
Abstract
Psychiatric co-morbidity is an important risk factor for chronification of primary headache into adulthood. The aim of this study was to investigate the extent and clinical relevance of emotional and behavioural problems in children and adolescents with primary headache. Children and adolescents (n = 128) with primary headache (International Headache Society, codes 1.1, 1.2, 2.1) and 83 matched controls aged 6-18 years were examined by standardized dimensional psychomet-rical tests (Child Behaviour Checklist, Depression Inventory for Children and Adolescents, Anxiety Questionnaire for Pupils). Children and adolescents with primary headache suffer more often from internalizing problems (depression, anxiety, somatization) than healthy controls. The detected emotional and behavioural problems are clinically relevant and require particular therapy in every third child suffering from headache. Two out of three children and adolescents with primary headache do not show clinically relevant psychopathology and may benefit from minimal therapeutic intervention. One of three examined headache patients needs additional psychiatric therapy.
Introduction
Recurrent primary headache is the most frequent neurological symptom at school age and the most frequent manifestation of pain in childhood (1). The prevalence in children and adolescents has increased over the last decade to 15% for migraine (2–4) and to 17% for non-migraine headache (5, 6), while the age of onset has decreased. Headache in children has a high risk of the development of chronic headache and tends to persist into adulthood in 60% (7, 8).
Chronic headache (9, 10), especially migraine (11, 12), causes high socio-economic costs in providing healthcare in adults. The economic consequences of lost and reduced productivity are great, but indirect costs (e.g. absenteeism, reduced work efficiency) are even higher and increase with headache severity (12) and frequency (13).
Psychiatric co-morbidity has recently been identified as an important risk factor for the development of chronic headache. The presence of psychiatric co-morbidity, especially anxiety and depression in children and adolescents with headache, is related to enduring headache for> 8 years (14). Depression, anxiety, and somatization are the most common psychiatric co-morbidities in adults with migraine and/or tension-type headache (15–19). This has been confirmed in children and adolescents in longitudinal (20–22) and clinical studies (23–26), as well as community samples (27–29). Associations between migraine, depression and anxiety were found using categorical diagnostic criteria (14, 20, 30). Egger and co-workers found that childhood headache is related to internalizing disorders (depression, anxiety, somatization) diagnosed by DSM-III-R (21).
Some studies failed to find direct associations between co-occurring disorders and headache (31, 32), but they suggested anxiety as a headache trigger factor.
There are differing views concerning the underlying biological or psychological causes linking migraine or tension-type headache, and psychiatric disorders:
One disorder predisposes the other. Support for the hypothesis that migraine predisposes to depression as a secondary reaction to chronic pain is given by several authors (25, 33, 34). Other researchers found an inverse relationship or presumed that both psychiatric disorders can lead to recurring headache (20). Merikangas and co-workers, for example, supposed that anxiety in childhood predicts migraine and migraine in childhood predicts depression in adults (15).
Some older studies suggest that chronic pain constitutes an equivalent to depression, e.g. (35–38).
A common underlying genetic or environmental risk factor is assumed, which causes a dysregulation in serotonergic and noradrenergic systems, the common neurotransmitter systems involved in migraine, depression, and anxiety (20). Some authors suggest that behavioural abnormalities in children and adolescents may be the result of a genetically determined cortical hypersensitivity, which may be reflected in higher amplitudes of contingent negative variation (CNV) components (39–42). This possibly leads to a combined risk of developing both behavioural and pain problems.
Increased levels of internalizing problems in children and adolescents were also found using dimensional standardized psychometrical testing (25, 33). This diagnostic method provides reliable statements about the extent of a symptom. In contrast, categorical diagnostic interviews are highly specific, but the sensitivity to detect early signs of emotional and behavioural problems is poor.
