
Abstract
The aim of this study was to describe the abnormalities associated with migraine aura lasting 1–24 h in children as shown by EEG, trancranial Doppler (TCD) and single photon emission computed tomography (SPECT). In this retrospective study, 11 patients each underwent EEG, TCD and brain SPECT on the day of admission and the day thereafter. On the day of admission, the migrainous hemisphere of all patients showed that the mean velocities were decreased in the middle cerebral artery by TCD, slow-wave abnormalities were recorded after several hours of aura by EEG and the SPECT showed hypoperfusion. On the day after, in the same hemisphere, slow waves were recorded only in the occipital area by EEG, and SPECT showed slight hyperperfusion. In these patients, there was a clear sequence of EEG, TCD and SPECT abnormalities.
Introduction
Research into the pathophysiology of human aura has been hampered by the episodic nature, short duration and unpredictable onset of migraine attacks. Many techniques have been employed, with variable success, to evaluate the relationships and the relative importance of neuronal vs. vascular factors associated with aura.
The migraine aura comprises a variety of neurological symptoms that appear gradually before or during the development of a migraine headache. In patients having a migraine with typical aura (MWTA), the duration of aura is usually 5–60 min according to the International Classification of Headache Disorders, 2nd edition (ICHD-II) (1), during which the EEG remains normal (2). The current neurogenic theory maintains that the aura is caused by a cortical spreading depression (CDS) (3). The most direct evidence of CSD in visual aura has been obtained by magnetoencephalography (4). The neuronal depolarization causes slow changes in direct current magnetic field potentials in patchy areas of the corresponding occipital cortex. Olesen and collegues (5) were the first to study cerebral blood flow during an attack of migraine with aura. They used intra-arterial 133Xe blood techniques to investigate the haemodynamic changes that occurred during aura-like symptoms induced by carotid angiography. They reported a succession of hypo- and hyperperfusion predominantly in the posterior part of the brain and usually lasting <8 h.
The single photon emission computed tomography (SPECT) technique has been used in a small series of patients (6). In most reported cases of MWTA, hypoperfusion occurred during the attack. More recently, positron emission tomography and blood oxygenation-dependent functional magnetic resonance imaging have provided the possibility of imaging the typical visual aura in migraine (7, 8). However, this technique does not directly record CSD. Transcranial Doppler (TCD) has also been used to investigate haemodynamic changes during MWTA, with controversial results (9, 10).
In sporadic hemiplegic migraine (HM), the aura lasts between 5 min and 24 h. This type of migraine is recognized by the ICDH-II if aura includes unilateral weakness. Some patients have aura lasting up 24 h but no weakness, and are often classified as MWTA, even if the criterion of duration of aura is not fullfilled. In these two types of patients, when the duration of aura is >1 h but <24 h (all the patients have a normal clinical status after a night's sleep), abnormal focal slow waves by EEG have been described (11), but the spatial and temporal distribution is not well known. Their relationships with vascular events have not been investigated.
Patients presenting with clinical manifestations of migraine aura with this prolonged duration are usually admitted to the paediatric emergency unit. Several investigations (EEG, TCD and SPECT) are sometimes performed to confirm the migraine-type neurovascular dysfunction. In this study, we report the retrospective analysis of these techniques in a group of such children.
Patients and methods
Between 1998 and 2004, 25 children (14 male and 11 female) aged from 8 to 15 years (mean 11 ± 2.4) were admitted to the paediatric emergency unit for migraine aura with a duration of >1 h but <24 h, with or without unilateral weakness. Adequate functional investigations for this retrospective analysis were available for only 11 of these 25 children. For the others, only clinical data were reported. None of the patients had mentioned a history of familial hemiplegic migraine or epilepsy. All had a normal brain computed tomography scan.
On the day of admission (D1), each patient had EEG, TCD and brain SPECT and the same investigations were repeated on the following day (D2). The migrainous hemisphere (MH) and the non-MH were defined according to the topography of neurological symptoms and the location of EEG abnormalities. The EEGs were recorded by 21 channels according to the 10–20 system. The TCD was performed with a 2-MHz probe. Mean velocities (MV) and pulsatility index were measured bilaterally on the middle cerebral arteries (MCA). The pulsatiliy index was calculated as the ratio: peak systolic velocity − end diastolic velocity/mean velocities and is considered as a measure of distal vascular resistance. The Wilcoxson test was used to compare MV and pulsatility index on MCA on the MH and non-MH. After injection of ethyl-cysteinate dimer (bicisate) (n = 10) or hexa-methyl-propylene-amone-oxime (exametazzime) (n = 1), the SPECT was performed on a dual-headed camera (DST-XL, GEMS). Projections were reconstructed using filtered back projection (gaussian filter: = 2.8). Five cerebral regions of interest (ROI) (calcarine, middle occipital, superior occipital, middle temporal and frontal) were drawn on each hemisphere using the Talairach atlas. The perfusion index were calculated for each ROI as the ratio of cortical perfusion/cerebellum perfusion. Analysis of variance were used to compare perfusion index between the MH and non-MH on D1 and on D2.
