
Abstract
Introduction: The aim of this study was to determine sex specific co-morbidity of migraine and its subtypes migraine without aura (MO) and migraine with aura (MA) with a number of common somatic diseases.
Subjects and methods: In 2002, a questionnaire containing previously validated questions to diagnose migraine and its subtypes as well as questions regarding some somatic diseases was sent to 46,418 twins residing in Denmark and born between 1931 and 1982. The twins are representative of the whole Danish population and were used as such in the present study.
Results: We found that 21, 23 and 12 conditions were co-morbid with migraine, MA and MO, respectively. Co-morbid diseases included previously documented diseases: asthma, epilepsy and stroke as well as new conditions: kidney stone, psoriasis, rheumatoid arthritis and fibromyalgia. MA had more co-morbidities than MO and females more than males.
Conclusions: Migraine occurs in 20–30% of several medical conditions. It should be diagnosed and treated along with the primary disease.
Introduction
In 2007, Stovner et al. (1) established a world-wide map of headache showing that migraine affects 11% of the adult population in the world. Migraine was ranked by the World Health Organization as the 19th of disabling diseases (2) and in Europe the total societal cost was estimated to be €27 billion per year for the 41 million migraine sufferers, indirect costs accounting for almost 90% (3).
Large-scale, population-based studies are required in order to provide reliable evidence for migraine co-morbidity. Conditions that have so far been verified from population-based studies with a consistent positive association to migraine are stroke (4,5), depression (6–9), anxiety disorders (8,10), epilepsy (11), and allergies and asthma (12). Some conditions lack convincing evidence due to conflicting results (13–15) or study designs with insufficient statistical power (16–18). Many conditions have not yet been explored or have only been paid little attention and will need further investigation.
So far, the majority of the studies investigating co-morbidity did not distinguish between migraine without aura (MO) and migraine with aura (MA). MO and MA are both clinically and pathophysiologically separate entities (19–23) and, in several cases, have different co-morbidities. Thus, MA shows significant co-morbidity with stroke (24,25) and suicidal attempt (26) but MO does not. Co-morbidity should, therefore, be analysed in MO and MA separately, if at all possible.
The Danish ‘Twin Omnibus 2002’ was a questionnaire study among almost 35,000 twin individuals, which included questions on somatic disorders and migraine (27). In the present publication, the twin status is disregarded and the material is presented as a random sample from the Danish population, which is acceptable since these twins have been shown to be representative of the whole Danish population with regard to several other diseases (e.g. diabetes (28,29), asthma (30) and mortality (31)). Our very large sample size has the statistical power not only to detect associations linked to migraine in general but also to reveal differences with regard to co-morbidity between males and females and patients with MA and MO.
The aim of the present study was to evaluate the association between a variety of medical disorders and migraine in males and females as well as patients with MA and MO.
Subjects and methods
The study population was based on twin cohorts born between 1931 and 1982 who were enrolled in the Danish Twin Registry (DTR), the oldest and most complete national twin registry in the world (32). The ascertainment of twins has been done in a variety of ways; for the twins enrolled in this study, the Danish Civil Registration System which has registered all persons living in Denmark since 1 April 1968 has been the primary source (27,32,33). A detailed description of the ascertainment procedure can be found elsewhere (32,34). The DTR is validated and representative of the Danish population as a whole (28–31) and with regard to migraine (35).
The ‘Twin Omnibus 2002’ was a questionnaire investigation about several medical disorders, including migraine. One part of the questionnaire asked the following question: Have you ever been told by a doctor that you have or have had one or more of the following disorders: diabetes, osteoporosis, epilepsy, coronary thrombosis, stroke, other thrombosis, hypertension treated with prescription drug, kidney stone, psoriasis, psoriatic arthritis, rheumatoid arthritis, juvenile arthritis, lupus, osteoarthritis, Bechterew’s disease (ankylosing spondylitis), fibromyalgia, other type of arthritis or disease of the connective tissue, hyperthyroidism (Graves’ disease), hypothyroidism (myxoedema), goitre and other diseases of the thyroid diseases? The subjects were also asked whether they ever have had this disorder: low back trouble, neck trouble, whiplash, Scheuermann’s disease, scoliosis, asthma, allergy to dust, pollen or animals, Ménière’s disease or tinnitus.
Self-reported migraine cases were identified based on the following questions: (i) have you ever had migraine? and (ii) have you ever had visual disturbances that lasted from 5–60 min and were succeeded by a headache?
Persons were classified as having migraine if they answered ‘yes’ to question 1. The second question was to determine whether they had MA or MO. MA was defined as subjects answering ‘yes’ to both questions and MO was defined as subjects answering ‘yes’ to question 1 and ‘no’ to question 2. Subjects answering ‘no’ to question 1 were considered healthy. Any questionnaires containing blanks in these questions were excluded for the purpose of the present study.