The Child Behaviour Checklist (CBCL; parental version (43)) is a very common standardized procedure to assess emotional and behavioural problems in children and adolescents from the age of 4 years onwards. Many investigators found higher levels of somatization and internalizing disorders in headache sufferers using the CBCL (parental version). Migraine-associated symptoms (headache, nausea/vomiting, eye problems) are included as items in the CBCL Somatic Complaints Scale and consecutively in the Internalizing Score (second order scale). Therefore previous investigations may possibly have overestimated psychiatric co-morbidity, especially internalizing disorders, since migraine symptoms could have been confounded with psychiatric internalizing co-morbidity. All known studies which found higher levels of somatization and internalizing disorders in headache sufferers using the CBCL failed to control these items (6, 25, 33).
The aim of this study was to investigate the extent and the clinical relevance of psychiatric co-morbidity in children and adolescents with primary headache using dimensional standardized diagnostic tools, including self and parental rating to describe emotional and behavioural problems. The following questions are addressed: (i) do children and adolescents with primary headache have more emotional and behavioural problems than healthy controls? (ii) are these emotional and behavioural problems clinically relevant? (iii) are there differences in the emotional and behavioural problems between the headache subtypes (migraine with and without aura, tension-type headache)?
Methods
Sample
The available data are based on a neurophysiological and psychological study in children and adolescents (6–18 years of age) which aims at establishing additive objective diagnostic criteria and neurophysiological markers for the diagnosis of migraine. One hundred and twenty-eight headache sufferers (60 females and 68 males) who presented with headache as their primary problem were recruited from the general population (75.4%) or from the neuropaediatric out-patient clinics (24.6%) of the University of Heidelberg and Mannheim and enrolled consecutively in the study. Eighty-three age- and sex-matched healthy volunteers (39 females and 44 males) were recruited in the same manner (local newspaper, hospital intranet) from the general population (for sample characteristics see Table 1). The study was conducted according to the Declaration of Helsinki on biomedical research involving human subjects. The protocol was approved by the University of Heidelberg Ethics Review Committee. All subjects were instructed about the study and signed informed consent was obtained from children and parents.
Sample characteristics

CO, Controls; MO, migraine without aura; MA, migraine with aura; TTH, tension-type headache.
All subjects were German speaking. The headache subgroups and the control group did not differ significantly in respect of educational level (Fisher's exact test: P = 0.154). The parents of controls achieved higher education and worked more often in highly qualified or prominent job positions (χ2 = 19.89, d.f. = 6, P = 0.003 for fathers’ education and χ2 = 38.51, d.f. = 6, P ≤ 0.001 for mothers’ education). Nationality was not significantly different between the headache and control groups (χ2 = 5.38, d.f. = 3, P = 0.146).
Diagnostic assessment of headache
Diagnosis was established by a self-designed, structured diagnostic interview according to the International Headache Society (IHS) criteria. The child and one of his or her parents were interviewed in a first examination. If more than one type of headache was reported, items were requested for both types of headache. Multiple diagnoses were possible. The interview included headache-specific characteristics (IHS criteria, intensity, quality and localization of pain, frequency and duration of headache, aura and associated symptoms). Information was also given about the history of headaches in the family, the child's own experience with pain, trigger factors, subjective distress, fear of headache attacks, aura symptoms, impairment of daily activities and other health and pain problems, their onset and changes over time. Ten-point scales were applied for intensity (ranging from a little painful to extremely painful), fear of attack (little fear–great fear), and subjective distress (not bad–very bad).
Before application, the interview was pretested by an experienced headache therapist and the interviewers were trained. Inter-rater reliability was investigated in a pilot study (n = 12) by two independent raters. To assess the reliability of intervally scaled items, the intraclass correlation was computed. For nominal dichotomically scaled items Cohen's κ, and for nominal categorically scaled items weighted κ was chosen. The inter-rater reliability in total for the children's part of the interview was mean κ = 0.902 (range κ = 0.647–1.00). Only two items (‘different headache types’ and ‘coping by laying down’) had an insufficient inter-rater reliability. The mean of the intraclass correlation in the children's part of the interview was ρ = 0.949 (range ρ = 0.735–0.997). In the parental part of the interview, the mean κ was κ = 0.880 (range κ = 0.625–1.00). Here the items ‘previous therapy’ and ‘switching between different unspecific symptoms in lifetime’ were insufficient to rate. The mean value of the intraclass correlation was ρ = 0.990 (range ρ = 0.982–0.996).
