
Abstract
The aim of this review was to summarize population-based studies reporting prevalence and/or incidence of chronic migraine (CM) and to explore variation across studies. A systematic literature search was conducted. Relevant data were abstracted and estimates were subdivided based on the criteria used in each study. Sixteen publications representing 12 studies were accepted. None presented data on CM incidence. The prevalence of CM was 0–5.1%, with estimates typically in the range of 1.4–2.2%. Seven studies used Silberstein–Lipton criteria (or equivalent), with prevalence ranging from 0.9% to 5.1%. Three estimates used migraine that occurred ≥ 15 days per month, with prevalence ranging from 0 to 0.7%. Prevalence varied by World Health Organization region and gender. This review identified population-based studies of CM prevalence, although heterogeneity across studies and lack of data from certain regions leaves an incomplete picture. Future studies on CM would benefit from an International Classification of Headache Disorders consensus diagnosis that is clinically appropriate and operational in epidemiological studies.
Introduction
The term chronic daily headache (CDH) refers to a heterogeneous group of disorders characterized by headaches that occur ≥ 15 days per month. CDH has a population prevalence of 3–5% and is disabling for headache sufferers (1,2). CDH is also vexing for neurologists, as patients with these disorders are over-represented in neurological practice. Patients with CDH comprise approximately 40% of patients in headache clinic populations (3,4). For these reasons, neurologists are stakeholders in optimally defining CDH as a step towards improving its management. The most common form of CDH in patients presenting to headache clinics is a condition variously called chronic migraine (CM) or transformed migraine (TM) (3,4). Current approaches to the definition and classification of CM are the result of 20 years of evolution and changing perspectives.
A formal definition of CM was introduced by Silberstein and Lipton (S–L) (1994) (5), who used the term transformed migraine, originally coined by Mathew and colleagues (1987) (6,7), to describe patients with daily or near-daily headache with migraine episodes. The S–L definition emphasizes the evolving nature of the disorder; headaches typically begin with episodic headaches that transform into a pattern of daily or near-daily frequency (8). Although the International Headache Society did not recognize CM as a distinct disorder in the original International Classification of Headache Disorders (ICHD)-I (1988) (9), the ICHD-II (2004) (10) incorporated a definition of CM as a complication of migraine. The ICHD-II criteria were stricter than those proposed by Silberstein and Lipton, and required that migraine be present for >15 days per month, as opposed to headache for >15 days per month with a link to migraine. Furthermore, the ICHD-II did not incorporate a history of transformation since diagnosis is often made after the transformation. The ICHD-II definition also required that CM be diagnosed only in the absence of medication overuse [i.e. CM and medication overuse headache (MOH) are mutually exclusive] (5,8). In contrast, the S–L criteria provided definitions for two types of TM, those with and without medication overuse (11).
Although the ICHD-II criteria for CM were originally designed to apply to patients in tertiary headache centres, when applied to patients in clinical practice or clinical trials the criteria had low specificity and very few patients met the diagnostic requirements (12). To address this, the ICHD-II proposed revisions to the CM criteria, which were added as an Appendix to the ICHD-II. The resulting 2006 ICHD-IIR criteria required ≥ 15 days of headache with ≥ 8 days of migraine for at least 3 months and five or more previous migraine attacks (12,13). These proposed revisions are currently undergoing field testing (12,14). One field test demonstrated that 92.4% of headache clinic patients with TM without medication overuse met the ICHD-IIR criteria for CM, compared with only 5.6% using the original ICHD-II criteria (14).
In addition to definition variability, other factors limit our understanding of the epidemiology of CM (15,16). Samples derived from neurology or headache practices are very different from population samples. Furthermore, because the disorder is rare, very large samples are required to assess prevalence or incidence, particularly for age- and gender-specific estimates. Although the literature on migraine epidemiology and natural history and studies of chronic headache as a group have been reviewed (1,17,18), a more focused review of CM is timely. Given the evolution of criteria over time as well as potential regional variations in prevalence, summarizing the published literature would provide a comprehensive source of information for impending studies on CM. Thus, this systematic review was conducted to identify and summarize population-based studies reporting the prevalence of CM and to explore classification variation across studies that could be used to inform future epidemiological research.
