
Abstract
Objective
The aim of this project was to evaluate the prevalence and pattern of musculoskeletal dysfunctions in migraine patients using a rigorous methodological approach and validating an international consensus cluster of headache assessment tests.
Methods
A physiotherapist, blinded towards the diagnosis, examined 138 migraine patients (frequent episodic and chronic), recruited at a specialised headache clinic, and 73 age and gender matched healthy controls following a standardised protocol. Eleven tests, previously identified in an international consensus procedure, were used to evaluate cervical and thoracic musculoskeletal dysfunctions.
Results
Primary analyses indicated statistically significant differences across groups for the total number of trigger points, flexion-rotation test, thoracic screening, manual joint testing of the upper cervical spine, cranio-cervical flexion test, and reproduction and resolution. Ninety three percent of the assessed patients had at least three musculoskeletal dysfunctions. Post-hoc tests showed significant differences between episodic or chronic migraine patients and healthy controls, but not between migraine groups.
Conclusions
A standardised set of six physical examination tests showed a high prevalence of musculoskeletal dysfunctions in migraine patients. These dysfunctions support a reciprocal interaction between the trigeminal and the cervical systems as a trait symptom in migraine.
Introduction
Patients with migraine have a high prevalence of neck pain (1). Almost 70% of 487 participants of a recent survey reported neck pain prior, during, or after a migraine attack (2). However, the International Headache Society (IHS) considers neck stiffness or neck pain a symptom rather than a cause of migraine attacks (3). Albeit clinically more often present than nausea or vomiting, symptoms such as neck pain are not part of the diagnostic criteria (3) and are not sufficiently supported with evidence to influence the discussion regarding the pathogenesis of migraine, which is currently centered around central versus vascular origin. Migraine is understood as a neurobiological disease that possibly originates in the central nervous system, with key areas including the brainstem and the hypothalamus (4,5).
Following evidence from animal studies (6) and limited experimental research in humans (7,8), there is a close anatomical connection between the cervical and the trigeminal systems and thereby a likelihood of reciprocal interaction (trigeminocervical convergence theory). While this connection is recognised as an explanation for the development of neck pain associated with migraine attacks or for the pain relief after greater occipital nerve blockade (9), it is only discussed as causal in cervicogenic headaches (10) and headaches following neck injuries, for example attributed to whiplash associated disorder (11) or spinal pathologies (12). Nevertheless, given the correlation between neck associated disability and the frequency of migraine attacks, neck dysfunctions can be a potential risk factor for chronicity (13) and/or can act as triggers for migraine attacks (14).
If the neck plays a role in either pathophysiology, the chronification process, or as a trigger for migraine attacks, migraine patients should have a higher prevalence of musculoskeletal dysfunctions in the neck than headache-free participants. Current evidence for or against musculoskeletal dysfunctions in migraine patients is conflicting: While Jull et al. (2007) found no musculoskeletal impairment in migraine patients using a large range of physical tests that were evaluated by an examiner blinded towards the diagnosis in a sample of 196 volunteers (15), other authors have reported an inferior range of cervical motion (16,17), increased pericranial tenderness (18) and lower pressure pain thresholds (19), a greater number of active trigger points (16,20), posture changes (16) and findings on manual joint palpation (20).
The conflicting results and methodological problems such as sample sizes of seven up to a maximum of 22 migraine patients, unclear success of blinding, the use of only one or a small selection of tests, and the use of different classification approaches, do not allow for a firm conclusion regarding the prevalence and pattern of musculoskeletal dysfunctions in migraine patients. If this is not known, the rationale for physiotherapy is weak. Until very recently, there were no recommendations for which musculoskeletal tests should be evaluated in headache patients in daily clinical routine. An international consensus procedure resulted in 11 clinically useful tests (headache assessment tests (HATs)) to detect musculoskeletal dysfunctions in headache patients (21). However, this recommendation has not yet been validated.
The objective of this study was, therefore, to evaluate the prevalence and pattern of musculoskeletal dysfunctions in migraine patients compared to healthy controls by using a rigorous methodological approach including examiner blinding, diagnosis according to the most recent version of the IHS classification, appropriate sample size and an international consensus cluster of HATs (21). For this purpose, musculoskeletal test results were analysed for statistically significant differences across groups, and a cluster of tests that best characterises migraine patients was identified. The null hypothesis was that migraine patients do not show more musculoskeletal dysfunctions than healthy controls.