A child-adapted prospective daily headache diary (44) was used to assess headache characteristics over an 8-week period from the first examination on. Prospective inquiry of headache using a diary is recommended to validate headache diagnosis. The chronicity of tension-type headache can be investigated reliably only by diary data (IHS: headache frequency ≥ 15 days/month). Many children and adolescents began to recognize additional tension-type headache episodes and associated migraine symptoms after they had started to pay more attention to their headache by filling in the headache diary.
Inclusion criteria for the headache group were primary recurring headache (IHS codes 1.1, 1.2, 2.1) over a period of at least 1 year and three to 18 attacks in the last quarter. Exclusion criteria were other headache subtypes (IHS codes 1.3–1.7, 2.3, 3–13), serious basic diseases, continuous medication and pharmacological prophylactic treatment for migraine over the last 6 months. According to the IHS diagnoses, 70 patients were classified as suffering from migraine without aura (IHS code 1.1: MO), 33 from migraine with aura (IHS code 1.2: MA), and 25 from tension-type headache (IHS code 2.1: TTH). According to the interview, no patient fulfilled the IHS criteria of chronic tension-type headache (IHS code 2.2). The headache diary over 8 weeks, however, gave evidence of chronic TTH in 16 patients, who were allowed to continue with the study protocol. In the MO group 28.1% were suffering additionally from episodic TTH and 4.7% from chronic TTH. Of the MA group, 8.6% had an additional episodic TTH and 3.1% suffered from the chronic type. In the TTH group 4.7% of the patients fulfilled the criteria for chronic TTH.
All subjects underwent a neurological examination, EEG recording and an ophthalmological examination. The control group completed a self-developed questionnaire to gain information about somatic complaints, medical history and pharmacological and psychological treatment. Control children and adolescents were not permitted to have any first-degree relatives suffering from migraine.
Psychological assessment
Dimensional diagnostic tools were used for psychological diagnostics because of their higher sensitivity for subthreshold psychiatric diagnoses, which is useful to identify children and adolescents who are at risk of developing a categorical diagnosis in future. Self and parental reports were applied to increase the validity of information. All used instruments have known validity and reliability. The same questionnaires were used with all age groups, because they are applicable over all developmental levels. Depression was measured one-dimensionally with a 27-item standardized psychometrical questionnaire on self-report – Depression Inventory for Children and Adolescents (DIKJ (45); German version based on the Children's Depression Inventory by Kovacs, 1985). The DIKJ has satisfactory internal consistency and convergent validity. Each child is asked to select one of three statements for each item which best describes him or herself. A global scale is assessed to measure the current level of depressive symptomatology. To assess anxiety, the Anxiety Questionnaire for Pupils (AFS (46)) was used. The AFS as a multifactorial questionnaire contains 50 items to measure and comprises four scales: Test Anxiety, General Anxiety, Dislike of School, and Lie Scale. The child has to decide for each item if she or he agrees with the statement. To evaluate the parental rating for behavioural and emotional problems, all syndrome scales and the Total Problem Score of the CBCL (43) (German parental version, 1991) were applied. The CBCL contains 120 behaviour problem descriptors as a checklist. It can be rated with ‘not true’, ‘sometimes true’ or ‘often true’. The reference period is the last 6 months. The nine symptom scales are Withdrawal, Somatic Complaints, Anxiousness/Depression, Social Problems, Thought Problems, Attentional Problems, Delinquent Behaviour, Aggressive Behaviour, Other Problems. Two composite scales, Internalizing and Externalizing, were additionally measured. Good test–retest (r = 0.89) and inter-rater reliability has been shown (ρ= 0.90) (43). The scales discriminate well between clinical and non-clinical samples of children and adolescents. The behaviour-related factors differ according to age and gender. ‘Clinical relevance’ of behavioural and emotional problems was defined as a CBCL Total Problem Score: T-score ≥ 64. This is in accordance with the recommendations of Achenbach et al. (43).