Validation of the migraine screening questions
Self-reported migraine based solely on question 1 had previously been validated against a clinical interview (36,37). In 1994, the DTR also conducted a similar twin omnibus survey with four questions screening for migraine, including the two questions mentioned above. In order to validate these questions, 1136 twin pairs where at least one twin had answered ‘yes’ to one or more of the four questions were interviewed by telephone (38). The diagnostic criteria of the International Headache Society classification (39) were used to diagnose the twins. Based on the data from the Twin Omnibus 1994 and from the telephone interviews, new calculations made only for our two questions showed that the sensitivity and specificity of question 1 was 76.2% and 85.6%, respectively. The positive predictive value was 75% and the kappa value was 0.615. By adding question 2, the sensitivity, specificity and kappa value was 84.6%, 40.3% and 0.260 for MA and 71.7%, 84.7% and 0.521 for MO. It is, therefore, possible to use question 1 to screen the Danish population for migraine unspecified and question 2 to distinguish between MA and MO. It was not possible to identify subjects with co-occurrence of MA and MO with these two questions. We have, therefore, chosen to group twins diagnosed with both MA and MO in the same group as MA because MA is more genetically determined (40).
Data analysis
The medical diseases were divided into seven categories: cardiovascular diseases, autoimmune disorders, musculoskeletal disorders, thyroid diseases, atopic diseases, audio-vestibular diseases and other diseases. Univariate analysis was conducted for each disease and category, calculating odds ratio (OR) with 99.9% confidence interval (CI). This level was chosen because of the multiple comparisons. Statistical significance was tested by means of Fisher’s Exact Test. P-values < 0.001 were considered significant. We chose not to use Bonferroni correction because many of the diseases are inter-related. P-values < 0.001 are suitable when doing more than 500 comparisons, which greatly exceed the number of tests done in this study. The analyses were furthermore stratified on sex, MA and MO. To control for the clustering within twin pairs, we also made the analysis for a random sample of one twin per pair using the same P-value as cut-off point. All analyses were performed with SPSS v15.0.
Results
Demographics
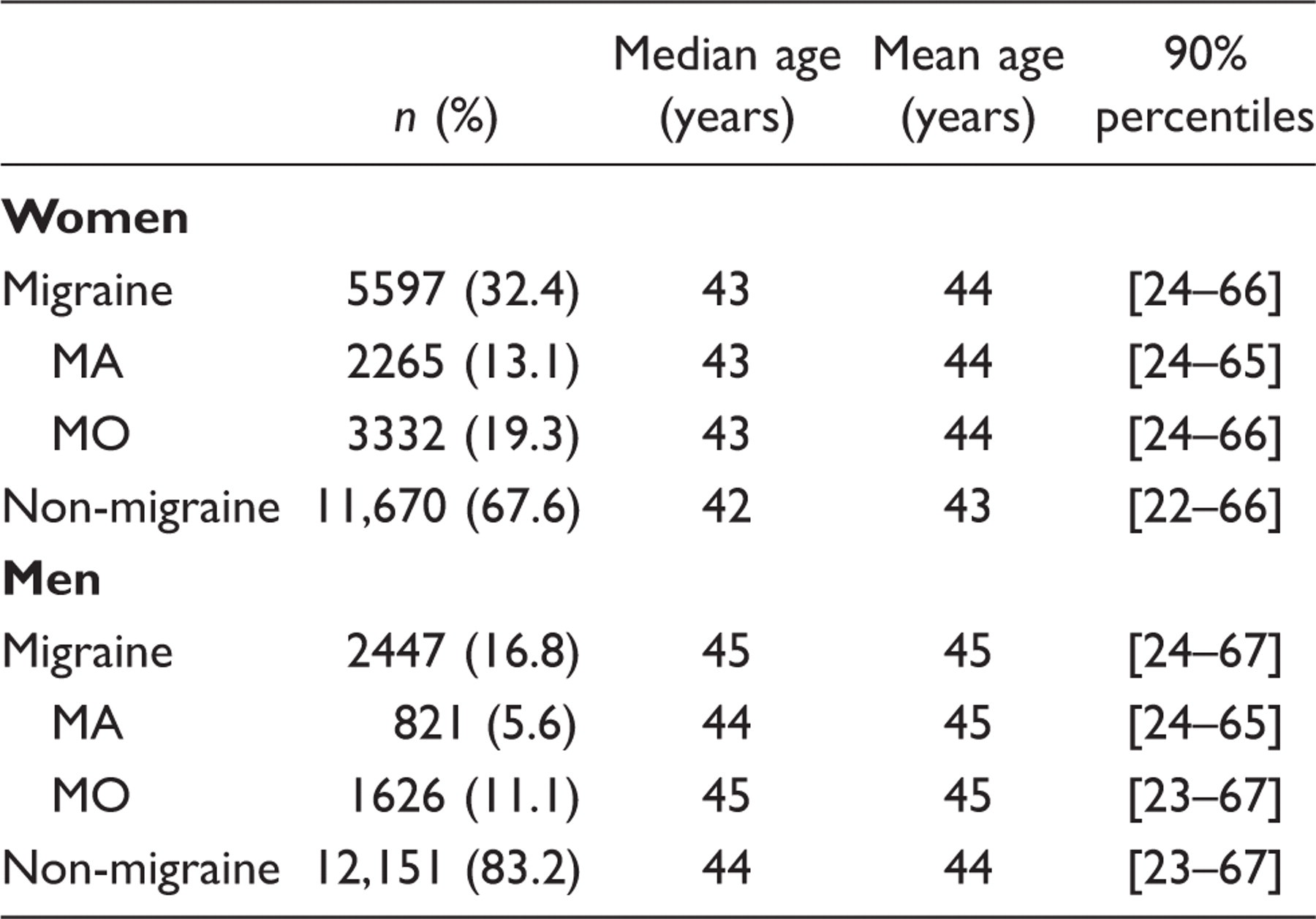
