
Abstract
This systematic review evaluates the strength of the evidence for the role of cervical musculoskeletal dysfunction in migraine. In this review, cervical musculoskeletal dysfunction will refer to the abnormal sensory afferentation from cervical region structures contained within the receptive field of the trigeminocervical nucleus. Electronic database searches using MEDLINE, PubMed and CINAHL were performed, and 17 studies investigating cervical musculoskeletal dysfunction in people with migraine were selected for review. The methodological quality of the included studies was assessed by two independent reviewers using a customized checklist. The review found that intersubject differences were inadequately reported and controlled, which resulted in grouping of participants with varying pathologies and symptoms. A diverse range of assessment procedures was used by the reviewed studies, which made comparison of their findings difficult. The assessment procedures were mainly used to quantify the degree of cervical musculoskeletal dysfunction, rather than to identify a cause and effect relationship between cervical structure and migrainous pain. Although animal study evidence proposes a role for cervical musculoskeletal dysfunction in migraine, this systematic review of the literature found that there is currently no convincing evidence to confirm this phenomenon in humans.
Introduction
This systematic review of the literature investigates the role of cervical musculoskeletal dysfunction in the pathogenesis of migraine. The potential for cervical dysfunction to manifest as headache is recognized under the classification of cervicogenic headache (1). The pain in cervicogenic headache is typically perceived within the dermatomes of the trigeminal and upper cervical (C2,3) nerves (2–7). The mechanism by which a cervical source of pain may be expressed as a trigeminal site of pain involves activation of the trigeminocervical nucleus (TCN). The TCN represents an area of overlap between the spinal trigeminal nucleus pars caudalis and the cervical dorsal horn above the level of C3 (2–4, 8, 9). Second-order nociceptive neurons within this area receive primary afferent input from both trigeminal and upper cervical (C1-3) nerves (2–4, 8, 10). This convergence of afferents then creates potential for the source of pain being misperceived at higher centres. In this review, cervical dysfunction will refer to the abnormal sensory afferentation from cervical region structures contained within the receptive field of the TCN.
The pain in migrainous disorders is also perceived within the dermatomes of the trigeminal and upper cervical (C2,3) nerves, which requires activation of the TCN. Therefore, cervical structures within the receptive field of the TCN may theoretically be involved in migraine pathogenesis, although this proposal is not supported by contemporary migraine models (11, 12). The classification of migrainous disorders is based upon presenting symptoms and their behaviour, rather than by identification of causative pathology (1). The relevance of cervical pain or dysfunction during a migrainous attack is subsequently unresolved, with logic suggesting that it could reflect pathogenesis, referred pain or comorbidity. Consistent with this logic argument, current evidence suggests that afferent input from cervical structures may be capable of facilitating the cranio-cervical pain associated with migraine (13, 14).
The proposed mechanism by which cervical afferent input can facilitate migraine pain involves central sensitization of the TCN. Persistent afferent discharge from dysfunctional cervical structures can evoke plastic changes in second-order nociceptive neurons within the TCN (15–19). These neurons could then have a reduced threshold to discharge or a capacity to respond to previously non-noxious input (19–21). If increased TCN reactivity reduces the threshold to migraine from its usual pathogenic factors, then the involved cervical structures have acted as facilitators. The neuroplastic changes could result from persistent input into the TCN by polymodal Aδ or C fibre nociceptive afferents or Aβ low-threshold mechanoreceptor afferents (10, 17, 19, 22–24). Therefore, a range of cervical musculoskeletal structures are capable of contributing to the TCN sensitization process.
The theoretical model that cervical afferent input is capable of facilitating migrainous pain is derived mainly from animal study evidence (14, 16, 25). However, anatomical differences in pain-processing systems between the species require that these data be interpreted with caution. Furthermore, as these studies utilized invasive procedures that cannot be ethically reproduced in humans, their findings are probably limited to hypothesis generation. Therefore, it is necessary to establish whether relevant studies involving humans with migraine have been conducted and to evaluate the strength of their evidence.
Relevant human studies must have assessed cervical structures from within the receptive field of the TCN. These structures include the C1–3 nerve roots and their branches, the O-C3 joints, the alar and transverse ligaments, the pre- and postvertebral muscles, trapezius, sternocleidomastoid, the cervical dura mater, and the vertebral and carotid arteries (3, 4). The purpose of this systematic review is to evaluate the evidence that supports or opposes a role for cervical musculoskeletal dysfunction in migraine. The findings will benefit practitioners treating migraine by providing the context for evaluating the clinical relevance of coexisting neck symptoms in their patients.