Statistical analysis
Univariate analysis of variance was calculated to evaluate the influence of diagnosis (four levels: controls, TTH, MO, MA), age and sex. T-scores of all reported scales were used as dependent variables. Post hoc analysis was carried out by Scheffe's test. R 2 indicates the level of explained variance by diagnostic group differences in the CBCL scales.
The differences between the scores of clinical relevance of the CBCL Total Problem Score (T-score ≥ 64) were assessed with the χ2 test. In order to control headache- and migraine-associated symptoms in headache sufferers, all items with migraine-associated phenomena (nausea, vomiting and eye problems) in the Somatic Complaints Scale were replaced by zero. Other pain, stomach ache, vertigo, skin problems and tiredness were still included in the score. The sum scores of the Somatic Complaints Scale, the Internalizing Score, and the Total Problem Score were adapted and the T-values were modified. The influence of education of children and parents on the CBCL second-order scales was tested by analyses of variance.
SPSS for Windows 10.0 software was used for statistical analyses.
Results
Mean differences between diagnostic groups in emotional and behavioural problems
Parental report
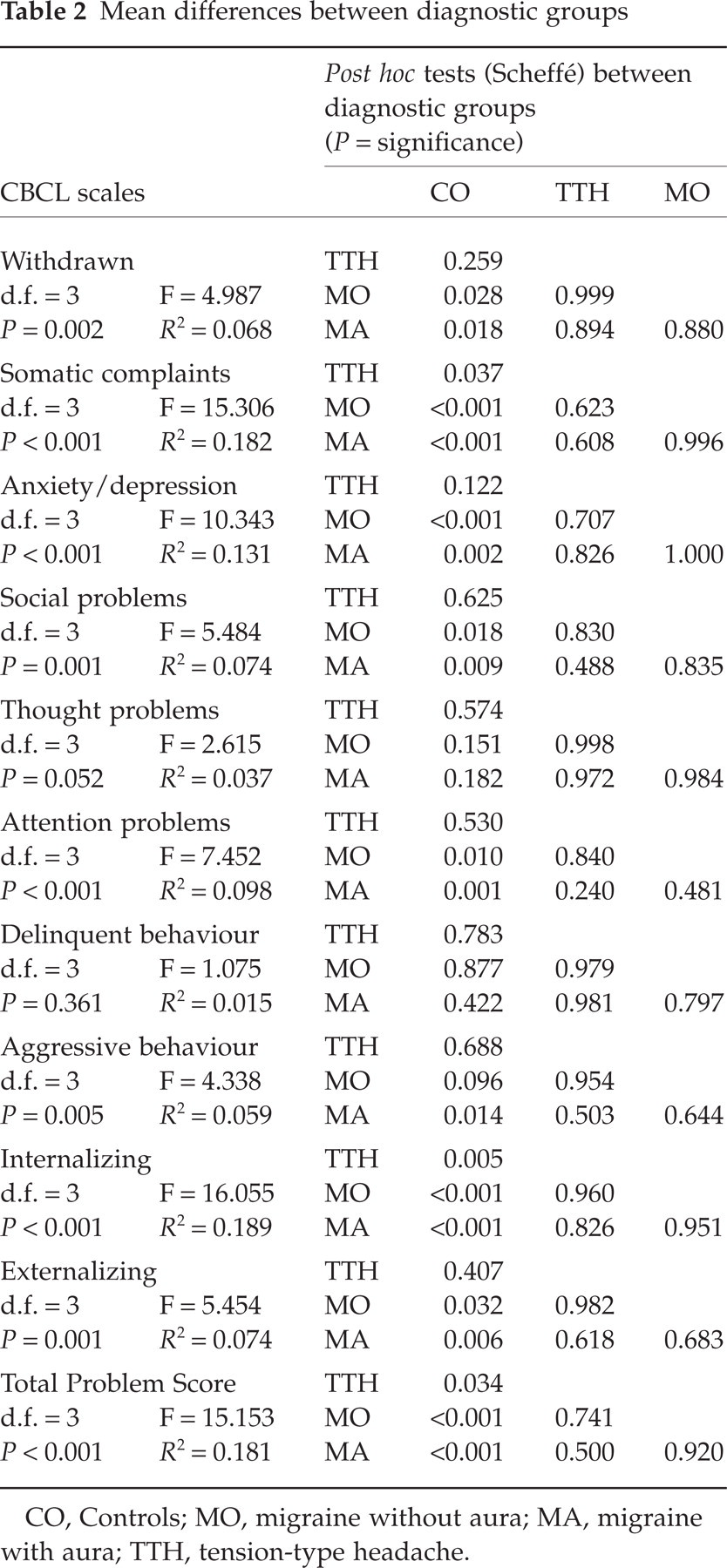
