
Abstract
The level of agreement between headache information, attained by clinical interview and headache diary, was evaluated in subjects who frequently suffered from headache and were participating in an epidemiological study of headache. One hundred and six subjects were interviewed and asked to complete a diary for a period of 4–8 weeks; 46% completed the study. For migraine the diary and clinical diagnoses demonstrated agreement in 82%, κ value 0.57, sensitivity 90% and specificity 64%. For tension-type headache they demonstrated agreement in 87%, κ value 0.39, sensitivity 97%, specificity 29% and a good agreement of frequency of tension-type headache was also obtained. In migraine, but not in tension-type headache, accompanying symptoms tended to be overestimated in the interview. The diary was not useful for the diagnosis of migraine with aura, but proved valuable in distinguishing between migraine and tension-type headache, and in the identification of coexisting headache disorders. Combined use of a diagnostic diary and clinical interview is recommended.
Introduction
Headache disorders, such as migraine and tension-type headache, are usually diagnosed on the basis of different combinations of symptoms and accompanying symptoms, set out in the Classification and Diagnostic Criteria for Headache Disorders, Cranial Neuralgias and Facial Pain by the International Headache Society (IHS) (1). Coexisting headache types and patient recall bias are major problems, well known to any interviewer, and the background for the development of headache diaries. Different headache diaries have been used and proven valuable in various situations such as measuring work disability (2), diagnosing headaches in children (3–5), validating questionnaires (6) and describing aura symptoms in relation to migraine (7).
The diagnostic headache diary used in this study is based on the operational diagnostic criteria of the HIS classification, 1st edition (1). It has been validated in a group of migraine patients from a specialized headache clinic and was found to be an important supplement to the clinical interview (8, 9). As part of an epidemiological survey of migraine and tension-type headache in a general population, the present study compares diagnoses and symptoms attained by clinical interview with those attained by diary. The aim was to reveal advantages and disadvantages of the diary used in a population-based group and to validate a clinical interview in relation to a diagnostic diary.
Materials and methods
Headache study
In 1989 an epidemiological study of headache in 1000 subjects from a general population was carried out at Glostrup University Hospital, which is situated in the western part of Copenhagen (10). As a follow-up, a corresponding study was made in 2001, inviting the same cohort as in 1989 (now aged 37–76 years) and a cohort of 300 young adults (aged 25–36 years) to establish a similar age group as in the first study (11). In 2001 a total of 1175 subjects were eligible for participation (i.e. alive, living in Denmark and able to answer written and verbal questions). The 125 non-eligible subjects were excluded because: 83 were deceased, 16 had emigrated, 14 were missing or had errors in the address list and 12 were unable to answer questions in Danish or English. In total, 848 participated (72.2%), 555 in the face-to-face interview and 293 in the telephone interview. A detailed description of methods and material is given elsewhere (11). The aim of the epidemiological study was to investigate the prevalence, incidence, prognosis, risk factors and personal and socio-economic costs of migraine and tension-type headache.
All subjects were invited to a general examination, with emphasis on primary headaches, which included a structured clinical headache interview, physical and neurological examination and a self-administered questionnaire. In cases where subjects did not participate in a clinical interview, attempts were made by the investigator to reach them by telephone and, if possible, a headache diagnostic interview was completed in this manner. The headache disorders were diagnosed and coded according to the criteria of the IHS 1988 (1). Migraine with aura, migraine without aura and tension-type headache are not mutually exclusive headache diagnoses. Each distinct form of headache in each individual was diagnosed; hence, coexisting migraine and tension-type headache could also be assessed. All interviews throughout the 2001 survey (both clinical and telephone interviews) were conducted between May 2001 and April 2002 by an experienced medical doctor (A.C.L.).
In 2001, the total population of the sampling area was 332 494, or 6.2% of the total Danish population (5349 212 persons) (12). The inhabitants of the sampling area were representative of the total Danish population with regard to age, gender and unemployment rate (12). Moreover, analyses of the demographic composition in 1989 and in 2001, and analyses of immigration to and emigration from the area with regard to age, gender and income revealed no major changes over this time period (12).
The study was approved by the Ethics Committee for Copenhagen County and The Danish Data Protection Agency. Informed consent was obtained from each participant before the interview.
Diary study
Sampling
As a part of the epidemiological headache study, 106 persons (12.5%) were asked to complete a diagnostic headache diary. The 106 participants were identified during interviews and examinations, where the interviewer found it difficult to diagnose the headaches on the basis of the history alone (i.e. subjects were unable to characterize their headache quality, frequency and/or associated symptoms). Participants were provided with a diary for a maximum of 24 headache days and asked to return the diary when completed, or at the latest after 2 months. A letter and a new diary were sent to those who did not return their diary, asking them to fill in the new diary or return the first one.