Methods
In a case-control design, a physiotherapist (KL), specialised in orthopaedic manual therapy and headache management and blinded towards the diagnosis, examined patients with migraine and healthy control participants using a cluster of tests that were previously identified in an international consensus study as the most clinically useful physical examination tests for the assessment of musculoskeletal dysfunctions in patients with headaches (21).
Participants
Patients were recruited at a university hospital headache clinic in Germany and diagnosed by a neurologist (AM) specialised in the diagnosis and management of headache patients according to the IHS classification version III beta (3). All consecutive patients attending the headache clinic between 01.12.2015 and 01.10.2016, and fulfilling the eligibility criteria but none of the exclusion criteria, were invited to participate; control participants responded to an online advertisement. To allow for investigator blinding, patients and control participants were contacted by a third researcher who provided information on the trial and arranged the appointments. All participants were advised not to reveal their diagnosis until the end of the assessment.
Patients were included if they fulfilled all the following eligibility criteria:
Age > 18 years A minimum of two years of migraine diagnosed by a medical specialist for the diagnosis and treatment of headaches according to the IHS classification version III beta. Although the diagnosis of migraine is accepted after five episodes fulfilling the IHS criteria for migraine, this minimum duration was chosen to allow for better estimation of attack frequency A minimum of six headache attacks per year. A minimum number of attacks was chosen to exclude patients who experience very rare migraine attacks No other relevant headache diagnosis (e.g. medication overuse headache)
Patients diagnosed with episodic migraine had to be headache-free on the day of the appointment and during the 48 hours prior to the examination. Chronic migraine patients were required to be migraine-free on the day of the appointment.
Control participants were defined as healthy persons with a maximum of two headache episodes per year that did not fulfill the criteria for migraine or any other primary headache type.
To avoid biased results due to pre-existing dysfunctions in the cervical spine or associated regions, or due to other diagnoses, patients and control participants were excluded if they stated that they fulfilled one of the following criteria:
Diagnosed pathology in the cervical spine (e.g. disc disease) History of trauma to the head or neck (e.g. whiplash associated disorder) Rheumatoid disease Craniomandibular dysfunction Other musculoskeletal, neurological, or psychiatric disease
Procedures
Prior to the physical testing, patients read the patient information sheet and had time for questions to the researcher before signing the informed consent form. They received a set of questionnaires to record demographical and migraine-specific data such as age, duration of disease, average pain intensity, headache days per months, migraine associated disability (MIDAS) (22), neck associated disability (NDI) (23), level of depression (PHQ-9) (24), and days since the last headache attack. Patients were contacted by email or telephone after one week to enquire about the date of the onset of the subsequent headache episode. Control participants answered only the questions on age, headache days per month, NDI and PHQ-9. All these tests were collected by the independent researcher to secure blinding of the investigator.
HATs were applied using the following procedures based on previous publications. Results were recorded on a pre-designed and pre-tested documentation sheet.
HFP: Using a CROM device with forward head arm (Cervical Range of Motion Instrument, Performance Attainment Associates, 1988, University of Minnesota), ventral translation was measured in centimetres using C7 as a reference point and maintaining neutral flexion/extension position.
The seating posture was standardised by returning to a relaxed position after two repetitions of maximum upright and maximum slouched position (25). Ventral translation of the head was recorded in centimetres.
AROM: Maximum active cervical flexion, extension, side-bending right and left, rotation right and left was recorded in degrees of movement with a CROM device (26). The total range of movement was determined by adding all measured values.
Upper Cx Quadrant: Upper cervical extension and rotation and ipsilateral lateroflexion were combined (27). This test was chosen as the key test to represent the category of combined cervical movements. Test results were documented as hypomobility (yes = 1; no = 0) and/or pain provocation (yes = 1; no = 0). The total test result was the score for hypomobility and pain combined for both sides.
PPIVMs: C0-2: Passive physiological flexion, extension, lateroflexion right and left, rotation right and left (27). Test results were documented as hypomobility or hypermobility (yes = 1; no = 0). The total test result was the score for hypomobility for both sides.
FRT: Degrees of passive and pain-free cervical rotation in maximum cervical flexion (28). Results were the combined degrees of movement for both directions.