Children and adolescents with headache showed significantly more emotional and behavioural problems in parental reports (CBCL) than healthy controls. Differences were most pronounced in the Total Problem Score and the Internalizing Score (Fig. 1: scales of second order). Means (T-scores) were significantly different between diagnostic groups for all first-order scales except Thought Problems and Delinquent Behaviour. Significant group and post hoc differences between groups are given in Table 2. The highest extent of variance explained by diagnostic group differences (R 2) is found for Somatic Complaints (18.2%), Anxiety/Depression (13.1%), and for Internalizing Disorders in total (18.9%) (see Table 2).
Mean differences between diagnostic groups
CO, Controls; MO, migraine without aura; MA, migraine with aura; TTH, tension-type headache.
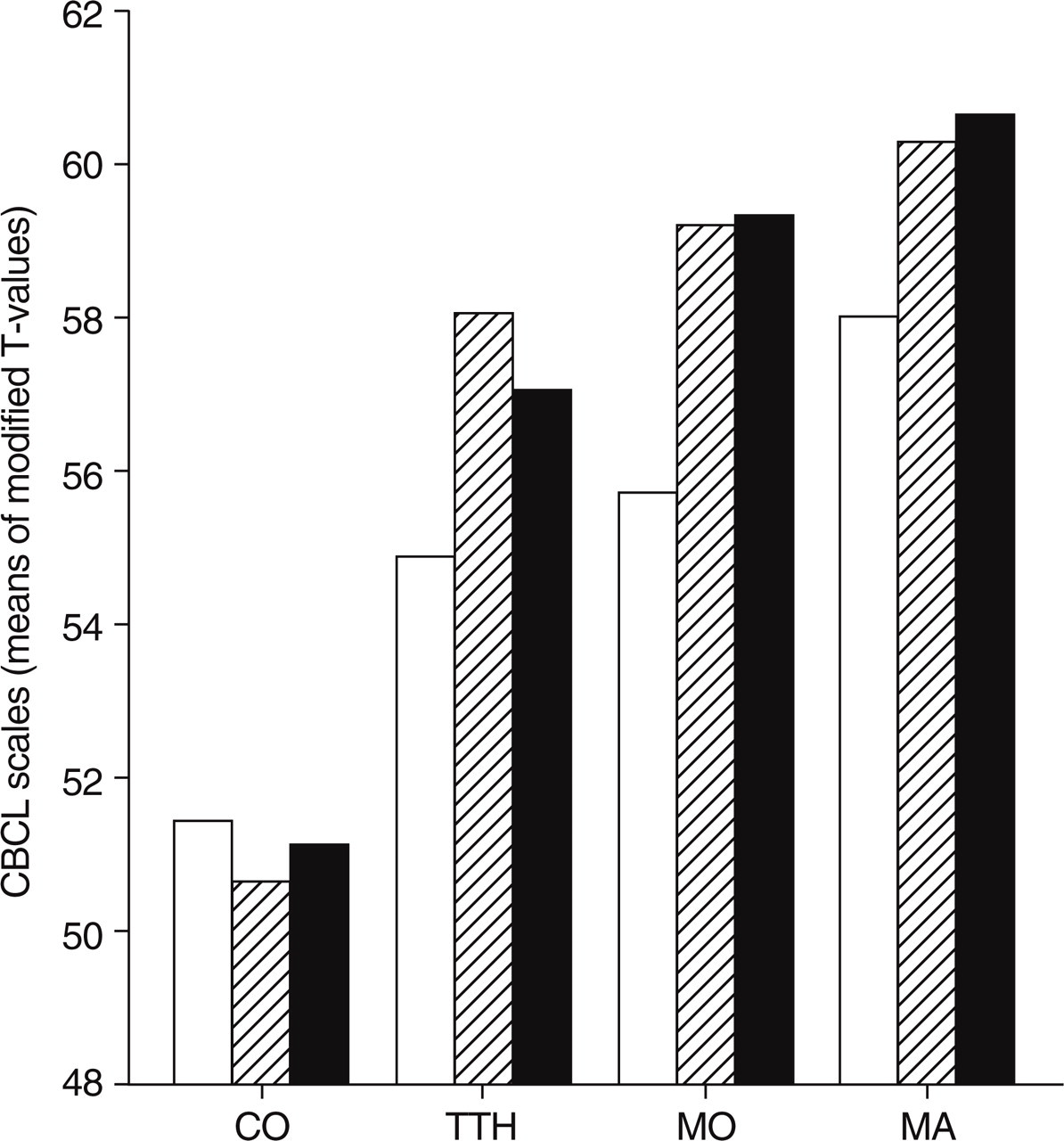
Scales of second order. CO, Controls; MO, migraine without aura; MA, migraine with aura; TTH, tension-type headache. □, Externalizing scale; hatched, Internalizing scale; ▪, Total Problem Score.
Clinical relevance
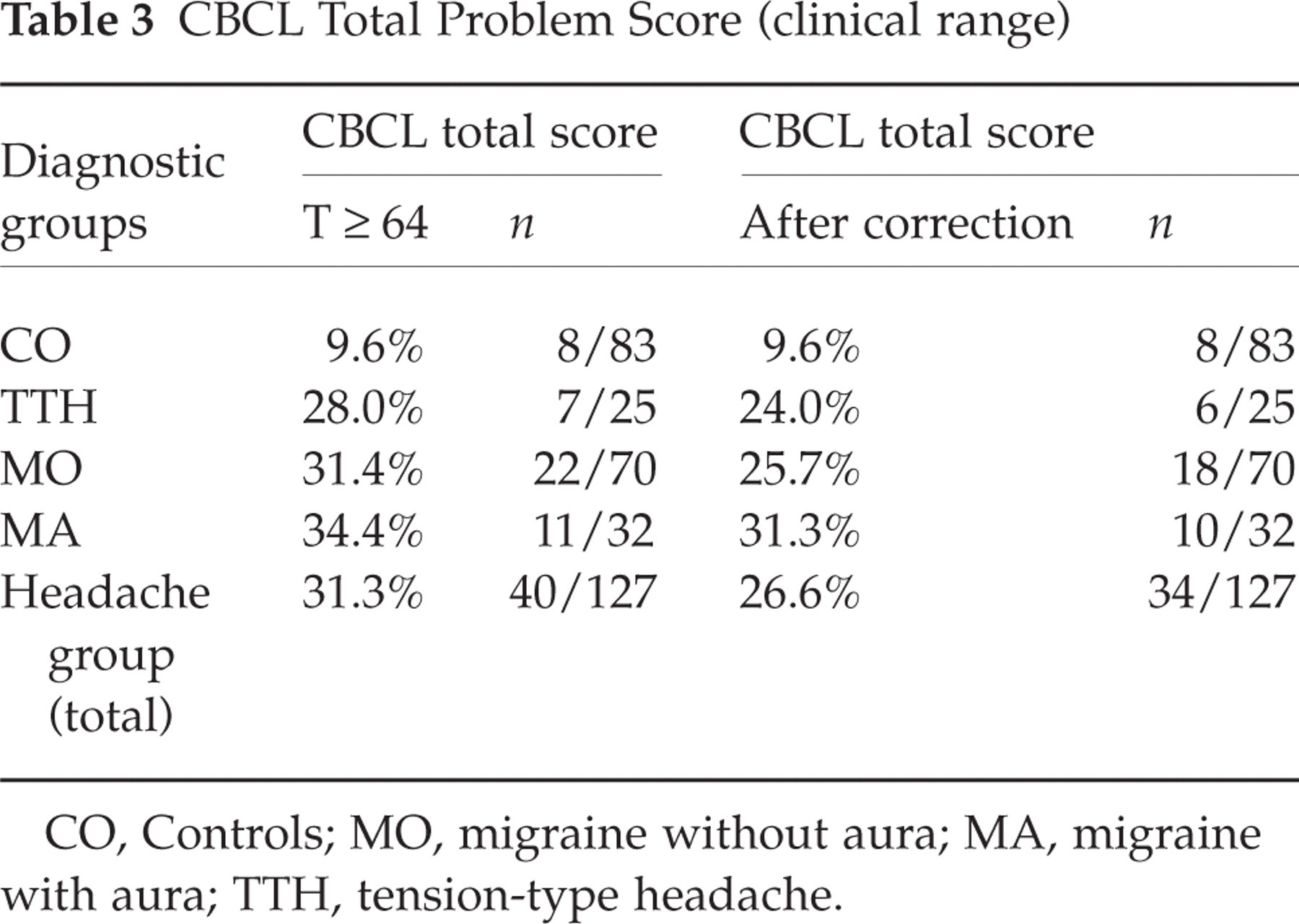
About one-third of children and adolescents in the headache groups suffered from emotional and behavioural problems of clinical relevance (according to Achenbach et al. (43)) vs. one-tenth of controls (uncorrected χ2 = 13.82, d.f. = 3, P = 0.003; corrected χ2 = 9.77, d.f. = 3, P = 0.021, see Table 3). The correction of artefacts indicated 4–5% false-positive ratings using the uncorrected scales.