Results
Of the 11 patients who had had the above investigations, nine had visual symptoms, four had hemiparesis with homolateral numbness, three had aphasia and five had a decreased level of consciousness. The minimal duration of aura was 5 h. Of these 11 patients, six fullfilled the criteria of MWTA and three of sporadic HM. For two patients, this was the first attack of migraine with aura (MA), and they can be classified as having probable MA.
Of the 14 other patients, 11 had visual symptoms, three had unilateral numbness, two hemiparesis with homolateral numbness, two aphasia and five a decreased level of consciousness. The minimal duration of the aura was 4 h. Of these 14 patients, nine fullfilled the criteria of MWTA and one the criteria of sporadic HM. For four patients this was the first attack of MA.
All 25 patients had migraine headache during the attack. The maximal duration of the aura was sometimes difficult to determine, but after a night's sleep all patients felt well and had a normal clinical status.
On D1 (Fig. 1a), the TCDs of all patients showed a decrease of MV of MCA on the MH (mean 50 cm/s; SD 8.5), compared with the non-MH (mean 61 cm/s; SD 12.7; P = 0.04). In addition, the pulsatility index on the MH (mean 1.19) was increased compared with the non-MH (mean 0.92; P = 0.002). On D2 (Fig. 1b), the increase in MV of the MCA on the MH was not significant.

(a) Transcranial Doppler (TCD) on day 1 [mean velocity (MV) in the middle cerebral artery (MCA)]. (b) TCD on day 2 (MV in the MCA).
