Finally, patients with active depression, conversion, cognitive perceptual disruption and severe personality disorders should be referred for assessment, as the anxiety level must be titrated to prevent exacerbation of these conditions.
Psychodiagnostic evaluation and treatment of a case of chronic daily headache
The principles described above will be illustrated with a case.
The patient is a 52-year-old woman with chronic daily bitemporal headaches and ‘fibromyalgia’, all of which have worsened over the past 4 years since the onset of menopause. Her headaches were present for 25 years prior to worsening and she had intermittent moderately severe headache when she was younger. Over time her headaches have become more frequent, with less severe episodes, but daily, and have not responded to any medications, including migraine-specific medications for abortive therapy and several preventive medications. She has been using a fair amount of analgesic-containing compounds in the past, which ‘took the edge off’ the pain, but in the last year stopped all medication as nothing worked. She has had a history of anxiety and depressive episodes. Her general and neurological examinations were within normal limits. Prior computed tomography of head and magnetic resonance scans failed to yield any intracranial pathology to explain these headaches. She arrived at the assessment interview describing her daily headache symptoms. She described that some episodes are more severe like a ‘pounding, smashing pain’, with nausea and sensitivity to light. She described no aura.
Preliminary diagnostic considerations
This is a typical case of chronic daily headache (CDH) (61). This patient is likely to have had migraine without aura when she was younger, and now has transformed into CDH over years, initially with overuse of analgesics, then without treatment. The history of prior anxiety, affective disorder and ‘fibroymalgia’ are well recognized conditions comorbid with CDH (62).
As the interview began she was visibly tense with hands clenched and with sighing respirations.
Doctor: I notice when you came in that you are tense. Did you notice that?
Patient: (sigh) No not really. I get short of breath sometimes and don't know why. I'm a little nervous about this interview.
Doctor: Do you notice the tension in your muscles?
Patient: I'm tense in the shoulders, my neck, my head and I have a headache. I feel a bit out of breath. (Sighs)
Doctor: Can we look into the feelings you have coming in here, to see what produces this tension?
Patient: I don't know. (Sighs, hands are clenched) I've been on medications for my headaches for many years.
Doctor: If you like we can try to see what generates this tension and how it affects you. (securing consent and collaboration)
Patient: Well, I've been having headaches for 25 years and nobody has been able to help remove them. There is a frustration about that now coming to see you. (A psychiatrist)
Doctor: How do you feel about 25 years of suffering now coming to see another doctor? What emotions tighten you up like this?
Patient: I can't recognize any feelings towards you. (Smiles but sounds somewhat irritated)
Doctor: Right now how did you feel?
Patient: Frustrated … at myself.
Doctor: But is that a pattern, that when you feel angry you become angry at yourself mostly?
Patient: Yeah, I suppose, but I never noticed that.
Doctor: But how do you feel toward me here first? What drives this tension in this moment? Is there a time you had strong anger but it goes at yourself?
With further focus she described a situation of anger towards her husband, but instead of feeling angry she became tensed, self-critical and felt pain in her shoulders and neck that later became a ‘pounding’ headache. From there she went to a situation of anger with her son, in which he was very defiant and she pulled his hair, became nauseated and later developed a severe headache.
Doctor: Can we look into that situation?
Patient: When my son was little, I was infuriated and pulled his hair. (Hands now look strong and the tension has dropped)
Doctor: How does the anger feel in your body? How do you feel right now here when you speak about it?
Patient: My arms just … want to grab … to punch. (Hands have turned to fists)
Doctor: What do your arms want to do with those fists?
Patient: I would punch him … hard.
Doctor: Where do you want to punch?
Patient: On the head … more than once for sure. I was so enraged…. That makes me feel horrible. I felt so bad and never forgot that all these years. (Tears of guilt form)
Doctor: How bad is he hurt with those punches?
Patient: Pretty bad. (More tears) He was a little boy but very stubborn. It was 25 years ago.
Doctor: You have guilt about just this old feeling really. Where does this anger and guilt all come from, because you have a pattern of it all turning inward?
Patient: I wanted to be a perfect mother … and I wasn't … (weeping). It was very hard with four children at that time. My son was so upset when the other children came along … he became so defiant and rejecting.
Doctor: He was rejecting you?