Trigger point palpation: Trigger points were defined as a tender spot in a taut band in the muscle belly that resulted in a referred pain, either recognised by the patient as the usual headache (active trigger point) or referred into a non-headache region (latent trigger point). Four TPs in the sternocleidomastoid muscle sternal head, 4 TPs in the masseter muscle, 3 TPs in the temporal muscle, 2 TPs in the suboccipital muscles, 4 TPs in the trapezius muscle (29). The number of active and latent trigger points was recorded. The total score was the combined number of active and latent trigger points for both sides.
Muscle tests shoulder girdle: The upper trapezius muscle was chosen as the key muscle to represent the upper crossed syndrome (30). Active hold against maximum resistance with scapula fixation and without substitution of the rhomboids or latissimus dorsi was considered normal and given a value of 2, active hold was documented as a value of 1, no active hold was given a value of 0. The patient was positioned prone, the scapula positioned in neutral and the arm placed at 180° elevation (31). The documented score was the combined result for both sides.
PAIVMs: Central and unilateral posterior-anterior movement at C0-3 (27). The number of hypomobile and/or painful joints and movement directions was recorded. The total score was the number of hypomobile and painful joints combined.
Reproduction and resolution: Sustained unilateral posterior-anterior movement at C0-3 (32). If reproduction and resolution of headache symptoms was achieved, this was given a value of 1.
Thoracic screening: Active rotation right and left, extension; central and unilateral posterior-anterior manual joint palpation (27). Hypomobility or pain provocation was recorded as a clinical sign (with a value of 1). The number of clinical signs (maximum of 6: extension, rotation right/left, central PA, unilateral PA right/left) was recorded.
CCFT: Pressure Biofeedback Unit 20–28 mmHG; 10 second hold without substitution of superficial muscles (33). The mmHG value that was held for 10 seconds without substitution was recorded.
Statistical analyses of results
The sample size calculation was based on a medium effect size d = 0.5, 80% power and a Bonferroni-corrected alpha of 0.005 (0.05 divided by 11 tests). The required total sample size was 192 participants (G*Power 3.1). Differences between headache-free participants and patients with episodic and chronic migraine were calculated using either one-way ANOVA for interval data with Bonferroni corrected post-hoc t-tests, or the Kruskal-Wallis Test for ordinal data using Dunn’s Test for post-hoc analysis (34). For the binary test reproduction and resolution, Chi2 was used for the across-group analysis and the test of proportions for post-hoc analyses. The alpha level accepted for significance of the results was p < 0.005 (0.05 divided by the number of tests (a total of 11) to correct for multiple testing). To limit the number of comparisons to 11, a single score for each test was used for the primary analyses. Subsequently, exploratory analyses at a more liberal alpha level of p < 0.05 were conducted to differentiate, for example, active from latent trigger points (TPs) or right and left rotation for the flexion-rotation test (FRT). Further secondary analyses using logistic regression models were used to identify the cluster of tests that best characterises musculoskeletal dysfunctions in migraine patients and to identify whether test results are explained by any factor other than the diagnosis, such as age, NDI, MIDAS, PHQ-9, proximity of the last and the next headache attack, and headache days per month. All analyses were conducted using STATA 14 (StataCorp, Texas, USA).
Results
Demographic data and headache specific characteristics.

BMI: body mass index; NDI: neck disability index; MIDAS: migraine disability assessment questionnaire; PHQ: Patient Health Questionnaire; SD: standard deviation.
Differences across groups for each test.

CCFT: cranio-cervical flexion test; Cx: cervical; FRT: flexion rotation test; HFP: head forward posture; PAIVMs: passive accessory intervertebral movements; PPIVMs: passive physiological intervertebral movements; Q: quadrant; ROM: range of movement; SD: standard deviation; TPs: trigger points. *p < 0.05; **p < 0.01;***p < 0.001.