Method
Search strategy
An electronic search was performed in April 2006 using the following databases, MEDLINE (1966 to April 2006), PubMed and CINAHL (1982 to April 2006). Keywords used in the search strategy included migraine, cervical, neck, nerve block, tenderness, range of movement, mobility and proprioception. These keywords aimed to identify cervical musculoskeletal structures and their typical modalities of assessment. Additional purposive searching was also performed by an electronic search of relevant journals, and a manual search of the references from each included study.
Selection criteria
The titles and abstracts for each study within the search strategy yield were assessed for inclusion in the review. Studies were included if they were a full paper written in English, were descriptive studies, utilized people diagnosed with migraine, and measured cervical dysfunction. They were excluded if they investigated treatment efficacy, investigated secondary headaches (other than cervicogenic headache) or included children.
Quality assessment
The quality of the included studies was assessed in relation to study design, participant selection and description, experimental control, procedural efficacy and measurement validity and reliability. These domains were selected to appraise the internal and external validity of the studies. The quality assessment questions, decision criteria and scoring system are listed in Table 1. The score represents the number of quality criteria fulfilled by each reviewed study. As the criteria are not weighted, the score provides an indication of study quality, but not an absolute or relative value.
Quality assessment checklist

Data extraction
Details for each included study were extracted using a customised checklist derived from the quality assessment criteria described above. The checklist was developed to accommodate the unique methodological considerations of this subset of the literature. The checklist was trialled by the two reviewers to ensure parity in interpretation, and thus improve the reliability of the process. The data extraction was then completed independently by the two reviewers, with any discrepancies resolved by discussion.
Results
Search strategy yield
The search strategy identified 225 published studies. Following application of the inclusion and exclusion criteria, 17 studies (26–42) were selected for inclusion in the systematic review. These are briefly described in Table 2.
Summary of included studies
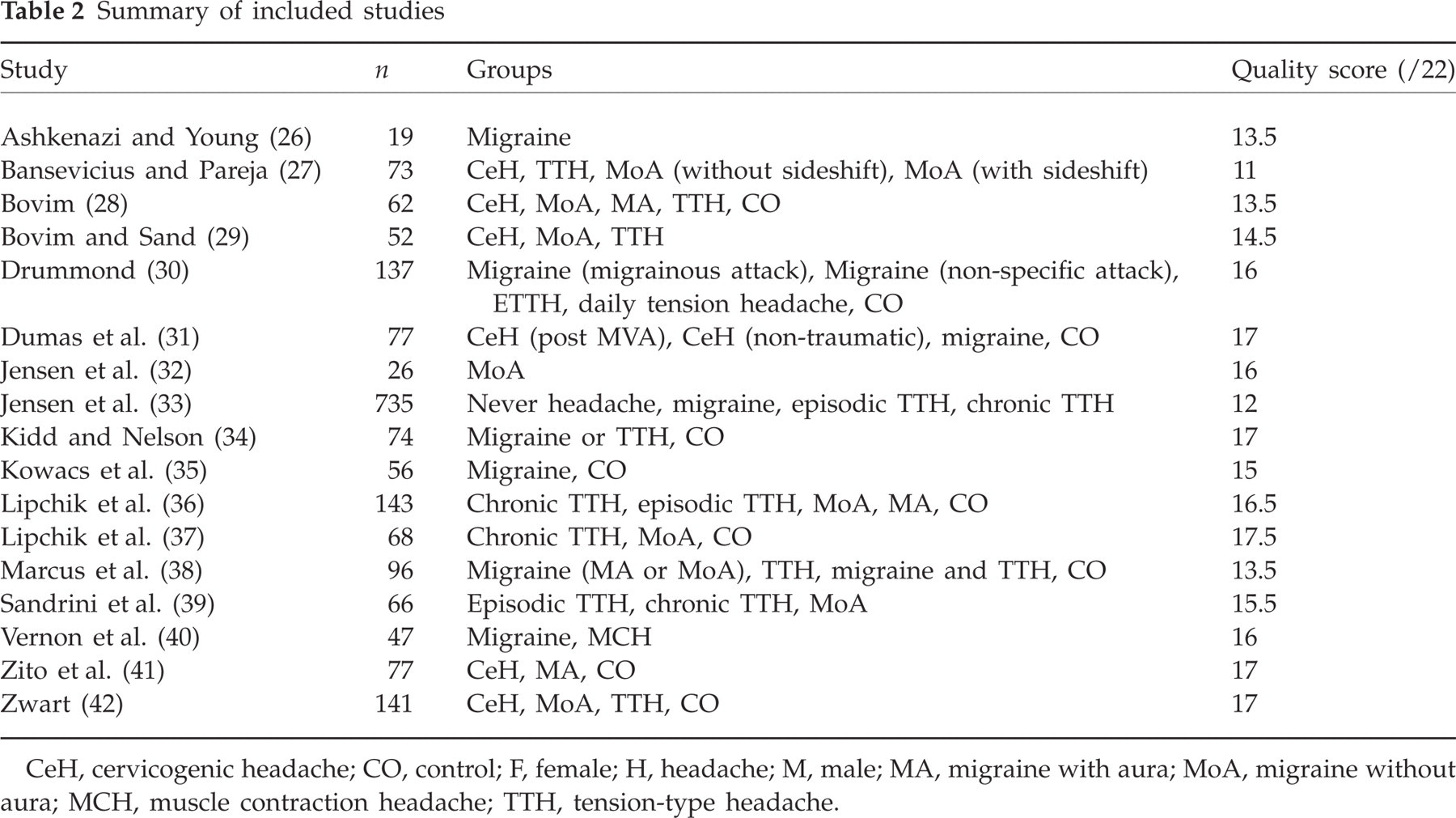
CeH, cervicogenic headache; CO, control; F, female; H, headache; M, male; MA, migraine with aura; MoA, migraine without aura; MCH, muscle contraction headache; TTH, tension-type headache.
Included studies
People with migraine were investigated as a symptomatic group in 10/17 studies, as a comparison group in 6/17, and as part of a population study in the remaining 1/17. A total of 573 people with migraine were included (469 female and 104 male). The sample sizes of the migraine groups ranged from eight to 70 with a mean of 25, and a median of 24. The mean age of the migraine groups was reported in 12/17 studies, of which 7/12 included standard deviation, and 3/12 included an age range. The mean age of the migraine groups, where reported, ranged from 23 to 43 with a mean of 36.5, and a median of 38 years.
Methodological quality of included studies