CBCL Total Problem Score (clinical range)
CO, Controls; MO, migraine without aura; MA, migraine with aura; TTH, tension-type headache.
Self reports
For the DIKJ global depression scale, diagnostic groups were significantly different (F = 3.41, d.f. = 3, P = 0.019). But post hoc analyses only showed a trend (P = 0.075) for the difference between controls and MA. In subscales of the AFS, diagnostic groups were not significantly different (Test Anxiety F = 1.65, d.f. = 3, P = 0.179; General Anxiety F = 2.41, d.f. = 3, P = 0.068; Dislike of School F = 1.58, d.f. = 3, P = 0.197; Lie Scale F = 1.19, d.f. = 3, P = 0.314).
Children's and parental education
The influence of the children's and parental education on the CBCL second-order scales was non-significant in the Total Problem Score for schooling (d.f. = 4, F = 0.694, P = 0.597), for father's education (d.f. = 3, F = 0.671, P = 0.571) and for mother's education (d.f. = 2, F = 1.37, P = 0.256).
Discussion
The key findings are: (i) children and adolescents with primary headache suffer from more behavioural and emotional problems than healthy controls; (ii) one-third of children and adolescents with headache have behavioural and emotional problems of clinical relevance; two-thirds do not show clinically relevant psychopathology.
The result that children and adolescents suffering from headache show more internalizing disorders is in line with the findings of other investigators (14, 25, 33). Strong associations were found between major depressive disorder and headache, especially in adolescents with migraine (47). Pine and co-workers otherwise found double the headache in depressive than that in non-depressive children in an epidemiological study, but no effect of headache on the risk of future depression (20). The direction of causality remains unclear and can also not be answered in this study.
No significant differences were found in self-rating of depression and anxiety. This probably reflects lack of self-perception in the young, and might furthermore be a sign of alexithymic behaviour. Our results show elevated depression rates reported by parents, but not by children and adolescents themselves. This is inconsistent with results from a review by Angold and co-workers (48), who found that parents report depressive symptoms less often in nearly all epidemiological studies. The parents of our study subjects, who responded to our announcement, were possibly more concerned about their children and more sensitive to disturbed emotions and behaviour.