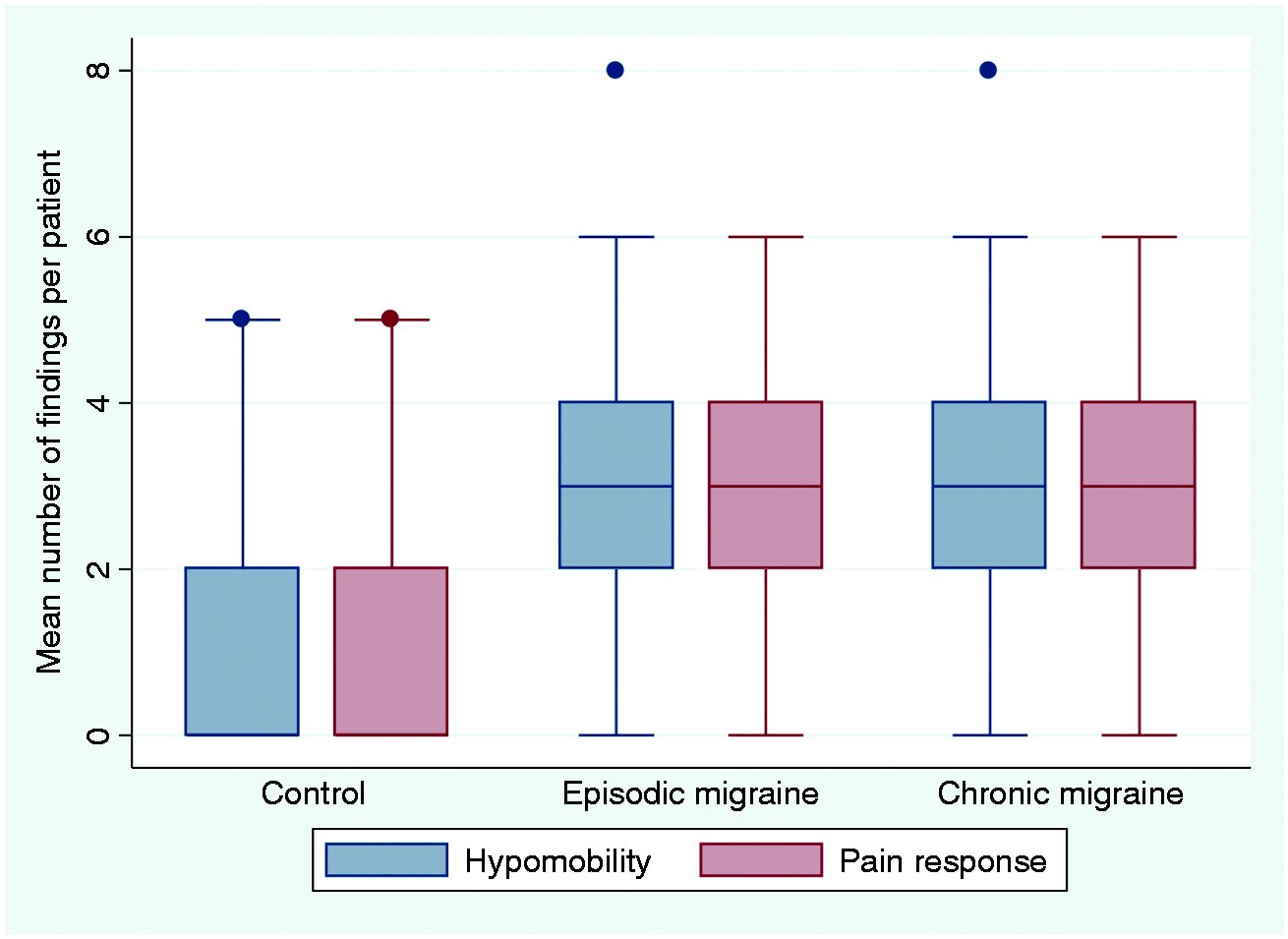
Secondary analyses for the six significant tests showed that active trigger points F(2,208) = 5.86; p = 0.003 as well as latent trigger points F(2,208) = 20.14; p < 0.0001 differentiated between migraine patients and headache-free participants (Figure 1). The FRT showed similar results for the right and the left side with F(2,208) = 6.83; p = 0.0013 and F(2,208) = 8.02; p = 0.0004 respectively. For the pain response to the FRT there was no statistically significant difference across groups H(2) = 3.646; p = 0.162. Thoracic screening consisted of active range of movement tests and passive joint mobility tests. Active tests alone were not statistically significant across groups with H(2) = 5.017; p = 0.0814; the combined result for hypomobility and pain response during passive thoracic joint mobility testing was H(2) = 19.336; p = 0.0001 (Figure 2). For cervical joint mobility testing, the results for hypomobility and pain response were identical across groups, indicating that hypomobile joints were generally perceived as painful and vice versa (Figure 3).