The diagnostic headache diary
The diagnostic headache diary is based on the criteria of the IHS and the questions provide the characteristics necessary to diagnose and distinguish between migraine and tension-type headache (8). One hundred and six participants received a diagnostic headache diary at the interview and were instructed to complete it at the end of each headache day. Since the questions in the diary were identical to those in the interview, they were familiar to the participants (Fig. 1).
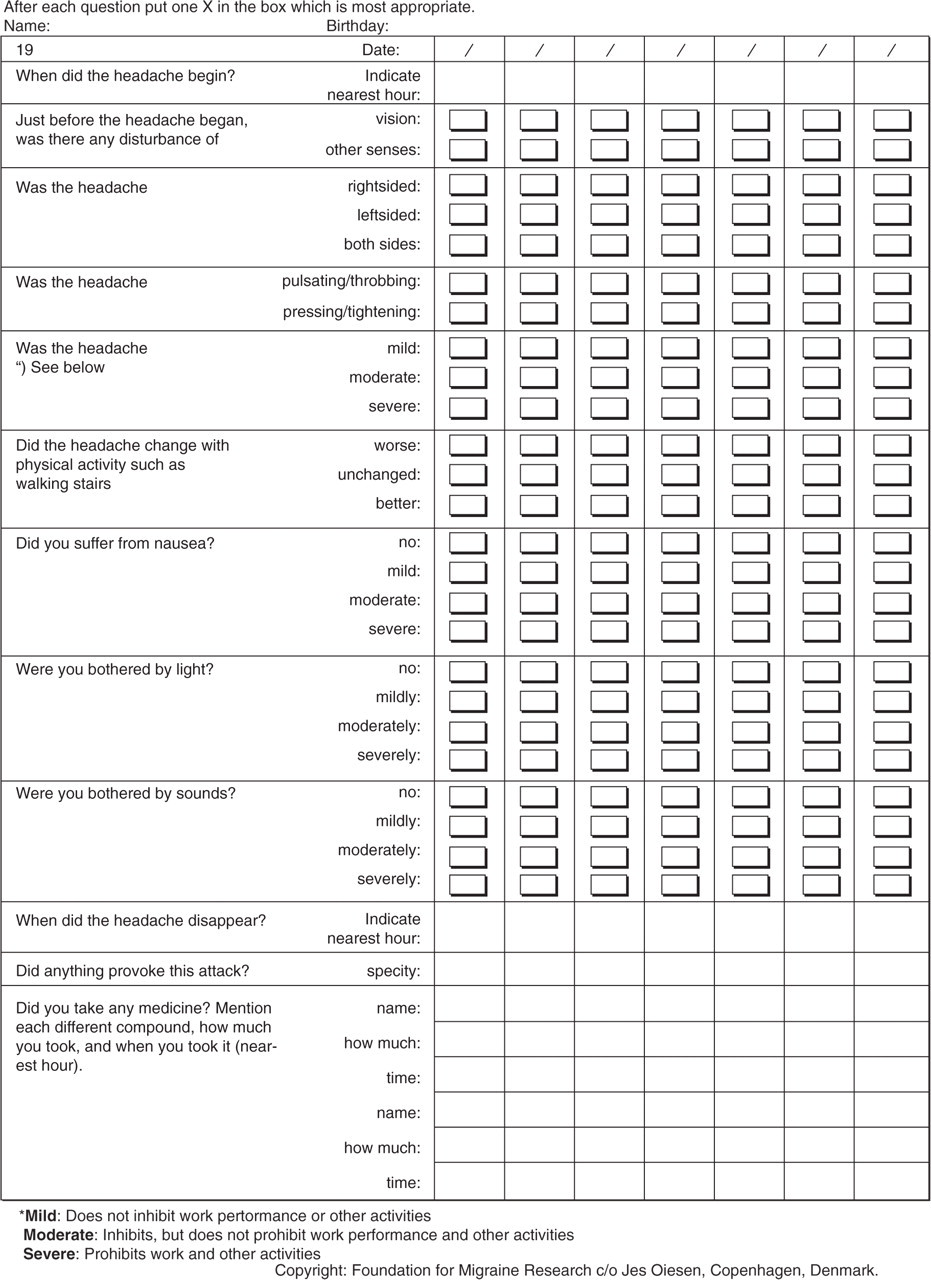
Diagnostic headache diary.