Of all the subjects who returned the questionnaire, 91.2% (n = 31,865) had answered both migraine questions. The rest were excluded due to missing data. Figure 1 shows a diagram of the population according to participation and classification. The number of self-reported migraine cases was 8044. There were more women (69.6%) than men (30.4%) in the migraine group whereas no significant difference was found in the group without migraine. The life-time prevalence of migraine was 17% for men and 32% for women. The median and mean age differed with one year between the migraine group and the group without migraine and with one or two years between men and women. Table 1 presents age and gender characteristics of the migraine group and the non-migraine group.
The response rate of the questionnaire was 75.3%. Of all the subjects who returned the questionnaire 91.2% were included. Inclusion required answering both migraine screening questions. Demographic characteristics of subjects with migraine and without migraine
Migraine co-morbidity
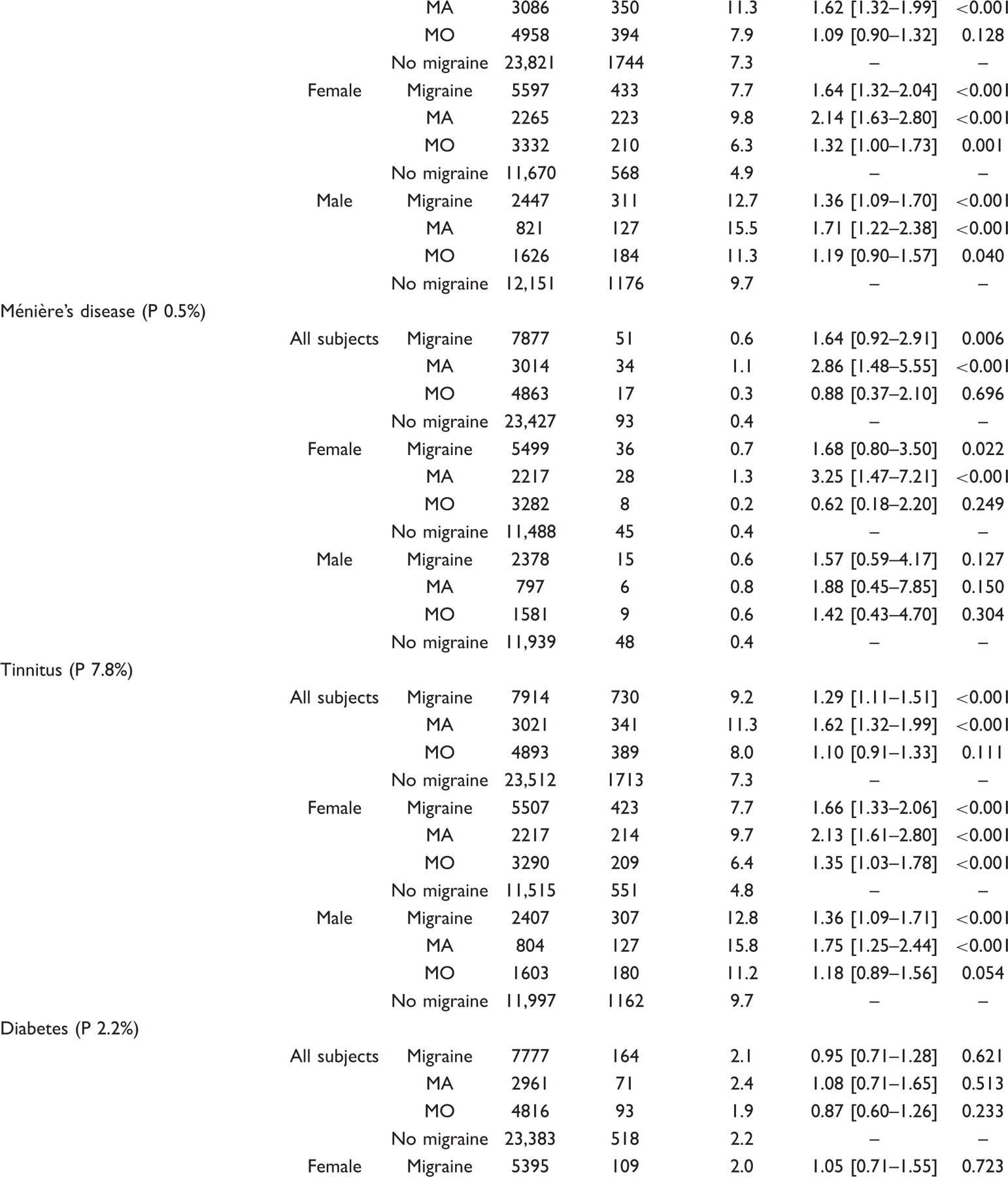
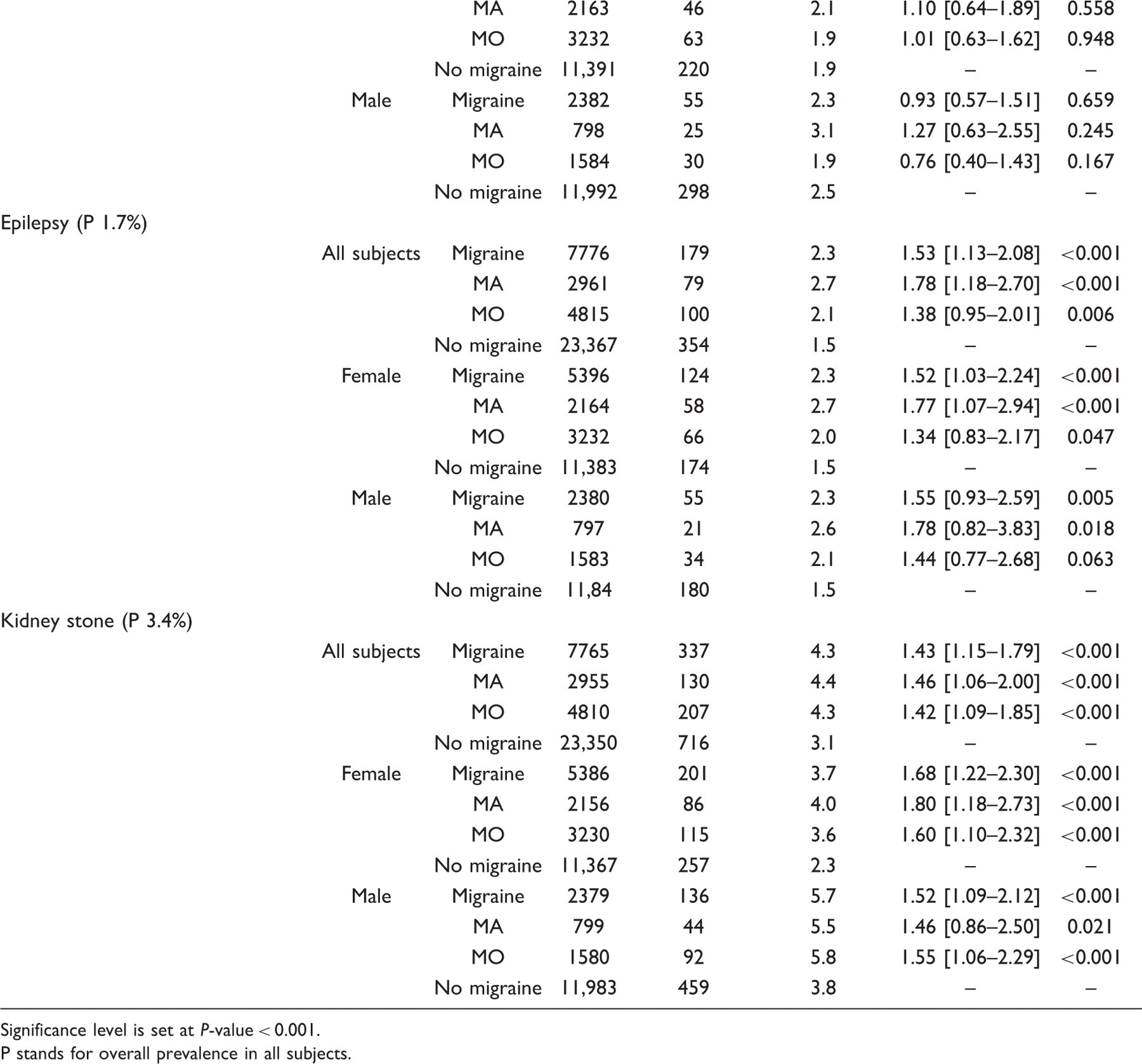
An extensive range of somatic disorders were identified as being co-morbid with life-time migraine and its subtypes MA and MO (Table 2). The number of co-morbidities in migraine, MA and MO, males and females are given in Figure 2. MA had the highest number of co-morbidities (23 out of 30) and males with MO the lowest (5 out of 30). The distribution of odds ratios is given in Figure 3.