Methods
Article selection
We conducted a systematic search of PubMed, Cochrane, and EMBASE databases to identify English-language articles reporting the prevalence and/or incidence of CM. Search dates ranged from 1 January 1990 through 17 July 2007. Detailed migraine search terms included chronic migraine, transformed migraine and frequent migraine, as well as epidemiological terms such as burden, prevalence and incidence. Related headache terms were also included (e.g. chronic headache, chronic daily headache, chronic tension-type headache) to capture estimates of CM that were reported in or could be calculated from more general studies of chronic headache (see Appendix A for full search criteria). Reference lists of relevant publications and review articles were reviewed for additional studies that may not have been captured by the database search.
Studies were included if they were: (i) population-based (e.g. random/cluster samples, surveys of whole populations, or general practice populations in countries with nationalized healthcare systems); (ii) conducted in adults (or a mix of adults and adolescent subjects, with the caveat that the inclusion of a small percentage of adolescents might attenuate estimates); and (iii) reported prevalence and/or incidence estimates for CM (or provided adequate information to calculate estimates). Articles were excluded if: (i) the study design was not appropriate (e.g. case–control studies); (ii) no specific data were provided on CM (e.g. general migraine only); (iii) the study was not population-based; (iv) the study population was restricted to individuals with CM (e.g. studies assessing quality of life); or (v) results were provided only for adolescents or children.
While reviewing studies, we noted a great deal of heterogeneity in terms of criteria and terminology employed. For example, overlap in headache frequency existed in studies termed frequent migraine and chronic migraine. In order to ensure review of studies using various definitions of ‘chronic’, we assessed studies that defined a group of ≥ 10 headaches per month as well as studies that addressed ‘daily’ headache without a specific quantitative cut-off point. Thus, we included studies that examined chronic headache with migraine as well as chronic migraine. Even though we used a relatively liberal definition of chronicity to identify studies for inclusion (i.e. 10+ migraines per month), the studies identified in this review typically defined chronicity of headache or migraine as 15 per month (or equivalent).
All abstracts were reviewed by one of two independent researchers. Initially, we selected a 10% sample of abstracts for review by both researchers; inter-rater agreement was assessed using the κ statistic, and the remaining abstracts were divided between the reviewers once a sufficient level of agreement was achieved (κ ≥ 0.7). If it was determined that an article might contain relevant primary data or secondary information (e.g. review article citing results from a population-based study), the full-text article was obtained and reviewed for inclusion and/or review of references. In order more easily to identify multiple publications from the same study, full-text articles were divided between two reviewers based on World Health Organization region. A third researcher independently reviewed all full-text studies (both accepted and rejected) to verify inclusion or exclusion. Discrepancies were resolved by discussion and consensus.
Data collection and analysis
Relevant data from accepted articles were abstracted for the following data categories: publication information (e.g. authors, year of publication), study methodology (e.g. sampling method used), study objective, study population, headache definition (e.g. diagnostic criterion, detailed definition), prevalence estimates, and incidence estimates. We calculated 95% confidence intervals using the prevalence estimate and sample size. All data and calculations were evaluated for completeness and accuracy by a second independent researcher. Regional variations were explored based on World Health Organization categorization.
