
Abstract
Migraine with aura (MA) is associated with changes in cerebral blood flow (CBF), whereas the role of cerebral autoregulation is uncertain. This study aimed to evaluate basal CBF, cerebral blood volume (CBV) and vasomotor reactivity (VMR) in MA patients. Twenty-one controls and 16 MA patients (eight with side predominance) underwent simultaneous examination of flow velocity in the middle cerebral arteries by transcranial Doppler (TCD) and of near-infrared spectroscopy (NIRS) parameters [oxygen haemoglobin saturation: oxygen%, and total haemoglobin content (THC)] at rest and after hypercapnia. Cerebral VMR, THC and oxygen% increases were significantly greater on the predominant compared with the non-predominant migraine side, with both sides of patients without side predominance and with controls. These findings suggest altered autoregulation in MA patients, possibly secondary to impaired cerebrovascular autonomic control. Simultaneous TCD and NIRS investigation could represent a non-invasive approach to evaluate cerebral haemodynamics at the cortical and subcortical level.
Keywords
Introduction
During migraine aura, cerebral blood flow (CBF) undergoes a sequence of changes, with vasodilation preceding oligoaemia and the development of neurological symptoms (1, 2). ‘Spreading oligoaemia’ (3) advances at the rate of 2–3 mm/min corresponding to the progression of a wave of short-lasting neuronal excitation that is then followed by prolonged depression of cortical neuronal activity, defined as cortical spreading depression (CSD) (4). Migraine aura is known to be caused by CSD (5).
During migraine attacks blood pressure autoregulation is normal in all brain regions; conversely, in hypoperfused brain areas the regional blood flow does not rise to match metabolic activation (carbon dioxide) (2). Other experimental studies have shown that CSD is followed by long-lasting hypoperfusion and impaired cerebrovascular reactivity (6). Regulation impairment is confined to the area of the oligoaemia, suggesting that blood flow variations are caused by changes in local metabolism. Between attacks migraineurs appear to have normal regulation of brain circulation. Nevertheless, there is evidence that regional CBF asymmetries are present in the headache-free interval of aura migraineurs (7).
Studies investigating CBF and vasomotor reactivity (VMR) in patients with migraine with aura (MA) using transcranial Doppler (TCD) have yielded contrasting results. Some have reported increased CBF in basal conditions (8, 9), whereas others have failed to document such a difference (10, 11). In addition, while some investigations have found decreased cerebral VMR to CO2 in the interictal period (12), most have described increased values (13–16). These findings suggest that in patients with MA there is an alteration of cerebral VMR.
Near-infrared spectroscopy (NIRS) is an optical method based on the measurement of near-infrared light that allows non-invasive assessment of real-time changes in cerebral haemoglobin (Hb) oxygen saturation, hence in cerebral blood volume (CBV) (17, 18). Because of its excellent temporal, though low spatial, resolution, NIRS has been employed to evaluate cerebral haemodynamics and oxygenation parameters in various pathological conditions (19, 20) and is a reliable technique to investigate cerebral VMR (21). With this aim, NIRS has also been applied to the study of migraine without aura during the interictal period (22, 23).
TCD and NIRS provide complementary data on CBF and VMR at different levels, the former by measuring changes in flow velocity in the middle cerebral arteries (MCAs), and NIRS showing variations in cortical arterioles and capillary blood volume (24). Together, the two techniques afford comprehensive evaluation of cerebral haemodynamics.
The aim of this study was to assess the haemodynamic changes elicited by a metabolic stimulus in the cortical vessels and MCAs of patients with MA. In this attempt, CBF, CBV and VMR were measured by performing TCD and NIRS simultaneously.
Methods
Twenty-one healthy subjects and 18 patients with MA diagnosed according to International Headache Society 2004 (25) criteria were enrolled in the study. Two patients were excluded because of inadequate MCA insonation through the temporal bone window. Monthly migraine attacks in the 16 patients were ≥ 2, with a clear side predominance in eight patients. All enrolled patients were studied during a headache-free period and had not taken drugs for migraine attacks in the previous week; all patients had discontinued prophylactic medications at least 1 month before the study. The baseline demographic and haemodynamic characteristics of controls and patients are reported in Table 1. Colour-coded duplex examination of cerebral vessels (Philips IUZZ, Philips Ultrasound Bothell, WA, USA) documented normal morphology and blood flow velocity in all enrolled subjects. Examination of circle of Willis vessels was performed by TCD (Multidop T DWL, Sipplingen, Germany) as described by Aaslid and collaborators (26). Patency of major collateral vessels—i.e. ophthalmic, anterior and posterior communicating arteries—was also evaluated.