Between group differences in the number of active and latent trigger points. Between group differences in active thoracic and joint mobility. Between group differences in responses to manual joint testing of the cervical spine.

Logistic regression model (backwards and forwards selection) indicating the tests that best characterise musculoskeletal dysfunctions in migraine patients.

CCFT: cranio-cervical flexion test; FRT: flexion-rotation-test; PAIVMs: passive accessory intervertebral movements; PPIVMs: passive physiological intervertebral movements; TPs: trigger points; Tx: thoracic spine.

Graphical illustration of results from the logistic regression model to identify the tests that best described the musculoskeletal dysfunctions in migraine patients. The values indicate the odds ratios for each test.
A further regression model evaluating the influence of age, MIDAS, PHQ-9, proximity of the last or the subsequent headache episode, and NDI (migraine group only), indicated that none of these factors significantly explained the results of either of these five tests. The only significant result was found for headache frequency as a factor influencing the results of manual joint testing (p = 0.007, 95% CI −0.26; −0.42).
The most prevalent joint hypomobility was C1/2 on the left with 73% and 78% of the episodic and chronic migraine patients, respectively, showing a dysfunctional response compared to only 33% of the headache-free participants.
Discussion
The cluster of tests identified by international consensus as the most useful for the physical examination of headache patients (HATs) detected musculoskeletal dysfunctions that were more prevalent in migraine patients than in participants without headaches (except head forward posture). Only six (CCFT, TPs, FRT, PAIVMs, Thoracic Screening and symptom reproduction and resolution) of the original 11 tests reached statistical significance between migraine patients and headache-free volunteers. Ninety three percent of the assessed patients had at least three different musculoskeletal dysfunctions. There was no statistically significant difference between episodic and chronic migraineurs for any test except for the reproduction of headaches during manual pressure over a cervical joint (and subsequent resolution of symptoms during maintained pressure).
The HATs have been shown to be feasible to conduct. Approximately 30 minutes were required to perform all tests, proving practicability in the clinical setting.
The high prevalence of musculoskeletal findings in migraine patients are in contrast to two previous studies investigating musculoskeletal dysfunctions in patients with migraine, tension-type headache and cervicogenic headache (15,35), which did not find statistically significant musculoskeletal dysfunctions in patients with migraine. One of the two studies included very young migraine participants (mean age 23 years) (35) and both studies diagnosed cervicogenic headache according to the criteria published by the Cervicogenic Headache International Study Group (CHISG) (36). Although frequently used in cervicogenic headache research, comparing the CHISG and the IHS criteria will result in differently classified patients, since the CHISG allows CGH patients to have some of the criteria, such as nausea and vomiting, phono- and photophobia that the IHS describes as typical features of migraine. Studies investigating migraine patients compared to healthy controls using the IHS criteria reported musculoskeletal findings that are in line with the results from this present study (16,17,32).
The IHS classification version III beta describes neck muscle tension as a possible premonitory symptom of migraine (3). This is interpreted that neck pain is indeed part of the migraine symptomatology and not a consequence of posture or a potential independent neck pathology. Based on the findings from this study, neck pain is not simply a symptom of the migraine attack (as proximity of the last or the subsequent migraine attack did not influence the test result) but persists throughout the cycle and is reflected by changes in the musculoskeletal system that can be detected by physical examination tests.
Three different models could explain the higher prevalence of musculoskeletal findings in migraine patients:
Frequent migraine headache causes muscle tension in the neck, consequently resulting in joint dysfunctions due to, for example, reduced mobility Pre-existing cervical joint or muscle dysfunctions serve as a trigger for migraine attacks In a highly sensitive/sensitised system (migraine), pressure as applied during joint palpation or trigger point palpation is more likely to be interpreted as pain than in a non-sensitised system (healthy controls)
There is little evidence to support any of these hypotheses. Research on experimental tooth clenching indicates that muscle tension can indeed theoretically provoke joint pain (37,38), hence cervical joint pain might be caused by premonitory neck muscle tension. However, there are no studies suggesting that migraine patients have indeed a higher muscle tension. That pre-existing cervical dysfunctions might trigger migraine attacks has been hypothesised (14) and experimentally induced by sustained pressure on upper cervical segments (32), but the headaches that were provoked by the pressure resembled migraine attacks only in a minority of patients.