Classification of chronic migraine definitions
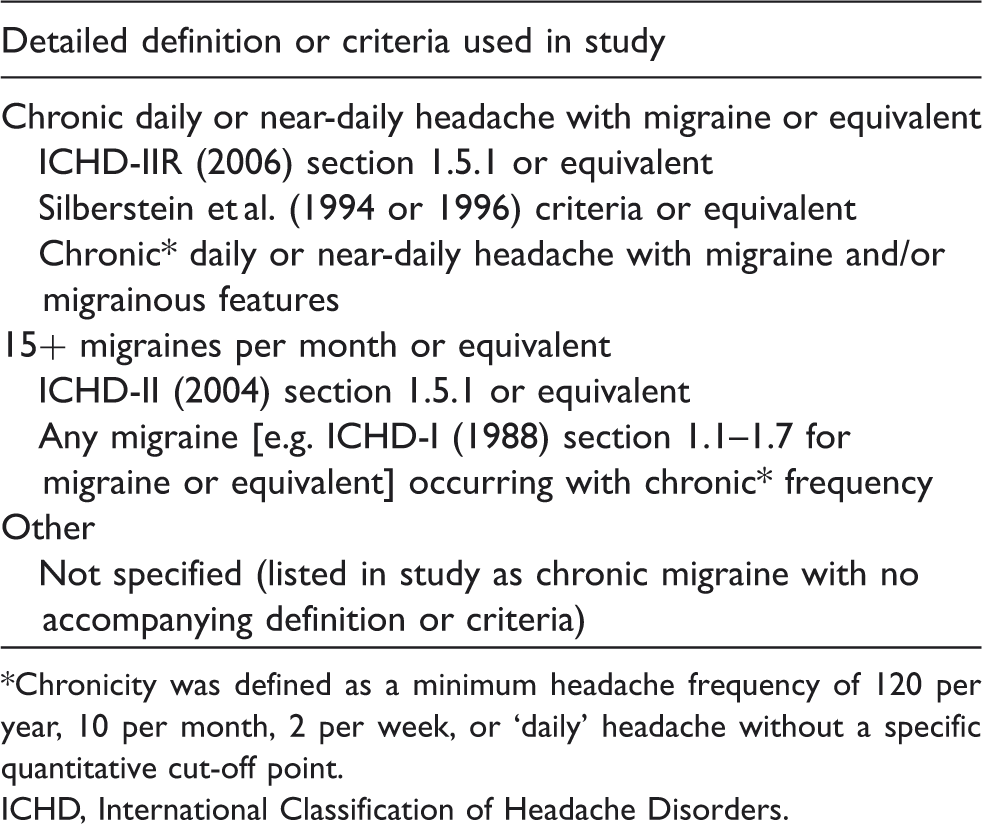
Chronicity was defined as a minimum headache frequency of 120 per year, 10 per month, 2 per week, or ‘daily’ headache without a specific quantitative cut-off point.
ICHD, International Classification of Headache Disorders.
Results
Search results and study characteristics
The initial search strategy elicited 859 unique reports. Of these, 97 abstracts were accepted and 25 additional articles were obtained based on review of relevant bibliographies. After review, 16 publications (15,19–33) representing 12 unique research studies were accepted for inclusion. A diagram of the article review process is presented in Figure 1.
Overall disposition of chronic migraine studies identified in PubMed, EMBASE, and Cochrane.
Characteristics of chronic migraine prevalence studies according to World Health Organization region

For studies with multiple relevant publications, the earliest available publication date is listed.
NR, not reported.
None of the studies presented data on the incidence of CM; only prevalence estimates were provided. One-year period prevalence was most commonly reported (n = 9, 75%); however, one study (8%) examined lifetime prevalence and two studies (17%) were not explicit as to the time frame used.
Prevalence of CM
The 12 studies included in this review provided 14 prevalence estimates for CM (the French GRIM2000 (15) study provided three estimates based on various definitions of migraine/migrainous disorder). The overall prevalence of CM ranged from 0 to 5.1% (Table 3, Figure 2).