Patient: Yes, he kept pushing me away.
Doctor: Did you ever have that happen before?
Patient: Yes, my father. I was the seventh child, and he was so busy, he never gave me any time. I wanted much more from him. I decided then I would show them more love when I had children. (waves of sadness weeping openly). My mother was too busy too. I felt that lack.
Doctor: Was there any time you wanted more and were rejected?
Patient: Yes, once, my father was sleeping and I went to kiss him and my mother told me to leave him alone. (Sighs)
Doctor: How do you feel toward her?
Patient: Angry. (Sighs again)
Doctor: Do you feel that now again?
Patient: Yes. (Animated and strong arms, rise in energy)
Doctor: How do you feel the anger if you don't let it go to tension? What did that anger want to do if you let it out?
Patient: I want to lash out at him. (Hands move to slapping motion) To slap him.
Patient: Thrusting feeling, to punch him.
Doctor: How much energy is in your arms?
Patient: Three hard punches. (Thrusts her fist forward illustrating the motion)
Doctor: How you feel if you repeatedly punched your father when you wanted affection from him?
Patient: I'd hold him … that's all I wanted. (Sobbing)
This is followed by a global review of what was covered, namely the link between rejection, sadness, anger and guilt about anger producing guilt and tension, as if to hold in the feelings from the past. When these complex feelings arise with her family members, or doctors, the anxiety rises as if the anger would come out. She then becomes tense, self-critical and inhibited, producing a combination of fibromyalgia pain, headache and depressive symptoms. Prior to this session, she had not been aware of the link between the feelings and symptoms. During the interview she clearly noticed the cessation of muscle tension and the headache when the feelings passed through. She left without tension and felt she had a good understanding of this emotional factor and how it impacted on her symptoms. In a 3-month follow-up she noted a significant drop in headache intensity and frequency, coupled with improved relationships with her son and husband.
Limitations and future directions
There are several limitations to note regarding what is presented in this review. First, the empirical support for the model of ‘unconscious’ and ‘emotions’ is limited to detailed analysis of large videotape case series. Because the unconscious mind is not a physical structure to be dissected, we are left to observe its outward manifestations and responses to interviewing. Nevertheless, this assessment method, called ‘unlocking the unconscious’, when applied to certain patients is considered by practitioners and noted researchers as one means to a ‘direct view’ of unconscious emotional operations (63).
Second, emotional factors may be a central cause, a partial contributor or not at all causal in a given patient's headaches, leading to some false positives and false negatives with this assessment approach. We recommend assessing emotional processes directly and making a determination, with the patient, of whether or not these factors play a role in his or her case.
Third, this assessment method generally does require training, although the information herein is enough to allow many clinicians to incorporate elements into a consultation as a part of functional inquiry (e.g. how does anger or stress affect you physically?) and the observation component of the mental status examination. Thus, we provide training in this to all medical undergraduates and residents across all disciplines at our university on an annual basis. The training method used is a combination of videotape workshops, live interviews for referral sources and videotape training with peer supervision (64).
To address the limitations of existing research, the ISTDP model requires formal research as a diagnostic and treatment vehicle as regards headache populations. This assessment interview should be formally researched to determine its sensitivity, specificity and limitations as it pertains to patients with recurrent headache. Its efficacy as a treatment model should be determined with an RCT of a neurologically evaluated and blindly rated sample of patients. Such a study could evaluate the scope of utility, magnitude of effects and the limitations of this as a treatment approach. Finally, a standardized brief assessment interview tool that physicians may use to screen for emotional factors in headache presentations should also be developed, piloted and researched.
Conclusion
Somatization in recurrent headache sufferers is prevalent and taxing—on the patient and loved ones, and the healthcare system and society at large. In some patients it appears a basic difficulty in identifying and experiencing complex feelings can result in or exacerbate the condition. Emotion-focused interviewing can help a physician to determine whether emotional processes are relevant in individual patients. Detected pathology can then become a focus of treatment. When no pathology is found in this system, one can pursue physical investigations with greater yield and more efficient use of often-limited resources.
Finally, although there is case-based and RCT evidence for its effectiveness in treating related populations, ISTDP should be formally researched to determine its role and limitations as a diagnostic and treatment approach for somatization in recurrent headache.