Number of diseases co-morbid with migraine and its subtypes migraine with aura (MA) and migraine without aura (MO) for all subjects and the sexes separately. Significance level is set as P-value < 0.001. Number of diseases co-morbid with migraine and its subtypes migraine with aura (MA) and migraine without aura (MO) grouped according to the magnitude of odds ratios. Significance level is set as P-value < 0.001. Co-morbidity of self-reported migraine and somatic medical diseases Significance level is set at P-value < 0.001. P stands for overall prevalence in all subjects.










Analysing co-morbidity for any cardiovascular disease (CVD) showed a significant co-morbidity in total and for female and male subjects separately as well as for migraine, MA and MO. The results in stroke showed, for all subjects, co-morbidity only with MA. This was almost exclusively accounted for by females with MA. Co-morbidity with arterial hypertension treated with prescription medicine pertained to males and females alike and to MA and MO alike.
For any autoimmune disorder, statistically significant co-morbidity with migraine was identified with an odds ratio ranging between 1.3–1.7 in the different groups. Consistently, MA had higher odds ratios than MO and females had slightly higher odds ratios than males. Considerably higher odds ratio was seen in several of the autoimmune subgroups such as lupus, rheumatoid arthritis and psoriatic arthritis.
All musculoskeletal disorders (MSDs) occurred more frequently in migraine patients with odds ratios from 1.7–3.1 and more so in MA than in MO. Low back trouble, neck trouble and whiplash were significantly co-morbid with all migraine subgroups and both sexes.
We found all types of thyroid disease to be co-morbid with migraine and its subtypes. This was almost exclusively accounted for by females since no association could be found for men. The odds ratio was consistently higher for MA (OR 1.8–2.4) than for MO (OR 1.2–1.7).
Any audio-vestibular disorder was co-morbid with migraine in the present study. Co-morbidity was found primarily in MA in both sexes while we could detect associations with MO only in female subjects. For Ménière’s disease, co-morbidity was found for all subjects with migraine or MA and females with MA. Co-morbidity was also found for atopic diseases, epilepsy and kidney stone. When analysing only one twin, the diseases with low absolute prevalence (lupus, psoriatic arthritis, psoriasis, other type of arthritis or diseases of the connective tissue, Scheuermann’s disease, scoliosis, osteoporosis, other diseases of the thyroid gland, epilepsy and Ménière’s disease) were no longer significantly co-morbid.
Diabetes, coronary thrombosis, juvenile arthritis and ankylosing spondylitis were not associated with migraine.
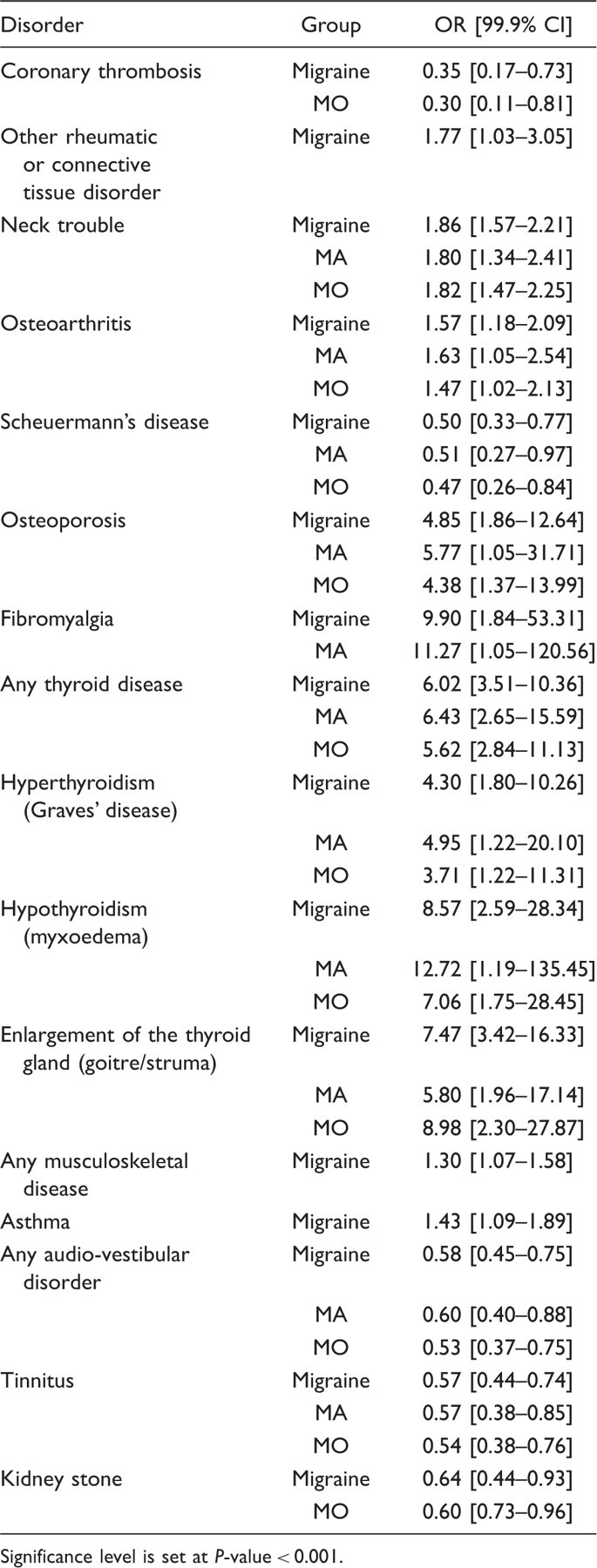
Difference between MA and MO
Co-morbidity of self-reported migraine and a variety of disorders for MA versus MO

Significance level is set at P-value < 0.001.
Difference between female and male patients with migraine
Co-morbidity of migraine and a variety of disorders for female versus male subjects
Significance level is set at P-value < 0.001.