Prevalence (%) of chronic migraine according to frequency of headache. Prevalence of chronic migraine according to frequency of headache (sorted by overall prevalence in descending order) These studies reported estimates but did not provide sufficient detail to be categorized in either of the above-mentioned groups. CDH, chronic daily headache; CI, confidence interval; ICHD, International Classification of Headache Disorders; NS, not specified.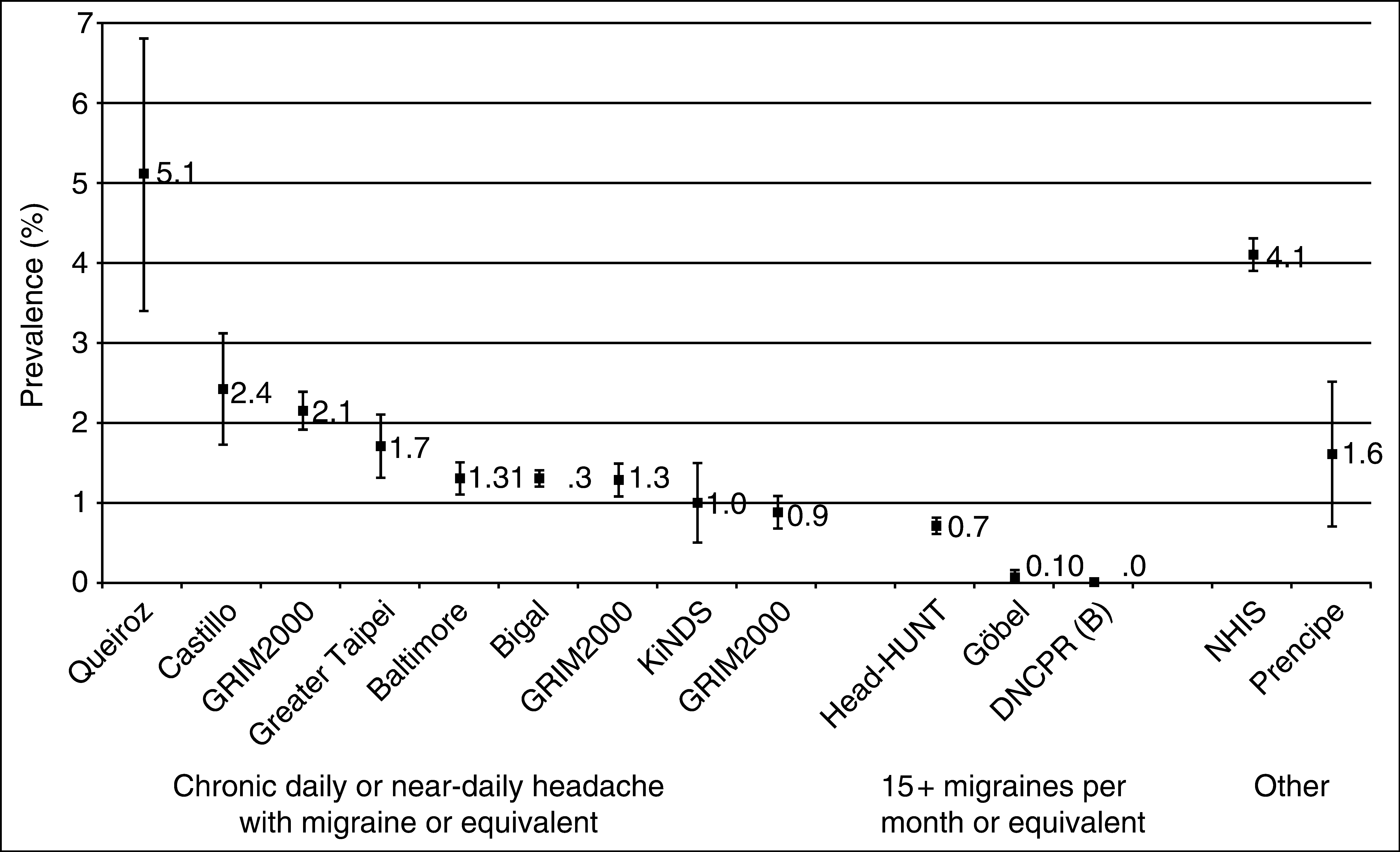

Classification variation
Several different criteria and definitions for CM were used across studies (Table 3). The studies identified in this review typically defined chronicity of headache or migraine as 15 per month (or equivalent). Seven of the studies used a definition of CM that was consistent with chronic daily or near-daily headache with features of migraine (e.g. S–L criteria for TM (5,11) or a definition in which at least half or 8+ of the headaches reported per month were migraine). The prevalence of CM in these seven studies (nine estimates) ranged from 0.86% to 5.1%. Three estimates defined CM as migraine that occurred on ≥ 15 days per month (or an equivalent yearly rate). Prevalence estimates using this more stringent criterion were relatively low and ranged from 0 to 0.7%. Two studies reported estimates, but did not provide sufficient detail to be categorized in either of the above-mentioned groups. An Italian study (29) reported the prevalence of TM as 1.6%, while a US study (24) reported the prevalence of CM as 4.1%.