The EEGs of two patients were performed within 2–3 h of the beginning of aura (hemiparesia for one and visual symptoms associated with sleepiness for the other), and the results were normal. These normal EEGs were associated with a slowing on MCA and diffuse or focal hypoperfusion on MH (Fig. 2a). The EEGs of the remaining nine patients, which were performed after 3 h on D1, were abnormal and showed unilateral slow-wave abnormalities on the MH, temporo-occipital for eight patients (Fig. 3a), diffuse for one patient (Fig. 4a) and associated with hypoperfusion in the same area. On D2, the EEGs of all patients showed strictly occipital rhythmic slow-wave abnormalities on the MH with a good reactivity at the opening of the eyes (Figs 2, 3 and 4b). The MH of each patient was well defined by concordance between the topography, the type of neurological symptoms and the lateralization of EEG abnormalities.
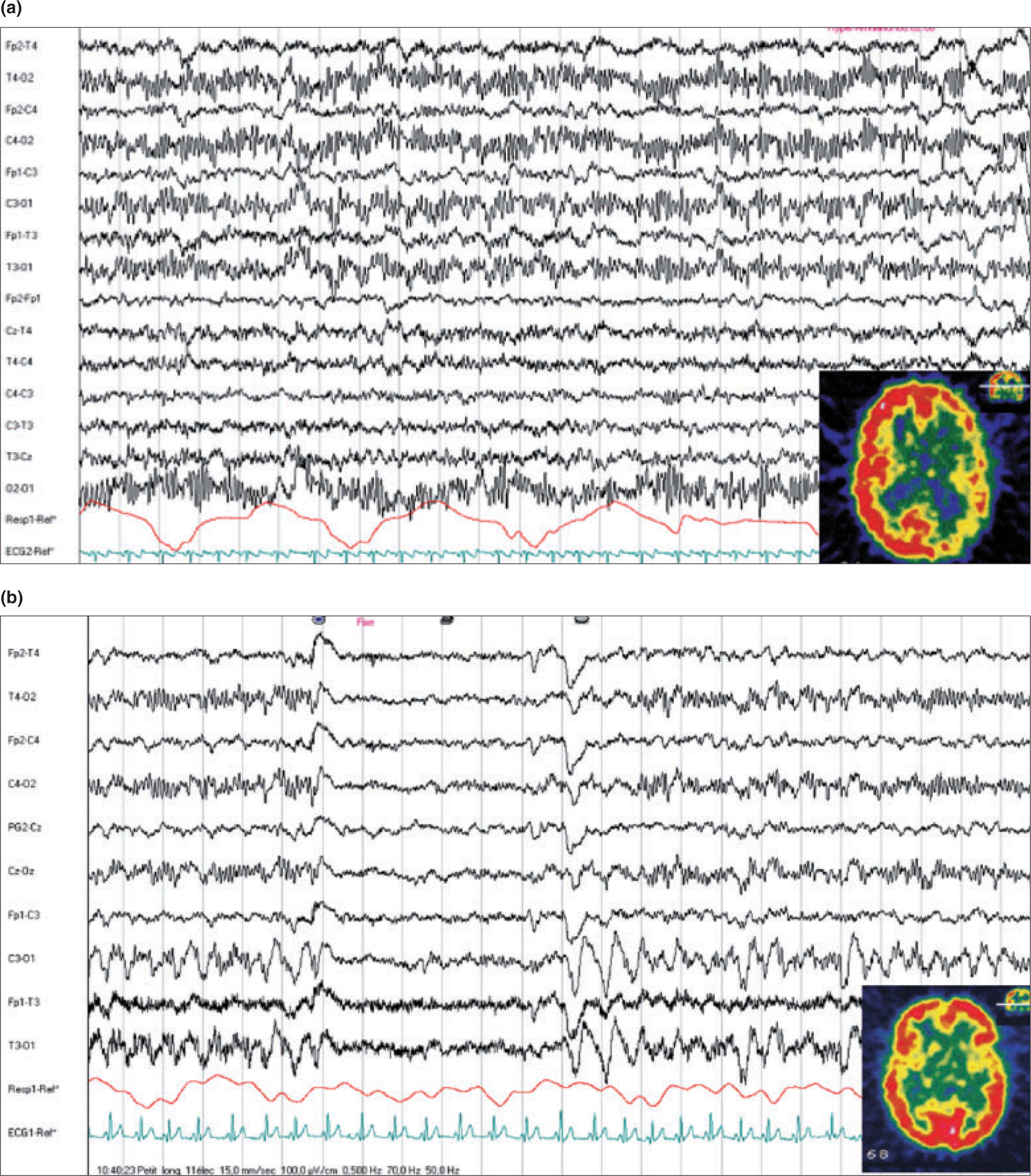
(a) EEG was preformed at 3 h (day 1) and single photon emission computed tomography (SPECT) at 4 h. Patient with right hemiparesis and headache: the EEG was normal and the SPECT showed diffuse left hypoperfusion (20%). (b) The same patient on day 2 with high-amplitude EEG slow-wave abnormalities in the left occipital area and 14% hyperperfusion in the left occipito-temporal area by SPECT.
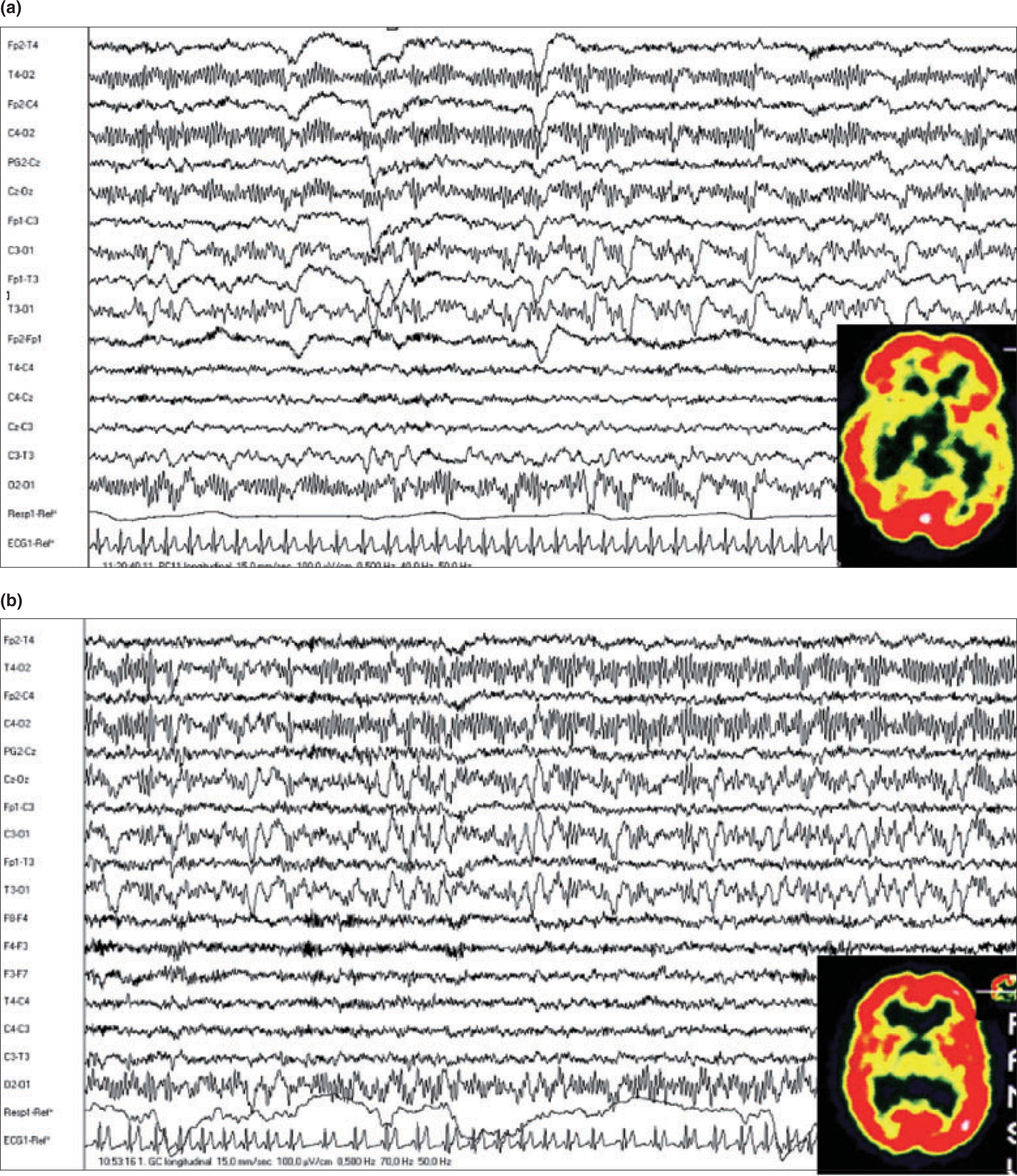
(a) Another patient with aphasia and headache on day 1. The EEGs were performed at 7 h with left temporo-occipital slow-wave abnormalities associated with hypoperfusion on the same area [single photon emission computed tomography (SPECT) at 12 h]. (b) The same patient on day 2: strictly left occipital EEG slow-wave abnormalities with left occipito-temporal hyperpufusion on SPECT.
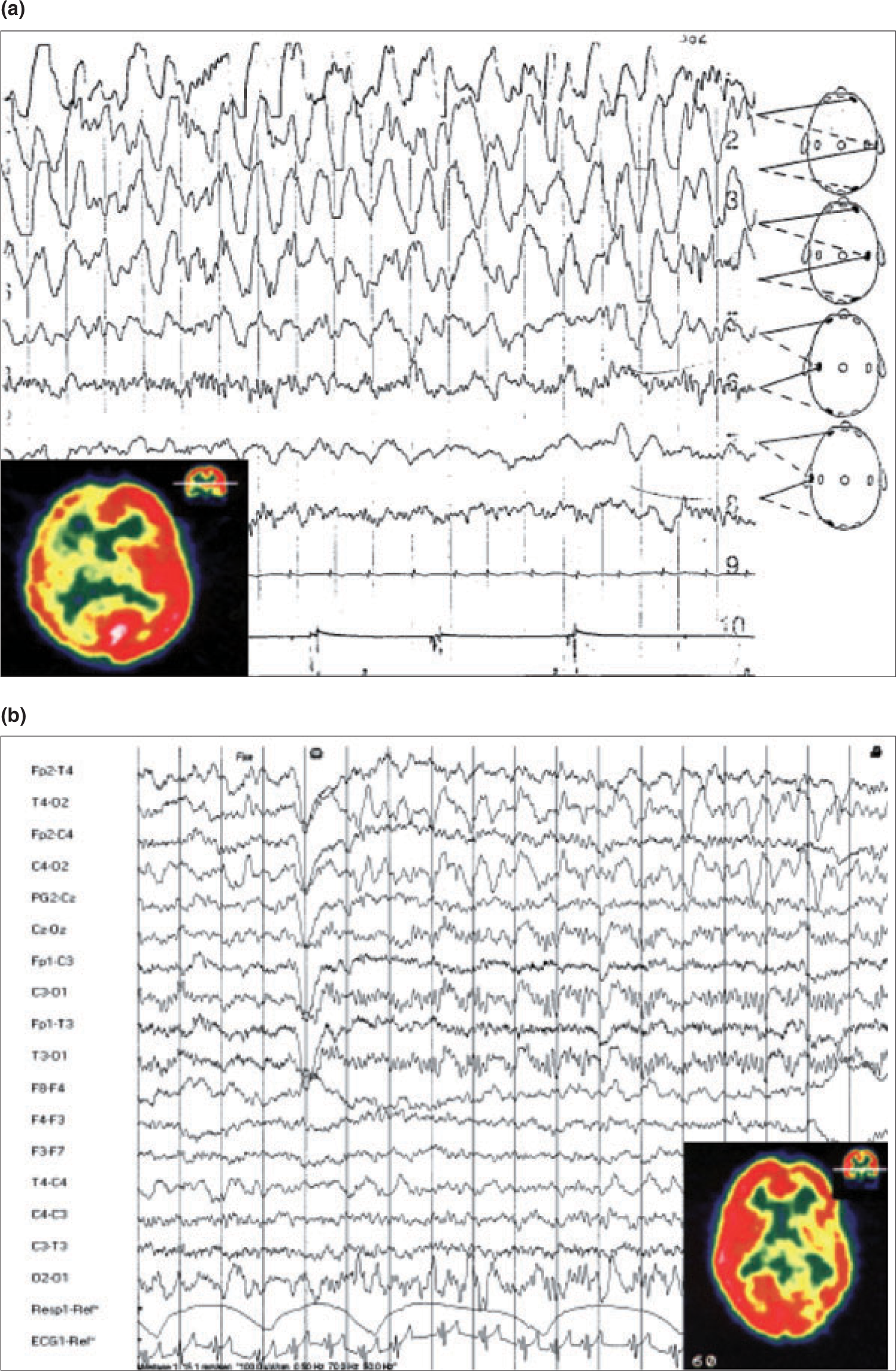
(a) Patient on day 1 with right high-amplitude diffuse EEG slow-wave abnormalities and diffuse hypoperfusion in the same hemisphere. (b) Same patient on day 2: right occipital EEG slow waves with hyperperfusion in the same hemisphere.
