
Abstract
The aim was to assess costs and cost-effectiveness of additional acupuncture treatment in patients with headache compared with patients receiving routine care alone. A randomized, controlled trial was conducted, including patients (≥18 years old) with primary headache (more than 12 months, at least two headaches/month). Outcome parameters were quality of life (Short Form 36), direct and indirect costs differences during the 3-month study period and the incremental cost-effectiveness ratio (ICER) of acupuncture treatment. A total of 3182 patients (1613 acupuncture; 1569 controls) with headache were included (77.4% women, mean age and standard deviation 42.6 ± 12.3; 22.6% men, 47.2 ± 13.4). Over 3 months costs were higher in the acupuncture group compared with the control [€857.47; 95% confidence interval 790.86, 924.07, vs. €527.34 (459.81, 594.88), P < 0.001, mean difference: €330.12 (235.27, 424.98)]. This cost increase was primarily due to costs of acupuncture [€365.64 (362.19, 369.10)]. The ICER was €11 657 per QALY gained. According to international cost-effectiveness threshold values, acupuncture is a cost-effective treatment in patients with primary headache.
Background
Headache is a common disease. In Germany headache has been reported in 21% of men and 36% of women (1). The condition is associated with a high health economic burden, especially with regard to indirect costs, which are primarily due to time lost from work and leisure (2). The two most frequent forms of headache are migraine and tension-type headache (TTH). Population-based studies have suggested that 6–7% of men and 15–18% of women experience migraine headaches (3, 4). A survey from the USA has found a 1-year prevalence of 38% for episodic and 2% for chronic tension-type headache (5).
Migraine typically manifests as attacks of severe, pulsating, one-sided headache and is often accompanied by nausea, phonophobia or photophobia (6), whereas TTH is essentially defined as bilateral headache of pressing or tightening quality without a known medical cause (7). TTH is classified as episodic if occurring on <15 days per month and as chronic if occurring more often (6). Although in most cases it is sufficient to treat acute headaches, a significant minority of patients with migraine need interval treatment as attacks occur too often or are insufficiently controlled. Drug treatment with β-blockers, calcium antagonists or other substances has been shown to reduce the frequency of migraine attacks; however, the success of treatment is usually modest and tolerability often suboptimal (8). Acupuncture is widely used for the treatment of TTH, but its effectiveness is controversial (9).
In Germany, acupuncture is administered primarily by physicians. The treatment is relatively resource-intensive due to the time involved for physicians and patients alike (10). The present study assessed the quality of life (QoL), costs and the cost–effectiveness relationship of routine care plus acupuncture compared with routine care alone in patients with primary headache, because there has been a lack of information on this research question. This investigation was part of the Acupuncture in Routine Care (ARC) studies (11).
Methods
Study design
In this multicentre, randomized controlled trial, patients (≥18 years old) diagnosed clinically with primary headache (>12 months) and at least two headaches per month were enrolled after they contacted a participating physician. Secondary headaches caused by somatic diseases (e.g. hypertension, meningioma or meningoencephalitis) were criteria for exclusion. Physicians classified patients according to the criteria of the International Headache Society to differentiate between patients with migraine (episodic or chronic) and those with TTH (frequent episodic or chronic) (6). Other forms of primary headache which did not meet the criteria for migraine or TTH were not classified, and patients with migraine were not differentiated into migraine with or without aura.
The patients were allocated either to an acupuncture group that received immediate acupuncture treatment or to a control group that received delayed acupuncture treatment (i.e. after 3 months). Both groups were free to use conventional routine medical care as offered by the German social health insurance funds. At baseline the number of days with headache was assessed for the months before randomization.
We used central telephone randomization with blocks of 10 patients, and the random list was generated with SAS software (SAS Institute, Inc., Cary, NC, USA).
Participating physicians were required to have received at least 140 h of acupuncture education (A-diploma). The majority of participating physicians were general practitioners. In Germany, as elsewhere, such training includes wide variations in acupuncture style. The acupuncture treatments provided in the study consisted of 10–15 acupuncture sessions. Further information on study design has been published elsewhere (11).
The primary outcome measure was the incremental cost-effectiveness ratio (ICER). Secondary outcomes in this evaluation included the QoL, costs and cost differences between the 3 months prior to and the 3 months following study initiation.
Quality of life
QoL was assessed with the Short Form (SF)-36 (12) questionnaire using the subscales and the components scales. The SF-36 also served as the basic benefit estimator for the cost-effectiveness analyses. At baseline and at 3 months the patients completed questionnaires which assessed the quality of life over the last 7 days.
Costs
The costs considered in the present analysis were measured in societal perspective and included the direct healthcare-related costs of acupuncture (cost of each acupuncture session was €35), physician visits and hospital stays (without consideration of private billings), and any drugs prescribed (including patient co-payments). In addition to health insurance costs, the indirect costs caused by lost workdays were also taken into account. These were determined by using the human capital approach (13) and were estimated to be approximately €78 per lost workday. We measured resource use based on data maintained by the social health insurance funds. The baseline period for costs was 3 months before randomization.
In the present study, we have calculated (i) the overall costs during the 3-month treatment period following randomization, including costs unrelated to headache; and (ii) diagnosis-specific costs. Therefore we used the International Classification of Diseases (ICD)-10 codes to identify costs due only to headache and related conditions. These codes were also provided by the insurance companies for all resources such as days of lost work. The headache-related ICD codes were predefined in an independent setting by two medical researchers. Disagreements were resolved by discussion until consensus was reached.
Cost-effectiveness analyses
In the case of higher costs and better medical outcome (improved QoL in acupuncture group), we performed additional cost-effectiveness analyses. The SF-36 QoL data were converted to SF-6D using the algorithm developed by Brazier et al. (14). Only patients with sufficient SF-36 data were included in the cost-effectiveness analysis. Quality-adjusted life years were calculated by adopting the area under the curve method (15, 16) using the following formula:
The analysis is based on the utility values at each time point (α= baseline utility, β= utility after 3 months) and uses the common assumption of a linear change over time (15). After the intervention period of 3 months, we assumed a linear decrease of acupuncture effects returning to baseline level 12 months after study onset. The differences in costs and effects between the two groups were compared and the ICER was calculated using the following relation (17):