Central and peripheral sensitisation have been investigated extensively in the past (39,40) and partially explain increased pressure pain thresholds (41) in migraine patients and potentially higher numbers of trigger points or even pain response to joint palpation. Nevertheless, even a more sensitive system with a disposition to lowered sensory thresholds (42) cannot explain a reduced thoracic mobility or difficulties in the recruitment of deep cervical flexor muscles. Whatever the biological explanation, this significant clinical presentation of pain in the trigeminal and cervical innervation territories indicates a rather static trigemino-cervical interaction in migraine.
Whether the observed changes are the consequence of repetitive migraine attacks, or can trigger more frequent attacks, or both, cannot be determined from the current data. Although no statistically significant differences were found between episodic and chronic migraine patients – except for the reproduction of headache during manual palpation – there was a trend for most tests to higher levels of dysfunction in the chronic migraine group. To further clarify the influence of musculoskeletal dysfunctions on headache symptoms, a randomised controlled trial would be required that investigates whether a reduction of musculoskeletal dysfunctions (by e.g. manual therapy) will also result in a reduction of migraine intensity, frequency and duration.
Clinical implications from the present findings are that it is important to complement the migraine diagnosis (based on the patient interview) with a thorough physical examination to detect potentially treatable musculoskeletal dysfunctions. The type and severity of these dysfunctions will influence the decision on whether a physiotherapy intervention is indicated and what type of intervention (e.g. joint mobilisation, neck muscle strengthening) is the most promising approach.
Limitations of this study regarding the generalisability of the results due to the patient recruitment at a specialised headache clinic apply: Patients consulting headache specialists tend to be more disabled by the disease than migraine patients without special care. This is also the most likely explanation for the similarity of findings between episodic and chronic migraine patients in this sample. Episodic migraine patients in our sample had an average of seven headache days per month, ranging between 0.5 and 14 days. Particularly, those patients at the higher end of this scale cannot be considered biologically different from chronic migraine patients. Headache frequency and exclusion criteria such as diagnosed pathologies were based on a patient interview and not on a headache diary or medical notes. This may have added recall/reporting bias to the number of headache days per month and may have also led to the inclusion of some pathologies that were either unknown or not of relevance to the patient. However, most participants had unchanged symptoms for a number of years, and some participants kept a headache diary for reasons other than this study.
The level of inter-rater reliability has not been established for all included tests; therefore, to avoid the influence of inter-examiner differences and thereby introduce heterogeneity in the data, only one examiner performed the tests.
Migraine patients generally showed more tenderness in the neck region, hence the physical therapist might have guessed after the initial tests whether the participant was a migraine patient or a control participant. However, most patients concealed their diagnoses until the end of the examination and there were examples of control participants with extremely tender neck regions and examples of migraine patients who only responded to a small number of tests, therefore guessing did not result in unblinding. In a future project, it might be useful to compare two different headache types, e.g. migraine versus tension-type headache, to reduce the risk of unblinding after the intial tests and to gain further insight into the discriminative value of the tests to distinguish between different pathophysiologies.
In summary, using a rigorous methodological approach with more than 200 participants and validating an international consensus cluster of headache assessment tests, we found a robust high prevalence of musculoskeletal dysfunctions. These dysfunctions are not simply part of the headache attack, and our data suggest a reciprocal interaction between the trigeminal and the cervical systems as a trait symptom in migraine. A set of six physical examination tests is recommended as the minimum cluster to detect typical musculoskeletal dysfunctions in migraine patients that are potentially treatable by physiotherapy.
Key findings
Migraine patients showed significantly more musculoskeletal dysfunctions than headache-free control participants. Migraine patients presented higher numbers of trigger points, lower mobility of the upper cervical spine and a higher pain sensitivity to palpation of the upper cervical spinal joints, reduced mobility in combined flexion and rotation, reduced mobility of the thoracic spine, and less activation of the stabilising muscles of the cervical spine than healthy control participants.
Footnotes
Acknowledgement
The authors would like to thank Thomas Schoettker-Koeniger for support with the statistical analysis.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This study was supported by the German Migraine and Headache Society (DMKG) and International Maitland Teachers Association (IMTA) to KL and by the 7th Framework EU-project EuroHeadPain (#602633) to AM.
Ethical approval
Ärztekammer Hamburg PV5011
Trial registration
German Clinical Trial Register DRKS-ID: DRKS00009622