Discussion
The main results of the present study were that self-reported migraine and its subtypes migraine with aura (MA) and migraine without aura (MO) were co-morbid with a number of somatic medical diseases: cardiovascular diseases, autoimmune disorders, musculoskeletal disorders, thyroid diseases, atopic diseases, audio-vestibular disorders, epilepsy and kidney stone.
It was possible in this study to differentiate between MA and MO because of the use of validated diagnostic questions (see Subjects and methods). Furthermore, it was possible to subdivide between men and women and to distinguish between several different diagnostic subgroups because of the large sample size. However, the present study also has weaknesses. The validation of the two questions used to identify migraine cases showed that self-reported migraine was only correct in 74.5% of cases while 25.5% had answered falsely positive to the diagnostic questions about migraine in general. Furthermore, we missed approximately 23.8% of the migraine patients with the questionnaire used. The diagnosis of migraine without aura was reasonably accurate while the diagnosis of migraine with aura contained many false positives. It is apparent that the relatively low kappa value for MA was caused by false-positive answers to the question on visual disturbances. This is also our personal experience from the use of a diagnostic headache diary (41). Thus, the sensitivity was good but the specificity was low for the MA diagnosis. The lack of diagnostic precision, particularly in MA, would, however, tend to diminish the differences between migraine sufferers and normal subjects. Thus, the differences observed in the present study are minimum figures for co-morbidity. However, in rare cases where MA attacks may be classified as stroke/transient ischaemic attack, this may lead to a spurious co-morbidity.
The diagnoses used for co-morbidity in the present study were based on self-reports and are most likely of different validity for the different groups of diagnoses. In several studies (42–45), the validity of self-reported medical somatic disorders has been investigated. For cardiovascular diseases as a group, hypertension and diabetes mellitus the kappa values were high (0.73–0.80; 0.85–0.90) (42,43), for osteoarthritis and rheumatoid arthritis kappa values ranged from 0.30–0.40 (44). The diagnostic uncertainty should be taken into account when judging the results of co-morbidity to migraine in the present study. Thus, some disorder such as stroke, lupus, psoriasis and thyroid disorders are most likely correctly reported whereas musculoskeletal disorders including osteoarthritis are more uncertain.
We found an unexpected high prevalence of migraine; however, similar estimates have been found in other population-based studies (46,47). In our latest interview-based study, we found life-time prevalences of migraine to be 24% for women and 12% for men (37). Furthermore, the Danish twins have repeatedly filled out health questionnaires which may have led to higher report values of migraine. While we cannot rule out the inclusion of false-positive answers, this effect is modest at best.