The ICER shows the additional costs for one extra quality-adjusted life year (QALY) gained compared with control treatment. We measured the ICER against a societal threshold value λ, which is often described as society's willingness to pay for one QALY gained. In the UK, a threshold of £30 000 to QALY has been found to be consistent with decisions for adopting new technologies by the National Institute for Clinical Excellence (18). In Germany, such a threshold does not yet exist. As a result, we used an arbitrary and hypothetical threshold of max. €50 000 per QALY. If the ICER is below such a threshold value, the treatment can be regarded as cost-effective. In addition, cost-effectiveness acceptability curves were created by applying the net benefit approach (19, 20):

For a given value of λ, an intervention can be considered cost-effective if its net benefit is greater than zero (i.e. the ICER is below λ). The costs and effectiveness results were bootstrapped and transformed into net benefit values under varying threshold values. Subsequently, the results were plotted in a cost-effectiveness acceptability curve. Under a Bayesian framework, the cost-effectiveness acceptability curve shows the probability that the incremental cost-effectiveness will be below λ for a whole range of values of λ (19).
The cost-effectiveness analyses were performed for selected patient subgroups, such as gender and the form of headache (i.e. migraine or TTH).
Sensitivity analyses
In additional sensitivity analyses, we considered a variety of acupuncture cost scenarios (between €15 and €55 per acupuncture session) and different durations of therapeutic and economic effects (1–5 years). As part of our calculations, we assumed that the differences in QoL outcome observed between the two treatments groups would gradually decrease over time. The different durations applied in these different scenarios ranged from 1 to 5 years. For sensitivity analyses, the study situation was always defined as base case. In an economic model calculation, we took into account the possibility that a variation in one specific parameter could result in modified therapeutic effect differences between the groups. This is why variations in physician's payment alone were taken into account, as well as the possibility that a decreased (or increased) physician's fee might result in reduced (or improved) clinical effectiveness. In acupuncture treatment, the impact of non-specific factors on treatment results has been widely discussed (21). For example, lower fees for acupuncture sessions may reduce the intensity of the physician–patient relationship, patient expectations, or treatment satisfaction. Furthermore, there is some evidence that different payment systems have different impacts on clinical outcomes (22, 23). Therefore, we assumed that a reduction in the cost of an acupuncture session from €35 (base case) to €15 would be associated with a 50% reduction in QALY differences, whereas an increase in cost to €55 would result in a 50% increase in QALY differences.
For the base case scenario, there was no need to discount any costs or effects, because the observation period was <1 year. In the sensitivity analyses, we discounted the measured future QALY effects at 1.5% and costs at 3% per year. The discount rates are compatible with those published previously (24, 25).
Statistical analyses
Student's t-test was used for comparisons on sociodemographic baseline characteristics and QoL data. Furthermore, an
To derive cost-effectiveness acceptability curves, non-parametric bootstrapping was used. The original sample was bootstrapped 1000 times to obtain 1000 means for cost and effect differences and the resulting ICERs. These bootstrap results were used to build the cost-effectiveness acceptability curves as described above.
For inferential statistics, SPSS© version 11.0 was used (SPSS Inc., Chicago, IL, USA). Finally, we used MS EXCEL© 2003 to model cost-effectiveness analyses for patient subgroups and to perform the additional sensitivity analyses. Significance was set at P < 0.05.
Results
Baseline characteristics
A total of 3182 patients (1613 acupuncture; 1569 controls) with headache were enrolled (77.4% women, mean age 42.6 ± 12.3 years; 22.6% men, mean age 47.2 ± 13.4 years). Migraine was diagnosed in 54.4% of patients (3.8% with chronic migraine) and TTH in 39.9% (7.1% with chronic TTH); 5.7% of patients had primary headache but did not meet definite criteria for migraine or TTH. At baseline there were no significant differences in sociodemographic variables and costs between the two treatment groups, with the exception of prior disease duration (Table 1), which was significant longer (P = 0.028) in control patients (mean difference of 0.8 ± 0.4 years).
Baseline characteristics of study population