The diagnostic headache diaries were examined by two independent observers, who had knowledge of neither the clinical diagnosis nor the diagnosis made by the other observer. Each recorded headache was diagnosed and coded according to the IHS criteria, 1st edn. If a recorded headache missed one or more answers or had two or more answers marked to each question, it was not classified unless the diagnosis was absolutely clear regardless of the missing answers. As proposed in the evaluation of the diary (8), a set of rules for reading the diary was made, based on the diagnostic criteria of the IHS. The diagnoses from both observers were in agreement in all cases.
The IHS criteria distinguish between migraine with aura (MA) and migraine without aura (MoA). In the diagnostic headache diary only one question concerns aura, and it serves primarily as a screening question for aura, therefore we did not separate the diagnoses MA and MoA in the diary diagnosis.
The criteria for chronic tension-type headache and for headache induced by chronic substance use or exposure were modified due to the short registration period. The general requirement for diagnosing chronic tension-type headache, is 15 days a month during at least 6 months. In this study, we used the diagnosis of chronic tension-type headache in the diagnostic headache diary, if the participant had tension-type headache for at least a half or more of the days in the registration period. Likewise, for headache induced by chronic substance use or exposure, IHS requires daily doses of the substance for at least 3 months, and that the headache disappears within 1 month after withdrawal (1). It is not possible to know about these two items from a diary kept for a maximum of 24 days. Therefore, we used the diagnosis ‘headache induced by chronic substance use’ when the headache was chronic (≥15 days a month) and the criterion about analgesic dose was kept. As in the headache interview, individuals could have more than one form of headache in the diary. Each distinct form of headache within the individual was diagnosed.
Statistics
All data analyses were made with the SAS statistical package V8e (SAS, Cary, NC, USA). For the present paper, analyses were made with χ2 test and with 5% as the chosen level of significance. The level of agreement between headache information attained by clinical interview and headache diary was evaluated with κ coefficient, sensitivity and specificity.
Results
Of the 106 subjects who received a diagnostic diary, 49 subjects (46%) returned it. Three of these found themselves unable to complete the diary due to work situation or illness other than headache. One subject missed so many answers in each recorded headache day that it was impossible to make any diagnoses. These four subjects were therefore excluded and 45 remained for the detailed analysis of the headache diagnoses.
The 45 subjects recorded a total of 413 headache days, of which six (from three different subjects) were not classifiable, because of one or more missing answers. Three subjects did not suffer any headaches during the registration period, while the remaining group recorded between one and 24 headache days per person, median nine headache days.
Responders and non-responders
The 49 responders had a mean age of 44 years, with a range of 26–70 years. The male:female ratio was 1 : 3.1. The lifetime prevalence for responders for tension-type headache was 92% (45 subjects) and for migraine 75% (36 subjects). Eighty-four percent (41 subjects) participated in the clinical interview and 16% (eight subjects) were interviewed by telephone.
In comparison, the 57 non-responders had a mean age of 42 years, range 26–69 years. The male:female ratio was 1 : 2.6. The lifetime prevalence for non-responders for tension-type headache was 96% (54 subjects) and for migraine 80% (45 subjects). Eighty-eight percent (50 subjects) participated in the clinical interview and 12% (seven subjects) were interviewed by telephone. The prevalence of migraine and tension-type headache was not significantly different between responders and non-responders (migraine P = 0.51, tension-type headache P = 0.55).
No significant difference in the number of headache days between responders and non-responders (migraine P = 0.85, tension-type headache P = 0.38) was recorded (11).
Migraine
According to the clinical interview, 33 subjects were diagnosed with MA, MoA or migrainous disorder (MD). Of these, 28 also recorded at least one attack in the diary fulfilling the criteria for one of the migraine types MoA or MD. An additional three subjects had migraine attacks according to the diary alone (Table 1). The κ coefficient was 0.57, sensitivity 90% and specificity 64%.
Comparison of migraine diagnoses in clinical interview and headache diary

Sensitivity: 90% (28/31); specificity: 64% (9/14).
A total of 18 subjects recorded aura symptoms in the aura screening question in the diary, whereas only four subjects were diagnosed with MA in the interview, of whom three also reported aura in the diary. Only one subject was diagnosed coexisting MoA and MA in the interview.
The subject with MA in the interview but no aura or MoA in the diary only recorded one headache day – a tension-type headache – and had written ‘no aura’ in the diary.