Prevalence estimates for demographic subgroups were not commonly reported. Among three studies that reported gender-specific estimates, the prevalence of CM was 2.5–6.5 times higher in women (1.7–4.0%) than in men (0.6–0.7%). There were no notable trends in overall prevalence based on the proportion of women in each study. Although no studies reported age- or race-specific prevalence estimates, one study reported estimates stratified by both race and gender simultaneously (20).
Regional variations
Regional prevalence variations were apparent. Prevalence in the Americas ranged from 1.3% to 5.1% based on four estimates from four studies (19–21,24). Prevalence in three large US studies ranged from 1.3% to 4.1% (20,21,24), which was slightly lower than the prevalence reported in a small Brazilian study of 625 participants (5.1%) (19). Definitions of CM were similar among these studies. Three of the studies (19–21) defined CM as chronic daily or near-daily headache with migraine in the past year, whereas the remaining study (24) did not provide a detailed definition of disease.
Prevalence in the six European studies ranged from 0 to 2.4%, although these studies employed definitions of CM that differed from those of studies conducted in the Americas (15,25,28–31). Two of the studies defined CM as chronic daily or near-daily headache with migraine, with resulting estimates that ranged from 0.86% to 2.4% (15,31). One of the studies, the French GRIM2000 study, examined three different definitions of migraine and/or migrainous disorder and found that the prevalence ranged from 0.86% to 2.14% depending on the relative stringency of migraine definition used (15). An Italian study that did not explicitly define their criteria for CM reported a prevalence of 1.6% (29). Three European studies conducted in Denmark, Germany and Norway used criteria similar to the ICHD-II criteria that required ≥ 15 migraines per month (25,28,30). Prevalence estimates in these studies were lower than the other European studies and ranged from 0 to 0.7%.
Two Western Pacific studies, both conducted in Taiwan, provided two prevalence estimates (32,33), both of which used similar definitions of CM (i.e. chronic daily or near-daily headache with migraine in the past year). The Greater Taipei study reported the prevalence of CM as 1.7% among 3377 subjects aged ≥ 15 years (32). The prevalence was slightly lower (0.98%) among 1533 elderly adults who participated in the KINDS study (33).
Medication overuse among subjects with CM
Relative frequency of medication overuse among patients with chronic migraine (sorted by overall prevalence in descending order)

ICHD, International Classification of Headache Disorders; NS, not specified, TM, transformed migraine.
Results from the Norwegian Head-HUNT study demonstrate how variations in the duration of daily or near-daily analgesic use affect prevalence estimates (30). When using a cut-off of at least 6 months of daily or near-daily analgesic use, the prevalence of medication overuse among individuals with CM was 39.3%. When the duration of medication overuse was reduced from 6 months to either 3 months or 1 month, the prevalence of medication overuse among individuals with CM increased to 48.8% and 59.6%, respectively.
Two studies evaluated specific analgesics that were overused (29,31). Both studies found that individuals who had CM associated with medication overuse were taking ergotamine-containing compounds (57–67%) as opposed to analgesics that did not contain ergotamine (33–43%).
Discussion
Although two recent reviews of headache prevalence by Stovner and colleagues have examined chronic headache prevalence (1,17), this systematic review focuses on worldwide population-based prevalence estimates specifically for CM. The overall prevalence of CM ranged from 0.9% to 5.1% in the general population, with estimates typically in the range of 1.4–2.2%.
The European and global reviews by Stovner found that the prevalence of chronic headache defined as headache ≥ 15 days per month was 3–4% (1,17). The prevalence findings presented here suggest that CM represents approximately half of all chronic headache based on estimates provided by Stovner, and the results of this review are in the range reported by others (34).
We explored potential differences in the prevalence of CM across both gender and age, although none of the population-based studies in this review reported prevalence stratified by age groups, and only three studies reported gender-specific estimates. Among these three studies the prevalence of CM was 2.5–6.5 times higher in women than in men. Future studies should aim to report both gender- and age-specific prevalence estimates.