One might wonder why so many co-morbidities were discovered (Figure 1). Most of the disorders studied were numerically more prevalent in migraine patients than in the non-migraine population. Several hypotheses could be put forward:
That migraine patients over-report co-morbidities in general. This explanation is unlikely for most of the disorders reported. Thus, in 21 out of 30 disorders, subjects were asked whether they had been informed by a doctor that they have had this disease. Furthermore, drug treated arterial hypertension, stroke and coronary heart disease are not likely to be over-reported as they are fairly difficult diagnoses. An external validation of the reporting by migraine patients was given with regard to stroke co-morbidity in the present study. We found an increased prevalence of stroke in female patients with MA. This is precisely the results found in very extensive epidemiological studies that have recently been reviewed (24,25). Any over-reporting by migraine patients is highly unlikely to result in this distinct pattern of co-morbidity. Also, our results concerning a number of other disorders, for which good previous epidemiological population studies of co-morbidity are available, were very similar to the previous results (12). Further adding to the validity of our results, the overall prevalence of the different diseases in our total population is in most cases similar to other studies (48–54). Therefore, our results should hold up also for diseases that have not previously been studied extensively. It could be that patients with chronic disorders have a general susceptibility due to genetic or environmental factors (55) meaning that once one disease is manifested, more may follow. It is possible that one gene is responsible for, or affecting, more than one phenotypic characteristic which could explain some of the associations between migraine and the other diseases. Migraine patients may have other types of headache or pain conditions that are co-morbid with some of the somatic medical diseases tested. It would not be possible to differentiate if the disease was strictly co-morbid to migraine. There may be an information bias related to the fact that, if someone has another medical disorder that has caused consultations and treatments, the likelihood will increase that the diagnosis of migraine has been made. This may be considered a variant of admission-rate (Berkson’s) bias. The degree to which this happens is presumably quite different for different co-morbid disorders. One may expect that, in individuals with suspected cerebrovascular disease, a more thorough examination regarding headaches, and in particular visual and other focal symptoms may have been performed. This may explain the strong association between MA and stroke. Also, persons who have, for example, neck pain or have had a whiplash trauma may have an increased likelihood of being questioned about migraine symptoms, and thereby get the diagnosis. However, coronary thrombosis and diabetes did not show co-morbidity. Therefore, this explanation is not likely to play a major role. Having a medical condition may be stressful and worrying which may increase the likelihood of having migraine. Medicine given for other disorders may provoke migraine (e.g. nitro-vasodilators). Such effects require further investigation.
As shown in Table 3, several conditions were more co-morbid with MA than MO. This difference between the two types of migraine was mainly seen in females. These findings support the view that migraine co-morbidity should be evaluated separately in MA and MO. Furthermore, they support the notion that the two types of migraine most likely have different pathophysiology (22,23).
Cardiovascular diseases (CVDs)
As in previous studies, we found increased frequency in females with MA for stroke (4,56). There was no co-morbidity for coronary thrombosis in keeping with previous studies (5,57). In contrast to our small previous study (58), we found a distinct co-morbidity with arterial hypertension treated with prescription medicine (OR 1.5). Other studies have shown no association to blood pressure (59) or that only the diastolic blood pressure (and not the systolic blood pressure) is elevated in migraine patients (58,60). The conflicting findings may be due to different methodology. Our results are based on drug-treated arterial hypertension whereas a single blood pressure was measured and used for analysis in the other studies (58,60,61).
An increased prevalence was found for a group of ‘other thromboses’ in migraine sufferers where the co-morbidity was highly significant especially with MA (OR 2.4). Due to limited questionnaire information, it was unfortunately not possible to attribute the effect to specific diagnoses within this overall group of other thromboses.
Musculoskeletal disorders (MSDs)
The present study confirms the findings of previous studies regarding associations between migraine and low back pain (62–65). We found a high prevalence of low back pain of 56.6% in the total population and 75.4% in females with MA. Neck pain, which occurred in 44.3% of the total population and in 72.4% of females with MA, is not well defined and overlaps with whiplash. However, there was an association with migraine as also previously reported (66). Osteoarthritis, scoliosis, osteoporosis, Scheuermann’s disease and fibromyalgia were co-morbid with migraine in all and in female subjects with migraine or MA. Co-morbidity of these musculoskeletal disorders and migraine has not previously been studied. Association of migraine and fibromyalgia has been suggested (67).
Autoimmune disorders
Overall, there was a strong co-morbidity of migraine with autoimmune disorders although some of the disorders had a low absolute prevalence. The total prevalence of any autoimmune diseases was 7.3% of which the majority was psoriasis (4.1%). Unspecific arthritis or diseases of connective tissue had a total prevalence of 2.3%, rheumatoid arthritis 0.9%, and lupus only 0.2%. There is a considerable literature on lupus and headache summarised in a recent meta-analysis which found that ‘pooled data from seven controlled studies showed that the prevalence of all headache types, including migraine, was not different from controls’ (68). In contrast, we investigated the prevalence of lupus in migraine patients and found, despite relatively small numbers, an increased co-morbidity of lupus (OR 2.8).