Patients' characteristics
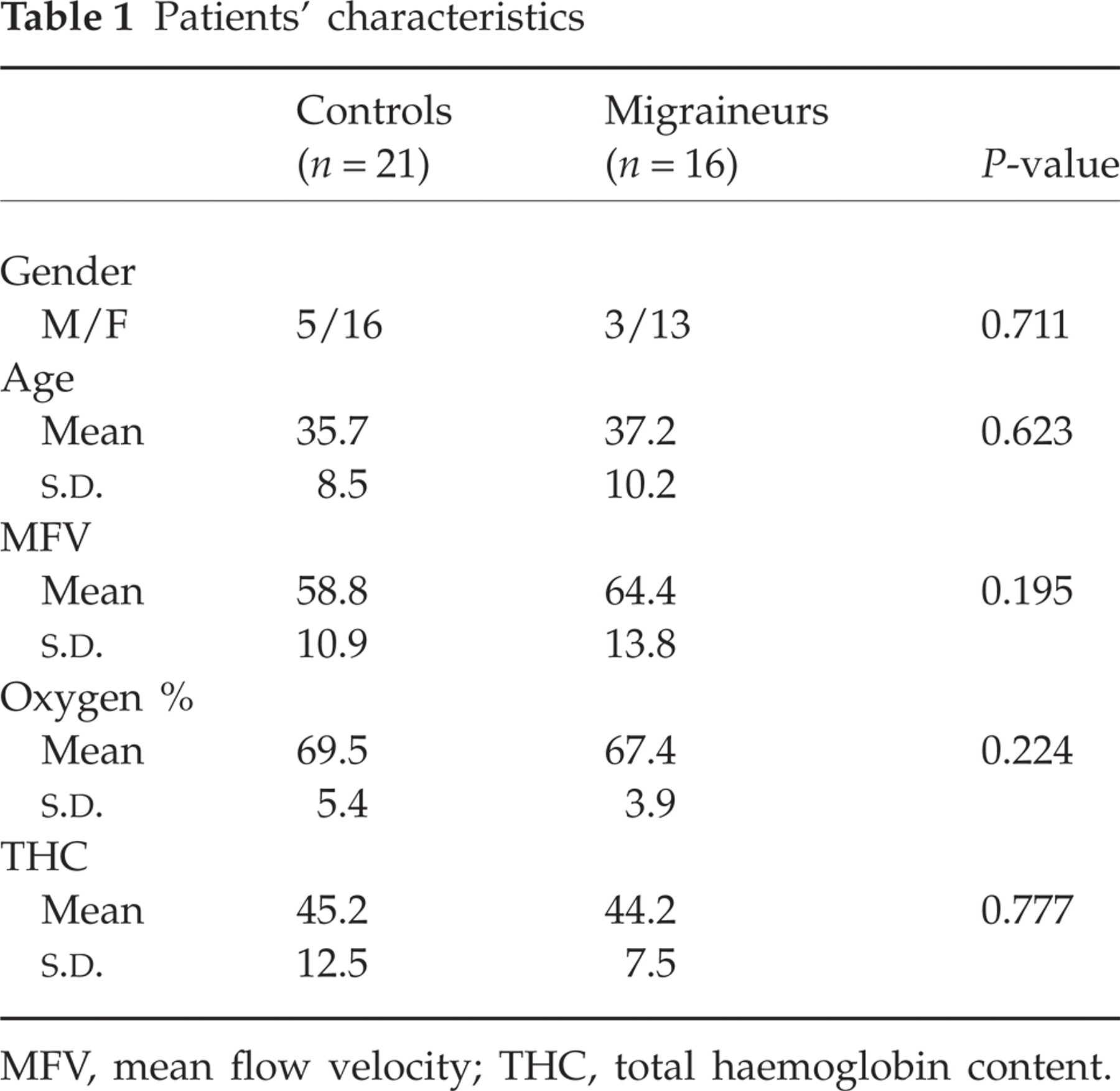
MFV, mean flow velocity; THC, total haemoglobin content.