Regional prevalence variations also were apparent, although these differences might be attributable to alternative definitions of CM as opposed to true geographical variations in burden of disease. Regional variations should be interpreted with caution because of the small number of studies from the Americas, Europe, and the Western Pacific regions as well as the lack of studies from other regions such as Africa, the Eastern Mediterranean, and Southeast Asia.
The Americas had the highest prevalence of CM, with estimates up to 5.1%, but also had the largest variation across studies (1.3–5.1%) even though the definitions used in these studies were more homogeneous than in other regions. The European studies used relatively heterogeneous definitions of chronicity and provided some insight into how variations in definition influence prevalence estimates. The French GRIM2000 study examined three different definitions of migraine and/or migrainous disorder and found that the prevalence ranged from 0.86% to 2.14% depending on the relative stringency of migraine definition used (15); and three additional European studies used relatively strict criteria that required ≥ 15 migraines per month, similar to the ICHD-II, reporting very low prevalence estimates ranging from 0 to 0.7% (25,28,30). Although true differences in CM prevalence may exist across countries, it is also likely that diagnostic criteria may be interpreted or applied differentially.
Prevalence of medication overuse among subjects with CM also demonstrated wide variation and was evaluated only in European studies. Among adults with CM, prevalence of medication overuse was 31–69%. Even with the exclusion of the study by Prencipe and coworkers (29) that measured medication overuse but did not provide a specific definition of medication overuse, the prevalence still ranged from 31% to 51%.
Determining the frequency of MOH is further complicated by the fact that medication overuse in epidemiological studies is a surrogate for a diagnosis of MOH. Difficulty involves the conflicting perspectives on MOH within the ICHD guidelines and S–L criteria. The S–L criteria treat MOH as a subset of patients within the CM population, whereas the ICHD criteria specifically exclude MOH from the CM criteria and instead view MOH as a mutually exclusive headache category. As such, prevalence of CM based on ICHD criteria should theoretically exclude patients with MOH, whereas prevalence using S–L criteria would include MOH as a proportion of all patients. Most studies reporting CM prevalence did not specifically mention MOH or medication overuse. Thus, we cannot confirm whether MOH was truly excluded from estimates based on ICHD criteria.
Issues surrounding regional variation and the different definitions of MOH highlight the need for an easy-to-implement, operational definition of CM. Within the current literature, there are well-designed population-based studies of CM prevalence; however, results are hardly comparable. Without an operational definition to serve as the basis for accurate and reliable epidemiological data, we have an incomplete understanding of the prevalence of CM as well as the characteristics of the patient population. Even within the clinical setting, regional variations may result from alternative interpretations of diagnostic criteria.
Our review failed to identify any population-based estimates of CM incidence. To our knowledge, the only studies of incident CM are in headache clinic patients or other non-population-based cohorts (35), although three other population-based studies have examined the incidence of chronic headache, with varying results (36–38). In these studies, the definitions of chronic headache were similar (i.e. 15+ per month or equivalent), although the studies differed in how they established a headache-free baseline population as well as their respective time frame. A Norwegian study reported a 1-year incidence of 1.4% (headache >14 days/month among those with no analgesic use at baseline) (38), whereas a Dutch study reported a much higher incidence of 5.5% during a 3-month time frame (headache >14 days/month among those without chronic frequent headache at baseline) (37). Finally, a US study found that the incidence of CDH (180+ headaches per year among those with 2–104 headaches per year at baseline) was 2.9% after a mean of 11 months' follow-up (36).
The overall heterogeneity across studies is worthy of additional discussion. Although we considered a quantitative analysis of studies, we concluded that techniques such as meta-analysis were premature and inappropriate because of significant clinical and methodological heterogeneity across studies. We also considered quantitative analysis of important subgroups, such as those based on diagnostic criteria or gender, but concluded that the residual heterogeneity remained considerable. In summary, there are too few studies of similar populations and methods to justify statistical pooling.