The high values of migraineurs in the Somatic Complaints Scale even after the correction of migraine-associated symptoms might represent somatization.
To the best of our knowledge, no study has been published that used CBCL scales corrected for headache- and migraine-associated symptoms. Cunningham and co-workers only discussed this point of view (33). They found the frequency of somatic complaints to be the only variable, which discriminates between musculoskeletal pain patients and headache sufferers. The higher frequency of somatic complaints in the headache group could be explained by the nature of the migraine disorder. The only known study which controlled migraine-associated symptoms in a somatization inventory found more somatic complaints independent of migraine-related symptoms in frequent headache sufferers (29).
According to Amminger and co-workers, childhood behaviour is a significant predictor of adult co-morbidity (49). This implies that our dimensionally measured results might give hints for the risk of the development of a categorical diagnosis in future.
In all headache sufferers, emotional and behavioural problems of clinical relevance were three-fold more frequent than in headache-free controls. These findings are in concordance with many studies in adults, which reported major depression and anxiety disorders in migraine sufferers as a serious health problem (50).
Our sample was not randomly selected, and was chosen by sampling procedures described above. Patients who responded to the announcement may be seeking counselling and medical treatment of their children and might therefore experience more subjective distress and psychic problems than non-responding headache sufferers. Other limitations pertain to the headache diagnoses. Episodic and chronic TTH were not distinguished in separate groups, because the numbers in each group were too small to give reasonable interpretations. In general, the validity of IHS criteria in childhood headache is presumed to be problematic (51, 52). High specificity but poor sensitivity have been frequently criticised. Some criteria are not common in children, such as unilateral localization or pulsating quality of headache. Often one criterion decides whether childhood migraine and TTH are diagnosed. More sensitive criteria are currently being developed, but at present, the IHS criteria are still ‘gold standard’, even in children. Finally, one methodological limitation that should be mentioned is that the modification of the T-values in the CBCL possibly leads to an underestimation of clinical relevance, because the critical T-value depends on the mean value of the tested population.
Two of three children and adolescents with primary headache do not show clinically relevant psychopathology and may benefit from minimal therapeutic intervention. One-third of examined headache patients needs additional psychiatric therapy. To prevent the development of chronic headaches, psychiatric co-morbidity (respective emotional and behavioural problems of clinical relevance) should be detected early and treated sufficiently. This may render prophylactic and acute treatment of headache more effective. Early treatment is also relevant for economic reasons (53).
In light of the above results, the following recommendations may be considered. Early medical treatment of acute headaches is necessary to decrease the intensity and duration of the headache. This may result in reducing and preventing the loss of self-control and helplessness experienced by the patient. Moreover, pharmacological prevention may also further this end if frequent headaches are experienced. Under these circumstances, psychological intervention may also improve coping strategies, thus hopefully improving the medical and psychological outcome.
Both treatments are described to reduce the frequency of attacks (4, 54–56). Two of three children and adolescents suffering from primary headache do not show emotional and behavioural problems of clinical significance. They may benefit from minimal therapeutic intervention, including improvement of acute pharmacological therapy, control of individual trigger factors, recommendations for individual relaxation strategies, encouragement to withdraw when necessary (e.g. to say ‘no’ and to care for themselves in daily routines) and explanation and reassurance that the problem is not life threatening.
In contrast, children and adolescents with primary headache and emotional/behavioural problems of clinical relevance need special psychiatric therapy (including the points mentioned above) which focuses on individual psychopathology in addition to medical management of their headache. Up to now it has not seemed clear how to distinguish easily between headache patients with and without relevant psychopathology (without psychometric testing) in a standard paediatric setting, which is the first contact point in most cases. To answer this question, further investigations are needed to evaluate shorter screening methods for diagnosis and indications for differential treatment of headache and co-occurring disorders.