NIRS measurements were conducted with an ISS Oximeter (Model 96208 Two-channel Non-Invasive Tissue Oximeter; ISS Inc., Champaign, IL, USA), which measures tissue oxygenated (oxyHb) and deoxygenated (deoxyHb) haemoglobin concentrations (27). The device works by delivering near-infrared light into tissue at four known distances (2, 2.5, 3 and 3.5 cm) from an optical fibre collecting the backscattered light. Light of two different wavelengths (750 and 825 nm) produced by solid-state lasers is modulated at a frequency of 110 MHz to allow measurement of phase and modulation of the collected light. From these raw data the absorption and scattering coefficients of the medium are determined. After application of the assumption that haemoglobin is the only significant absorber, oxyHb and deoxyHb concentrations are calculated.
Oxygen haemoglobin saturation (oxygen%) and total Hb content (THC) were obtained from the concentration of oxy and deoxy species, respectively:


OxyHb, deoxyHb and THC concentrations are expressed in μmol.
Simultaneous examination with TCD and NIRS was conducted at rest and after inhalation of a mixture of 7% CO2/air. During the experiments, end-tidal expiratory CO2 was measured with a capnometer (Drager Capnodig, Lübeck, Germany). Mean arterial blood pressure (MBP) was measured with a blood pressure monitor (2300 Finapress, Ohmeda, Louisville, CO, USA). Changes in MBP recorded after hypercapnia were slight (2–4%).
Two TCD dual 2-MHz transducers fitted on a headband and placed on the temporal bone windows were used to obtain continuous bilateral measurement of mean flow velocity (MFV) in the MCAs at a depth of 50 ± 4 mm. Two NIR optodes, each consisting of four light-radiating fibres and one light-collecting fibre, were placed symmetrically on the frontotemporal region and attached with the headband.
Each examination consisted of three consecutive phases: a 60-s rest period, a 90-s CO2 inhalation period—always including for each patient a 30-s period in which MCA velocity became stable (plateau period)—and, finally, a 90-s recovery period. Each experiment was performed at least three times at intervals of no less than 10 min. Data from the three experiments were averaged for each patient. The TCD and NIRS baseline values were taken as the average of the rest period (60 s). The TCD and NIRS parameters after CO2 stimulation were the average of the plateau periods and were obtained according to the formula:

For TCD recordings, VMR was considered as the relative change in MFV; for NIRS recordings it was considered as the relative change in THC, oxygen%, oxy-Hb and deoxy-Hb values (24).
The study was approved by the local ethics committee. All subjects gave their informed written consent.
Statistical analysis
Comparisons between patients and controls were evaluated by analysis of variance and the χ2 test, where appropriate. Given the small size of the groups of migraineurs with and without a predominant migraine side, no conservative post hoc procedure was applied and comparisons were performed by least significant differences (exact P-values were reported). Checks for Gaussianity and homogeneity of variances were performed without finding clear deviations from these assumptions.
Finally, Pearson's r was used to verify the correlation between increments of blood flow velocity and total Hb.
Results
There was no significant difference in baseline demographic and haemodynamic characteristics between migraineurs and controls (Table 1). As regards poststimulus increases, VMR values were significantly different between patients and controls (respectively 60%,
Hereafter migraineurs were divided in two groups: eight patients with side predominance (six with right predominance) and eight without. The percent increases of TCD and NIRS values in the three considered groups are reported in Table 2.
Increases in TCD and NIRS parameter by group and predominant side

LS, left side; RS, right side; PS, predominant side; NS, non-predominant side; total haemoglobin content; VMR, vasomotor reactivity; THC, total haemoglobin content.
Correlation between TCD and NIRS parameters showed VMR to be significantly associated with increased THC (r = 0.43; P = 0.011) and oxygen% values (r = 0.45; P = 0.007). Figure 1 reports the scatter plot between MFV and both THC and oxygen% increases on the affected side of patients and on the left side of healthy subjects. Very similar results were obtained with the right side of controls.