A summary of the extracted data is provided in the form of a quality score in Table 2. The majority of studies (16/17) clearly stated their research question, with all studies utilizing an appropriate design and cohort in consideration of their aims. The sampling method was stated in only 10/17 studies, with convenience sampling used to recruit symptomatic participants (6/10), and/or volunteer sampling (5/10) to recruit controls. The inclusion criteria were stated in the majority of studies (15/17), although the exclusion criteria were less frequent (7/17).
Subject characteristics
Twenty-two migraine groups were investigated across the reviewed studies, and were described as either migraine (8/22), migraine without aura (9/22), migraine with aura (3/22), or migraine/tension-type headache (2/22). Twelve studies reported at least one measure of the participant's headache history (i.e. location, frequency, duration, severity); however, only two studies reported detail of their participant's medication use. The headache and medication status at the time of examination was reported in only 11 and seven studies, respectively.
Experimental control
Methods employed to control intersubject differences included selection (15/17 studies), age matching (4/17), gender matching (5/17) and blocking (2/17). People with migraine were then compared with asymptomatic controls (12/17), other headache diagnoses (11/17), or within group only (4/17). During assessment, blinding of the examiner to the participant's diagnosis was employed in only nine studies.
Measurement procedures
A total of 36 measurement procedures were employed by the reviewed studies to identify some element of cervical dysfunction (Table 3). The majority of studies (16/17) adequately described these procedures and, additionally, their associated scoring systems. Only 5/17 studies provided adequate descriptions of their data recording systems. The majority of procedures employed demonstrated only face validity (20/36), with criterion (14/36) or construct validity (2/36) less frequent. Reliability was addressed in only 7/17 studies, with no study reporting reliability for all measurement procedures employed.
Findings of included studies (data for migraine groups only)


CCFT, craniocervical flexion test; CeH, cervicogenic headache; CO, control; CROM, cervical range of movement; CV, craniovertebral angle; EMG, electromyography; ETH, eye-tragion angle; H, headache; MA, migraine with aura; MoA, migraine without aura; NSD, no significant difference; PAIVM, passive intervertebral range of movement; PPT, pressure-pain threshold; ROM, range of movement; SD, significant difference.
Findings of included studies
The findings of each study that are specific to people with migraine are summarized in Table 3. A statistically significant difference was reported for 11/36 measurement procedures and no significant difference for 20/36. The remaining 5/36 procedures have no conclusion due to deficiencies in statistical method and/or reporting. The number of measurement procedures employed by the included studies varied between one and seven. Two studies (31, 41) which utilized people with migraine as a comparison group produced 12/20 non-significant findings, and thus may have skewed the results. When considered by study, 10/17 reported statistical significance, and 8/17 reported no significance for at least one measure.