On D1, the SPECT of each patient showed hypoperfusion in several ROI on the MH compared with the non-MH. The mean perfusion index of each of the four occipital and temporal ROIs of the MH were significantly decreased (−13% to −15%; 0.0014 < P < 0.0076) on D1 and significantly increased (+6%; 0.0021 < P < 0.01) on D2. A comparison of the perfusion index on DI with those of the D2 revealed a significant change in these four ROIs (+15 to +19%; 0.0001 < P < 0.0064) on the MH, but no significant change in any ROI on the non-MH. No significant changes were noted in the perfusion index of the bilateral frontal ROI.
Discussion
The time of appearance of EEG abnormalities in migraine aura has not been known until now, but the EEG is reported to remain normal in MWTA lasting 5–60 min (2). Of our patients, nine were recorded later than 3 h after the beginning of aura on D1 and EEG slow-wave abnormalities were always observed on the MH, either temporo-occipital or diffuse. In the two patients recorded earlier during the first 3 h, the EEGs were normal. Although the number of patients recorded during this period was small, it can be hypothesized that the EEG abnormalities appear between 1 and 3 h after the beginning of migraine aura. On D2, the EEG slow-wave abnormalities were observed only in the occipital area of the same hemisphere and were associated with a normal clinical status.
In rats, CSD can be observed by application of potassium chloride on the cerebral cortex. The electrocorticogram records first an electrical silence, followed, some minutes later, by abnormal slow waves before complete restoration. Several waves of depressed neuronal activity are propagated across the brain cortex at 2–3 mm/min and associated with a reduction in cerebral blood flow. At the beginning of human aura, the electrical volume of conduction of CSD is too small to evoke EEG abnormalities, but sufficiently large to be detected by magnetoencephalography and to cause neurological symptoms. The slow-wave abnormalities appear after several hours, probably due to the increase in the area of electrical volume of conduction of CSD. These slow waves are probably the direct expression of the restoration phase of CSD. The localization of EEG abnormalities on D2 in the occipital lobe of the migrainous hemisphere in each patient is perhaps due to a particular predisposition of this brain area to CSD.
According to the literature and our data, the hypoperfusion seems to appear very soon in aura. This hypoperfusion is under the threshold of ischaemia and not severe enough to cause clinical symptoms. It is classically admitted that the hypoperfusion in aura is secondary to CSD, although some contradictory data have been reported (12). In one of our patients, diffuse unilateral hypoperfusion was associated with a controlateral hemiparesis and a normal EEG during the first hours of aura. The areas of spreading depression were probably too limited to cause EEG abnormalities and diffuse hypoperfusion. Some brainstem nuclei may have a role in triggering the hypoperfusion.
According to these data, there is a clear sequence of EEG, TCD and SPECT in migrainous aura lasting 1–24 h. In clinical practice, the use of EEG and TCD may be enough to identify the neurovascular events in these types of patients, but the timing of the recording is crucial.