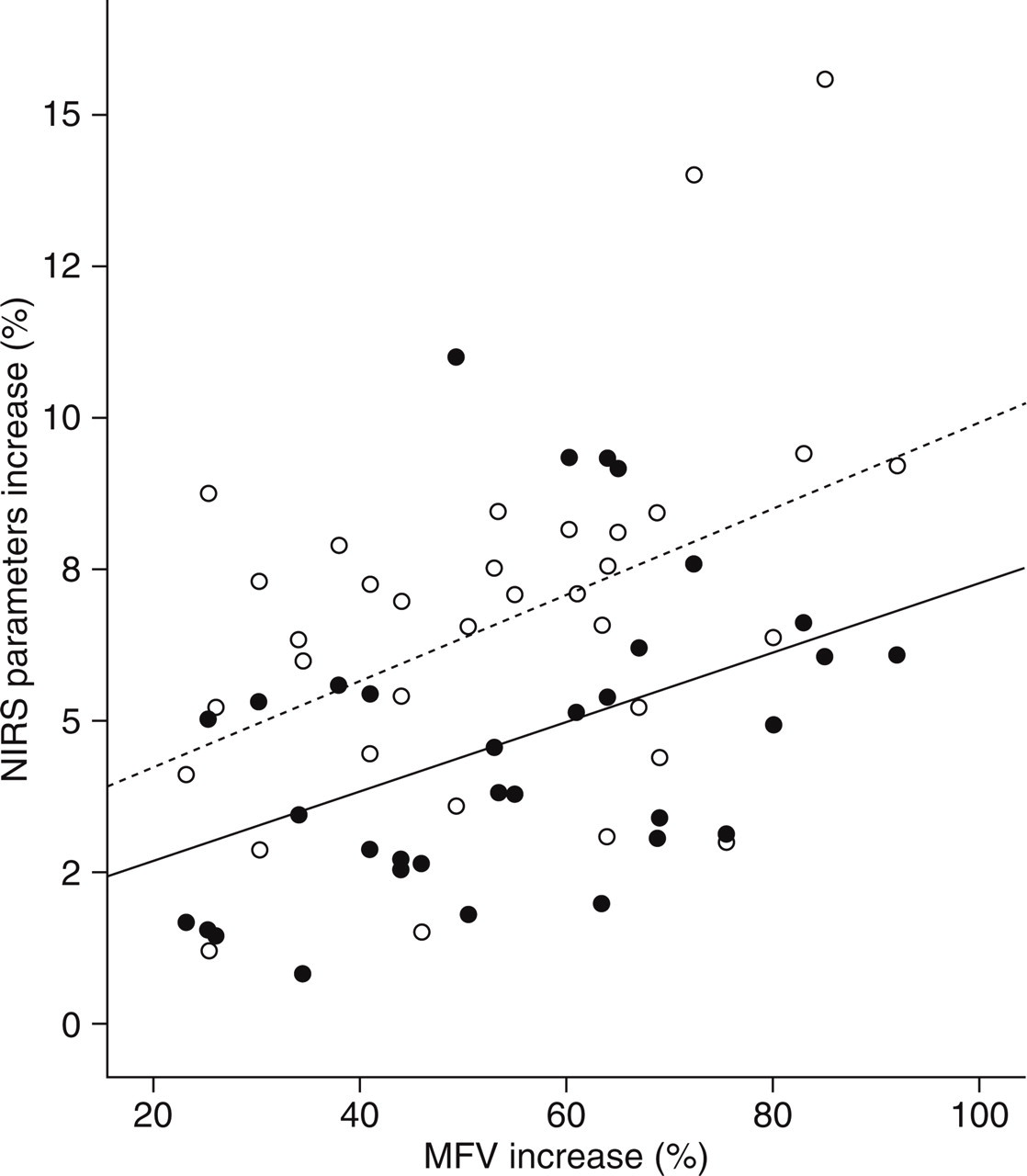
Scatter plot of near-infrared spectroscopy (NIRS) parameters (ordinate; closed circles, total haemoglobin content increase; open circles, oygen% increase) against transcranial Doppler (TCD) parameters increase [abscissa; vasomotor reactivity (VMR)]. The variance accounted for by VMR was 18.5% and 20.4%, respectively.
In both patients and controls, changes in MFV and NIRS parameters were short-lasting and returned to basal values in all subjects within 1 min from the end of hypercapnic stimulus.
Discussion
The present study has demonstrated that in the interictal period patients with MA have an increased cerebral VMR to CO2 measured by means of TCD and NIRS in the most frequent attacks side. Our results support the hypothesis that in migraine aura there is an abnormality of cerebral autoregulatory mechanisms. Simultaneous investigation with TCD and NIRS enabled for the first time detection of changes both at the subcortical level (by TCD) and in the cortical vascular district (by NIRS). However, in order to obtain these data we were forced to explore vascular territories not primarily involved in the pathophysiology of aura, since the NIRS technique is not suitable for exploration of the occipital areas.