Tension-type headache
In the interview, 42 subjects reported a tension-type headache, of whom 37 also recorded at least one attack in the diary fulfilling the diagnostic criteria for episodic tension-type headache, chronic tension-type headache or headache of the tension type not fulfilling the criteria for episodic or chronic tension-type headache. Only one subject had a tension-type headache in the diary without having reported tension-type headache in the interview (Table 2). The κ coefficient was 0.39, sensitivity 97% and specificity 29%.
Comparison of tension-type headache (TTH) diagnoses in interview and headache diary

Sensitivity: 97% (37/38); specificity: 29% (2/7).
Nine of the subjects with tension-type headache had chronic tension-type headache according to the interview, whereas only seven had chronic tension-type headache according to the diary. The last two were diagnosed with episodic tension-type headache in the diary, because their headaches occurred on less than half of the days in the registration period.
Headache induced by chronic substance use or exposure
Headache induced by chronic substance use was found in one subject according to the interview, and in another according to the diary. The subject diagnosed with medication overuse headache (MOH) in the interview recorded 10 headache days in the diary through a period of 12 days. In one of the headache days, there was no registration of drug use. A total of 17 g paracetamol was consumed in the remaining nine headache days. The subject diagnosed with MOH in the diary but not in the interview was using buprenorfin on a daily basis after a trauma and had no history of headache or analgesic use before the trauma.
Accompanying symptoms
The accompanying symptoms were compared in subjects with the same diagnosis in interview and diary. Regarding tension-type headache, there were only few differences, but there was a slight tendency towards underestimating the accompanying symptoms in the interview (Fig. 2). When comparing pain intensity recorded in the interview and diary in tension-type headaches, 12 subjects (32%) overestimated their pain intensity in the interview.

Comparison of accompanying symptoms in interview (I) and diary (D). Tension-type headache diagnoses.
As regards migraine, the differences were more marked, and in this case the accompanying symptoms were overestimated in the interview compared with the diary (Fig. 3). In 11 (39%) of the migraineurs less nausea was reported in the diary compared with the interview. Photophobia was less severe in 22 (79%) of the migraineurs in the diary compared with the interview and likewise phonophobia in 21 (75%) migraineurs. Pain intensity was also overestimated in the interview by 13 subjects (46%).

Comparison of accompanying symptoms in interview (I) and diary (D). Migraine diagnoses.
Compliance
Thirteen subjects recorded one or more headache days each that were not correctly completed, i.e. missing values or two answers to single questions. At the same time, all 13 subjects also recorded perfectly completed diaries on other headache days.
Overall, information about headache start and disappearance was not taken into account. A total of 22 subjects (45%) did not answer both these questions in every recorded attack, and therefore duration of attacks could not be recorded in this study.
Thirty-four subjects indicated use of analgesics in one or more of the headache days recorded in the diary. Two specified that they did not use any drugs, and with three subjects without headache, the remaining six subjects either did not use any drugs or did not mention its use at all in the diary. However, very few subjects specified consequent analgesic use in all their recorded headache days.
Discussion
The diagnostic headache diary is based on the first edition of the operational diagnostic criteria of the IHS (1). In a previous study of migraine and tension-type headache, the diary was found to be an important supplement to the clinical interview, especially in distinguishing between coexisting headache types, the frequency of the different types of headache and in recording drug consumption in patients with suspected drug overuse (8).
Despite thorough instruction on how to complete the diary and the fact that the subjects were familiar with the questions it contained, compliance proved to be a problem in the present study. Previous studies of different diaries have recorded problems of the same kind (2, 9). Twenty-seven percent of subjects recorded at least one headache day with missing or double answers to the questions concerning symptoms and accompanying symptoms. The problematic questions were mainly those concerning aggravation by routine physical activity and phonophobia. Also, the start and disappearance of headache were troublesome in the present as well as in other diary studies (3). It has previously been found that the duration of an attack is not essential in discriminating between different types of headache attack (13, 14), but it is useful information in the planning of an adequate treatment strategy in a clinical setting.
All subjects recorded headache days in the diaries, where all answers were completed perfectly, which indicates that the problem was not due to lack of understanding of the individual questions. More likely, the matters of accompanying symptoms are either more complicated or less important to the subjects, and therefore they may not pay as much attention to these questions as to those regarding pain symptoms.
In the majority of headache attacks, there were no records of drug consumption and we are therefore unable to conclude whether it was due to no drug use or to no reporting of drug use. An overall screening question, where it is possible to tick yes or no to drug consumption, may improve the value of the diary.