Psoriasis, being a much more common disease, showed more consistent results. All subgroups showed essentially identical results (OR 1.4) and only male subjects with MA did not show significant co-morbidity. Rheumatoid arthritis showed co-morbidity with migraine especially in females and in MA. The group with unspecific arthritis or diseases of connective tissue showed the same pattern – co-morbidity with females and MA.
The observed co-morbidity of migraine with autoimmune disease raises the question: is migraine a systemic disorder or is there some common genetic background for migraine and autoimmune disorders?
Thyroid diseases
Previous studies showed increased prevalence of hyperthyroidism (OR 1.3) and hypothyroidism (OR 1.2) in female migraine patients but no significant correlation in males (69). A small study found that subjects with hypothyroidism were four times more likely to have migraine (18) and all affected subjects were female and had MO. Our results showed co-morbidity with hypothyroidism (OR 1.6–2.4) as well as hyperthyroidism (OR 1.5–2.4) and goitre (OR 1.3–2.7).
Hyperthyroidism and hypothyroidism are both autoimmune thyroid disorder and their combined prevalence in the general population is reported to be 3–5% (70) compared to a prevalence of 4.5% for any thyroid disease in the present study. Both hyperthyroidism (2.2% in migraine patients vs 1.2% in healthy subjects) and hypothyroidism (2.1% vs 1.0%) were co-morbid with migraine. This could be an autoimmunity diathesis in migraine (see above).
Atopic diseases
The association between migraine and asthma (12,71–73) and allergy (12,74) is well documented. A recent study (12) found an increased risk for asthma (OR 1.6–2.9) as well as hay fever (OR 1.5–2.6) among migraine patients. We found both asthma and allergy to be significantly co-morbid with migraine (OR 1.1–1.7) in all groups except males with MO.
Audio-vestibular disorders
More women than men had Ménière’s disease amongst migraine cases in agreement with previous studies (17,75,76). MA was the predominant type of migraine among Ménière patients with a prevalence of 1.1% unlike a previous study that reported MO to be the most common type of migraine in these patients (17). Tinnitus had a total prevalence of 7.8% and tinnitus was co-morbid with migraine with a prevalence of 9.7% in females with MA and 15.8% in males with MA.
Other medical diseases
We could not detect any significant association between self-reported migraine and diabetes. Results of previous studies are conflicting, some showing co-morbidity (77), some not (73), and yet others reporting an inverse association (15,78). The bidirectional co-morbidity between migraine and epilepsy has been well documented in previous studies (11,79,80). We found epilepsy to be co-morbid with migraine and MA in all subjects (prevalence 2.7%) and in females (prevalence 2.7%). Kidney stones were surprisingly co-morbid with all diagnostic groups except MA in male subjects. The reason underlying this finding remains elusive. To our knowledge, no studies have yet investigated the relationship between migraine and kidney stone.
Conclusions
We have demonstrated co-morbidity between a number of medical diseases and self-reported migraine and have distinguished between the subtypes MA and MO and between sexes. For most diseases, this has not been done before. Furthermore, we have demonstrated co-morbidity between migraine and autoimmune disorders, thyroid disorders and kidney stone for the first time. These co-morbidities should be evaluated and treated in migraine patients. Apart from the clinical relevance, co-morbidities are also important for aetiological theories of migraine. Future work should analyse genetic as well as environmental factors that may be the reason for the observed co-morbidities. The present study calls in particular for further investigation of possible autoimmune mechanisms of migraine.
Footnotes
Acknowledgements
The authors thank Dr Anders Jørgen Svendsen, consultant, guest researcher, the Danish Twin Registry, Epidemiology, Institute of Public Health, University of Southern Denmark, Denmark, Dr Thomas Brix, consultant, Endocrinology Department M, Odense University Hospital, Odense, Denmark, Dr Vibeke Backer, consultant, associate clinical professor and Simon Francis Thomsen, Department of Lung Medicine, Bispebjerg Hospital, Bispebjerg, Denmark, Dr Frank Damborg, consultant, Lillebaelt Hospital, Kolding, Denmark, Dr Wilhelm Engell, senior resident, Lillebaelt Hospital, Vejle, Denmark, Dr Mikkel Andersen, consultant, Lillebaelt Hospital, Give, Denmark, Prof. Charlotte Lebeuf-Yde, The Back Research Unit, Institute of Health Services Research, University of Southern Denmark, Denmark, Prof. Jan Hartvigsen and associate prof. Rene Fejer, Institute of Sports Science and Clinical Biomechanics, University of Southern Denmark, Denmark, Simon Francis Thomsen and Steen Fibiger, Centre for Rehabilitation and Special Counselling, The Southern Danish Region for access to data from the ‘Twin Omnibus 2002’ study. The authors also thank Jytte Duerlund for assistance in carrying out the ‘Twin Omnibus 2002’ study. None of the above mentioned persons received compensation for their assistance.