According to most TCD studies, cerebral VMR is increased in patients with MA during the interictal period (13–16). On the other hand, previous studies, also by our group (10, 28), have failed to evidence significant changes in the autoregulatory mechanisms in the MCAs of MA patients. Here for the first time we used a powerful and prolonged metabolic stimulus to induce maximum arteriolar vasodilation. This probably accounts for the differences from previous investigations that used a less intense stimulus, such as voluntary apnoea. Moreover, given the high interindividual variability of migraine also in the pathophysiology of the different disease phases, patient clinical characteristics and time of the investigation are also liable to affect results. In this respect, patients included in the present study were characterized by a high attack frequency. This, together with the influence of their side predominance, may have caused further discrepancies.
To date, NIRS has been performed only twice to study CBV changes in patients exclusively affected by migraine without aura. In both studies, impairment of cerebral haemodynamics during the interictal phase was documented (22, 23).
In normal conditions, cerebral vessels are able to maintain constant and adequate cerebral blood flow and tissue perfusion over a wide range of perfusion pressures. At least three systems are implicated in controlling cerebral autoregulation: myogenic mechanisms, local chemical metabolic factors and cerebrovascular innervation, i.e. sympathetic and parasympathetic. While sympathetic innervation do not seem to play a relevant role in CBF regulation under physiological conditions, it does modulate autoregulation: a reduction in sympathetic activity shifts the lower limit of autoregulation to lower perfusion pressures, whereas increased sympathetic activity is responsible for the constancy of CBF even at higher ranges of perfusion pressure (29).
Lauritzen first demonstrated (2) that during migraine attacks blood pressure autoregulation is normal in all brain regions, but that following CSD metabolic autoregulation (CO2 reactivity) is impaired in hypoperfused compared with normally perfused brain regions. These findings suggest that the long-lasting oligoaemia arising after spreading depression may be induced by a vasoconstrictor stimulus capable of overriding the vasodilatory effect of an acid pH.
Excessive and asymmetric cerebral vasodilator responsiveness to CO2 has been detected in migraine patients compared with normal volunteers and with patients with headache other than migraine (30). This abnormality was significantly greater on the side of the most recent and most usual migrainous headache. Our study has confirmed this finding: higher values of VMR measured by TCD and of THC and oxygen% detected by NIRS were measured on the most frequent side of attacks. The excessive response to hypercapnia found in migraine patients can be best accounted for by hypersensitivity of adrenoceptor sites that is temporarily overcome by CO2 inhalation. Reduced receptor sensitivity to epinephrine and norepinephrine has been shown during hypercapnia (31). An asymmetric and excessive response at regional adrenoceptor sites may be a consequence of sympathetic dysregulation and could account for a genetically determined vasomotor instability first noted in migraineurs by Wolff (32).
Further findings support the theory of a sympathetic hyper-responsiveness in migraineurs. Using the cold pressor test, which induces a reproducible sympathetic stimulation, Micieli et al. (33) observed a different functional noradrenergic reactivity in migraine patients compared with healthy controls, i.e. increases in CBV and decreases in vascular resistance. They suggested that a peculiar neuronal/vascular reactivity in migraine may be the predisposing trait capable of precipitating attacks and the sensory, autonomic and behavioural phenomena that usually accompany neurovascular pain.
Additional evidence that migraine patients suffer from an autoregulation disorder has been reported by Nedeltchev and colleagues (34), who investigated flow response behaviour both in the MCAs and in the posterior cerebral arteries (PCAs) by applying visual stimuli during the attack-free period. While PCA blood velocity remained elevated throughout the stimulation period both in patients and in controls, MCA velocity failed to habituate to the stimulus in the migraineurs. Failure of the autonomic mechanism participating in the autoregulatory processes could be explain these findings.
Muller and Marziniak used frequency analysis of dynamic cerebral autoregulation to assess whether blood flow regulation disturbances may be found at the same frequencies of sympathetic and parasympathetic activity (35), and interpreted the impaired autoregulation observed in migraine patients as a possible lack of sympathetic and parasympathetic control of cerebral blood flow.
In conclusion, evidence from literature and from this study points to an autoregulation disorder in patients with migraine aura characterized by an excessive response of intracranial resistance vessels to metabolic stimulus. Further studies are needed to investigate whether these findings are simply epiphenomena or may have pathophysiological implications in MA.