The participants were selected by the interviewer when the interviewer found it difficult to make a specific diagnosis on the basis of the history alone. The optimal study population is representative of the background population, but still has a high frequency of difficult diagnosed headaches. Including all subjects from the general population would have heightened the representativeness but reduced the usefulness of our observations, as most subjects assessed would be easily diagnosed regardless. However, only 46% returned the diary, which is less than in other diary studies (55–88%) (2–4). The low response rate in the present study decreases the possibility of generalizing and applying the results to clinical practice. To overcome these problems, it is necessary either to include all subjects from the population-based headache study or to motivate the participants more to complete their diaries.
Including the data derived from the 1989 cohort when utilizing all data obtained in 2001 as a cross-sectional sample of the Danish population in 2001 may have limitations due to bias depending on factors correlated to the previous survey. However, bias due to differential participation was minimized by inviting all subjects in the 1989 cohort, regardless of participation status in 1989. Moreover, the participants in 2001 derived from the 1989 cohort were representative of the study population with respect to age, gender and headache status. Thus, no evident bias was found.
In order to ensure a high participation rate in 2001, all subjects not responding to the invitation were contacted by telephone. The telephone interviews were conducted exactly as the face-to-face interviews, the only difference in headache assessment being the absence of a physical examination.
A physical and neurological examination rarely affect headache diagnoses in the general population due to relatively few symptomatic headaches in this setting. Moreover, the diagnostic clinical telephone interviews have been shown to have good validity and reliability when evaluated with clinical face-to-face interviews as the gold standard (15, 16). Thus, no differences in ascertainment by the two approaches are expected.
A further problem was the registration period. Several subjects recorded only one or a few headache days, making it impossible to diagnose coexisting headache types, drug overuse or chronic headache, and it is therefore recommended to extend the recording period in future studies to at least 2 months. On the other hand, such a long recording period may worsen the problems of compliance and lack of interest. Combining the diary with a calendar to mark headache days that are not recorded in the diary may give more precise information on the frequency of headaches.
The question in the diary concerning migraine aura is intended for screening purposes (8). It precludes the possibility of answering ‘no aura’, which could be useful because migraineurs with aura also experience some attacks of MoA and tension-type headache. In any case, the screening question recorded all subjects with an aura according to the interview, but also many other subjects without an aura. Subjects suffering from aura symptoms have probably already been diagnosed before or at the clinical interview, and therefore they know the symptoms. Subjects with no previous knowledge of aura are likely to have confused it with photophobia or premonitory symptoms.
Despite the fact that the study group included only subjects whom the interviewer found difficult to diagnose, the migraine diagnosis showed moderate agreement, with only few differences between interview and diary, thus both sensitivity and specificity is fairly high in migraine (Table 1). Migraineurs who were diagnosed in the interview and not in the diary can be explained by the relatively short observation period. Those migraineurs who were diagnosed in the diary but not in the interview were found among subjects with many recorded attacks in the diary, and with different combinations of symptoms. If this is a typical pattern for these subjects, it may be difficult to describe a typical, untreated attack, and it may therefore also be difficult for the interviewer to distinguish between these different headache types. These controversies and practical problems are all in favour of the use of a diagnostic diary.
A previous study of the validity of the present diagnostic headache diary reports episodic tension-type headache to be less frequent in interview than in diary (8). This was not the case in this study, as we noted a slight preponderance of episodic tension-type headache in the interview compared with the diary. Different interview methods, interviewers or study populations may explain this difference. The previous study also found a great discrepancy between interview and diary in the matter of chronic tension-type headache, with higher frequency of chronic tension-type headache in the interview. In the present study, there were only a few more chronic tension-type headache diagnoses in the interview than in the diary.
Subjects with migraine diagnosis showed rather marked differences in the accompanying symptoms in interview and diary (Fig. 3). In the interview, subjects were asked to describe a typical untreated attack, whereas the diary reports all types of attacks – treated as well as untreated. Therefore the symptoms may not have evolved to the same degree in the attacks described in the diary. Incomplete memory causing bias towards the more severe headache attacks could also be part of the explanation.
Despite the low response rate and the rather small groups of participants, it is possible to conclude that a diagnostic headache diary may be an important supplement to the clinical interview when discriminating headache disorders as migraine and tension-type headache. In particular, patients with a complicated headache history at the clinical interview can benefit from the use of a diagnostic diary for at least 1 or preferable 2 months. Thorough instruction in the practical use of the diary is important, however, but we find that the diary is mandatory for the diagnosis of frequent coexisting migraine and tension-type headache as well as for MOH. Therefore, the diary complements the clinical interview and can be recommended for further research and clinical use.