Discussion
Included studies
The search strategy and systematic review criteria identified the subset of the literature which investigated cervical dysfunction in people with migraine (26–42). Of the 17 included studies, only 10 (26, 27, 29, 30, 32, 35, 38, 40, 42) identified people with migraine as a symptomatic group of interest. There was a broad range of assessment procedures employed by the included studies (Table 3), which perhaps reflects the structural and functional diversity of the cervical region. This disparity in method manifests as a challenge to the comparability of the studies within this literature subset, with the somewhat equivocal findings inhibiting a conclusion from being drawn.
Methodological quality of the included studies
Most of the investigations utilized appropriate study designs and participants aligned with their research aims. Where described, the recruitment of symptomatic participants mainly relied on convenience sampling. This could predispose to selection or experimental bias, as the participating clinics may themselves receive specific patient types based upon their expertise and treatments provided. Most studies used established diagnostic criteria (1, 43, 44) for participant selection or group allocation, with only one study (30) defining their own criteria. Although these criteria (1, 43, 44) provide a framework from which to operate, the diagnosis of migrainous disorders is based upon symptom behaviour rather than pathology. Subsequently, there is potential for a disparate group of people to be included under the same diagnostic title should these criteria be incorrectly applied. Even though 12/22 migrainous groups investigated were classified under the subtypes migraine without aura (9/22) and migraine with aura (3/22), the remaining groups were classified as ‘migraine’ (8/22), or as a component of a mixed headache (2/22). It is questionable whether the latter two groupings would include people with comparable clinical conditions. Furthermore, only 9/17 studies used examiner blinding, thereby increasing the risk of experimental bias.
Subject characteristics and experimental control
In the absence of an identifiable pathology the diagnosis and group allocation of people with migraine is dependent upon interpretation of symptoms (1, 43, 44). The classification of participants may reflect reporting behaviour rather than the magnitude of pathogenic factors. Therefore, researchers need to investigate and report adequate detail of participant characteristics to allow comparison. Although the age and gender profiles of the included studies were well described, the reporting of headache features and medication use was generally inadequate, both historically and at the time of examination. Thus, groups may include people with disparate severity and chronicity, and the interpretation of findings in the context of presenting headache symptomatology is impaired.
The application of strict selection criteria may reduce intersubject differences, although it can also reduce sample size and statistical power. With reference to people with migraine, the mean and median group sizes within the included studies were 25 and 24, respectively. These subjects demonstrated a broad age range, high female to male ratio, and potentially disparate symptom behaviour within the included studies. However, only a small number of studies employed blocking (27, 39) or matching (31, 34, 38, 42), with the control of extraneous variables being generally inadequate. A number of studies did not include asymptomatic controls (26, 27, 29, 32, 33, 39, 40) and/or did not perform any group comparisons (26, 32, 35, 40). Therefore, in the absence of control or normative data, it is not possible to conclude that any of the assessment findings demonstrate dysfunction.
Measurement procedure efficacy, validity and reliability
Evaluation of the validity of cervical dysfunction measures requires consideration of their rationale, tool validity and tester reliability. The theoretical rationale provides a framework by which the assessment findings are interpreted. Even though many measurement procedures were described in sufficient detail to enable replication, their rationale was less well defined. The procedures used across the reviewed studies included tests of cervical structure, function, or pain. The tests of cervical structure included joint mobility (31, 38, 41), muscle length (41), posture (31, 38, 40, 41) and range of movement (31, 34, 38, 40–42). The tests of cervical function included electromyography (39, 41), muscle strength (31) and proprioception (31, 41). These tests appear to be capable of identifying elements of cervical dysfunction, although the absence of comparison with usual migraine symptomatology prevents a cause and effect relationship from being demonstrated. These procedures subsequently rely upon the theoretical model of non-nociceptive sensitization of the TCN (15–21) to contribute to migraine pathogenesis or facilitation.
The tests of cervical pain included response to anaesthetic nerve blockade (26, 29), pressure algometry (28, 35, 39–41) and tenderness to manual palpation (27, 30–33, 36–40). Pain can be defined as ‘… an unpleasant sensory and emotional experience associated with actual or potential tissue damage, or described in terms of such damage’ (45, p. 21). The objective assessment of pain can be problematic, as intersubject differences may be due to reporting behaviour rather than differences in sensory stimulus. It is important for experimentally provoked or relieved pain to be compared with the usual migrainous pain, although this was achieved in only a small number of studies (26, 29, 30, 36–38). Should a test of cervical structure provoke the usual migrainous pain, then a pattern of referral or secondary hyperalgesia may be inferred. The headache status at the time of examination may also influence the assessment findings in terms of state-dependent sensory processing (10). During a headache-free interval, reduced input from migrainous pathogens may prevent a facilitative role of cervical structures from being demonstrated.