Some limitations in our results should be acknowledged in the interpretation of findings. First, during the review of search results, abstracts were evaluated for possible mention of chronic headache or migraine prevalence. In some instances, articles on episodic headache may have contained CM prevalence data that were not included in the abstract and thus not selected for inclusion in this study. To reduce this limitation, the bibliographies of included studies and relevant review articles were reviewed to identify missing studies, and two publications on episodic headache/migraine that contained data on CM were found in this manner (26,28). Second, many estimates identified in this review were two-phase studies: typically, a screening questionnaire or interview followed by a physical examination. In the majority of cases, only subjects who screened positive were subsequently examined. This two-phase screening process is likely to reduce specificity (i.e. correctly ruling out chronic headache) but not sensitivity (i.e. correctly identifying true cases of chronic headache). These variations may result in an underestimate of the true prevalence of chronic headache, although the number of false negatives is likely to be very low for a condition such as headache. Third, it sometimes was not clear whether a given study took into account duration and persistence of headache or if secondary headache was excluded. Even if secondary headache were inappropriately included, this would not result in a vast overestimate of the true prevalence, since the proportion of subjects with secondary headache is very small (31). Fourth, all systematic reviews are limited by the dates of the search and review. Any population-based studies on chronic headache that have been published since mid 2007 therefore would not be included in this review. Lastly, a significant challenge of this review was reconciling frequency-based definitions of chronicity with the multiple chronic headache criteria that have evolved over the past 20 years. We used both frequency- and criteria-based definitions in developing our headache classification scheme, and some heterogeneity within each headache definition may exist.
This systematic review has identified population-based data on CM from around the world, although heterogeneity across studies and lack of data from certain regions leave an incomplete picture of the global prevalence of CM. Using the strict ICHD-II criteria, prevalence seems to be well under 1% of the adult population, at least in Northern Europe where this has been investigated. However, with a less restrictive definition, like the S–L criteria, or including patients with medication overuse, the prevalence is much higher, between 1 and 5%. For the neurologist, the prevalence of CM, even at the low end, is in the same range as epilepsy (39). Given the prevalence and burden of CM, the identification and treatment of patients with this debilitating condition should be recognized. Future epidemiological studies on CM and other chronic headache disorders would benefit from an ICHD consensus diagnosis that is both clinically appropriate and operational in large-scale epidemiological studies.
Footnotes
Competing interests
A.M. and C.C.T. are employees of Allergan, Inc. and therefore receive personal compensation (e.g. salary) from and have an equity/ownership (e.g. company stock) in the study sponsor. R.B.L. has received both grants and personal compensation from Allergan, Inc., each totalling in excess of $10 000. J.L.N., Q.B. and B.D. are employees of Cerner LifeSciences, which received research funding for this project. L.S. was obtained as an independent consultant without any compensation.
Acknowledgements
The authors thank Nirav Shah, MD, MPH, for his valuable feedback on this manuscript. The research presented in this paper was supported by Allergan, Inc. Employees for Allergan, Inc. were involved in the methodological design of the systematic literature review and helped write and edit drafts of this manuscript. They were not primarily involved in decisions regarding the included literature, management, analysis, or interpretation of the data. Primary decisions regarding the collection, management, analysis, and interpretation of the data were made by consultants.
Appendix A Search strategy for chronic migraine systematic review
SEARCH LIMITS
PubMed: 1990–17 July 2007
EMBASE: 1990–12 July 2007
Cochrane: 1990–12 July 12007
English language
SEARCH TERMS
Category
Terms
Field
PubMed results
EMBASE results
Cochrane results
Headache Class
‘chronic migraine’ OR ‘chronic headache’ OR ‘chronic daily headache’ OR ‘chronic tension-type headache’ OR ‘frequent headache’ OR ‘chronic frequent headache’ OR ‘transformed migraine’ OR ‘transformed headache’ OR ‘medication overuse headache’ OR ‘frequent daily headache’ OR ‘frequent migraine’ OR ‘analgesic overuse headache’ OR ‘rebound headache’ OR ‘misuse of headache medication’
All
1541
1484
656
Epidemiology
epidemiology OR burden OR prevalence OR incidence OR survival OR mortality OR morbidity
All
1 175 329
972 366
79 501