The previously described model of cervical facilitation of migrainous pain infers that the structures of interest are those which lie within the receptive field of the TCN. A number of studies adequately differentiate the sites within the TCN receptive field (26, 27, 29, 30, 32, 33, 35, 39, 41), although the remaining studies incorporate structures from either lower cervical (34, 40, 42), cephalic (28, 36, 37) or both (31, 38) regions. The value of the data from combined studies is impaired in relation to the facilitation model. These deficiencies in rationale are further compounded by varying levels of measurement tool validity and tester reliability. The majority of measures (20/36) demonstrate only face validity, questioning whether the data obtained accurately represent the structure tested. Only 7/17 studies report tester reliability for their procedures, with no study describing all measures. The implication is that the reproducibility of the results may be impaired. The procedural efficacy of the included studies must be considered when interpreting their findings.
Interpretation of findings of included studies
The statistical test results from the included studies require consideration in terms of methodology, participant characteristics and procedural efficacy to determine the utility of the study findings. The deficiencies in recruitment procedures increased participant heterogeneity, which was not reported or controlled. There was insufficient attention paid to headache status at time of examination, with procedural rationale failing to consider the influence of neural plasticity or state-dependent sensory processing. The majority of tests were intended to quantify some element of cervical musculoskeletal dysfunction, rather than to suggest a cause-and-effect relationship between cervical structure and migraine pain. The speculative role of cervical structures in migraine is as a facilitator. When migraine pathogens are subthreshold, it may be unlikely that any difference between people with migraine and asymptomatic controls would be detected.
A statistically significant difference was found between people with migraine and asymptomatic controls for EMG activity (39), posture (38), pressure algometry (41) and tenderness to manual palpation (27, 30, 36–38) (Table 3). Only four of these studies reported findings specific to structures within the TCN receptive field (27, 30, 39, 41), and of these only one (30) correlated the observed measures to the usual headache symptoms. This study (30) had limitations in recruitment and group allocation sufficient to challenge the internal and external validity of their findings. No difference was found for EMG activity (41), joint mobility (31, 38, 41), muscle strength (31) or length (41), pressure algometry (28, 39, 41), posture (31, 41), proprioception (31, 41), range of movement (31, 34, 38, 41, 42) or tenderness to manual palpation (31, 33) (Table 3). Only three of these studies reported findings specific to structures within the TCN receptive field (33, 39, 41), none of which equated the observed measures to the usual headache symptoms. The remaining findings (Table 3) were excluded due to the absence of comparison with asymptomatic controls (26, 29, 32, 35) or deficiencies in reporting (39–41).
Recommendations for future research
This systematic review has identified several deficiencies in study methodology that warrant consideration when planning future research. In order to investigate causality between cervical dysfunction and migraine, studies with prospectively collected data are required. The range of structures within the receptive field of the TCN implies that a number of physical tests are required to examine the region thoroughly, with single or reduced testing inadequate. The reproduction of usual migrainous symptoms during physical testing of cervical structures suggests cause and effect. This reproduction is more informative than simply quantifying the degree of cervical dysfunction alone, and is a necessary consideration for all studies. The headache status during examination may influence the physical test findings, owing to state-dependent sensory processing in the TCN and/or the level of input from migrainous pathogens into the TCN; hence the need for prospectively collected data. Ideally, participants would be tested both when symptomatic and symptom free to investigate this potentially confounding variable. Finally, the involvement of cervical structures implicated in migraine by physical testing is best confirmed using diagnostic anaesthetic blockade where possible.
Conclusion
This systematic review has confirmed that few human studies have investigated the role of cervical dysfunction in migraine. The available studies showed deficiencies in experimental methodology that prevented definitive conclusions from being drawn. Although the reviewed studies measured elements of cervical musculoskeletal dysfunction in people with migraine, many had methodological inadequacies. Most procedures used were intended to quantify a measure of cervical dysfunction, rather than investigate a cause-and-effect relationship with the migrainous symptoms. There was inadequate control of the headache status at the time of examination, which may have influenced the physical test results owing to state-dependent sensory processing in the TCN. Although a growing body of evidence from animal studies supports that cervical dysfunction may facilitate migrainous pain, this awaits verification in humans.