Student's t-test.
The acupuncture treatment for the enrolled patients was performed by 1560 participating physicians (1429 for patients included in cost-effectiveness analyses) in Germany. Participating patients received a mean number of 10.5 [95% confidence interval (CI) 10.3, 10.6] acupuncture sessions over the 3-month treatment period. Sociodemographic and economic data were available for all patients, so all were included in the cost analysis. The QoL analysis and the analyses of cost-effectiveness are based on a reduced number of patients caused by missing data on the QoL questionnaire.
Costs analysis
Table 2 shows the mean costs during the treatment period as well as the cost differences between baseline (i.e. the 3-month period prior to study initiation) and the 3-month treatment period. The mean overall costs incurred by acupuncture patients during the treatment period were €857.47 (95% CI 790.86, 924.07) [diagnosis specific: €410.23 (95% CI 399.75, 420.71)] and €527.34 (95% CI 459.81, 594.88) [diagnosis specific: €46.49 (95% CI 35.87, 57.11)] in control patients (P < 0.001). Three months after randomization, the mean cost difference between the two treatment groups [total overall: €330.12 (95% CI 235.27, 424.98), diagnosis specific: €363.74 (95% CI 348.82, 378.66)} was primarily due to the acupuncture costs in the acupuncture group [€365.64 (95% CI 362.19, 369.10)].
Mean costs and cost differences (costs during the 3-month treatment period–costs during the 3 months prior to study initiation) in EURO per patient for acupuncture and control group

Negative values indicate decreased costs during the 3-month treatment period compared with the 3 months prior to study initiation.
In acupuncture patients, the overall cost difference between baseline and the end of the 3-month treatment period was €362.05 (95% CI 293.78, 430.32) compared with €7.05 (95% CI −62.17, 76.27) in control patients (P < 0.001). The diagnosis-specific difference was €374.17 (95% CI 364.54, 383.80) in acupuncture patients compared with €5.73 (95% CI −4.03, 15.49) in control patients (P < 0.001). Excluding the costs of acupuncture reveals that there were no significant overall cost differences between the two study groups. Also in single cost components no significant differences between the two study groups could be detected.
Quality of life
QoL data for calculation of SF-36 component scores were available for 2569 patients at baseline and for 2600 patients after the 3 months study duration. Table 3 shows the results of the QoL assessment determined from the particular SF-36 dimensions and component scores. At baseline we found no significant differences in patients' QoL. Three months after randomization, highly significant differences were assessed in all SF-36 dimensions and component scores in favour of acupuncture-treated patients.
SF-36 at baseline and 3 months after randomization

Student's t-test.
All scales range from 0 to 100, higher values indicate improved quality of life.
Cost-effectiveness analysis
QALYs could be generated for 2682 patients (84.3% of all included patients; 1356 acupuncture; 1326 controls). For these patients sufficient QoL data for baseline and the 3-month follow-up were available and it was possible to perform additional cost-effectiveness analyses. As a result, we observed a gain of 0.0301 ± 0.004 QALYs in the acupuncture group compared with the control group (Table 4). However, this gain was associated with additional costs [overall: €350.85 (95% CI 216.63, 485.07), diagnosis-specific: €365.38 (95% CI 341.74, 389.02)]. The ICER was €11 657 (overall) and €12 140 (diagnosis-specific) per QALY gained. Therefore, for the assumed threshold value of €50 000, the additional acupuncture intervention would appear to be cost-effective.
We performed sensitivity analyses (Table 5) comparing subgroups according to gender and type of headache and effect duration. For migraine it was found that acupuncture treatment in men seems to be more cost-effective than in women (ICER men €−810 vs. women €19 228). This finding was also confirmed after adjusting for age and gender (ICER men €1567 vs. women €6183). In contrast, a reverse situation was observed for TTH. Therefore, the acupuncture treatment was assessed as a more cost-effective treatment for women (ICER men €34 775 vs. women €4109; adjusted ICER men €12 599 vs. women €2619).
Cost-effectiveness analyses: mean QALY differences, mean cost differences in overall and diagnosis-specific view and the resulting ICERs in acupuncture patients vs. control patients after 3 months study duration

Estimated values based on
Sample size: Migraine n = 1485 (male = 278; female = 1207); tension-type headache n = 1050 (male = 306; female = 744); all patients n = 2682 (male = 612; female = 2070).
QALY, Quality-adjusted life year; ICER, incremental cost-effectiveness ratio.
ICERs in sensitivity analyses—isolated variation of physicians' acupuncture payment rate, length of acupuncture effect and combined variation of acupuncture payment rate and dimension of group effect difference
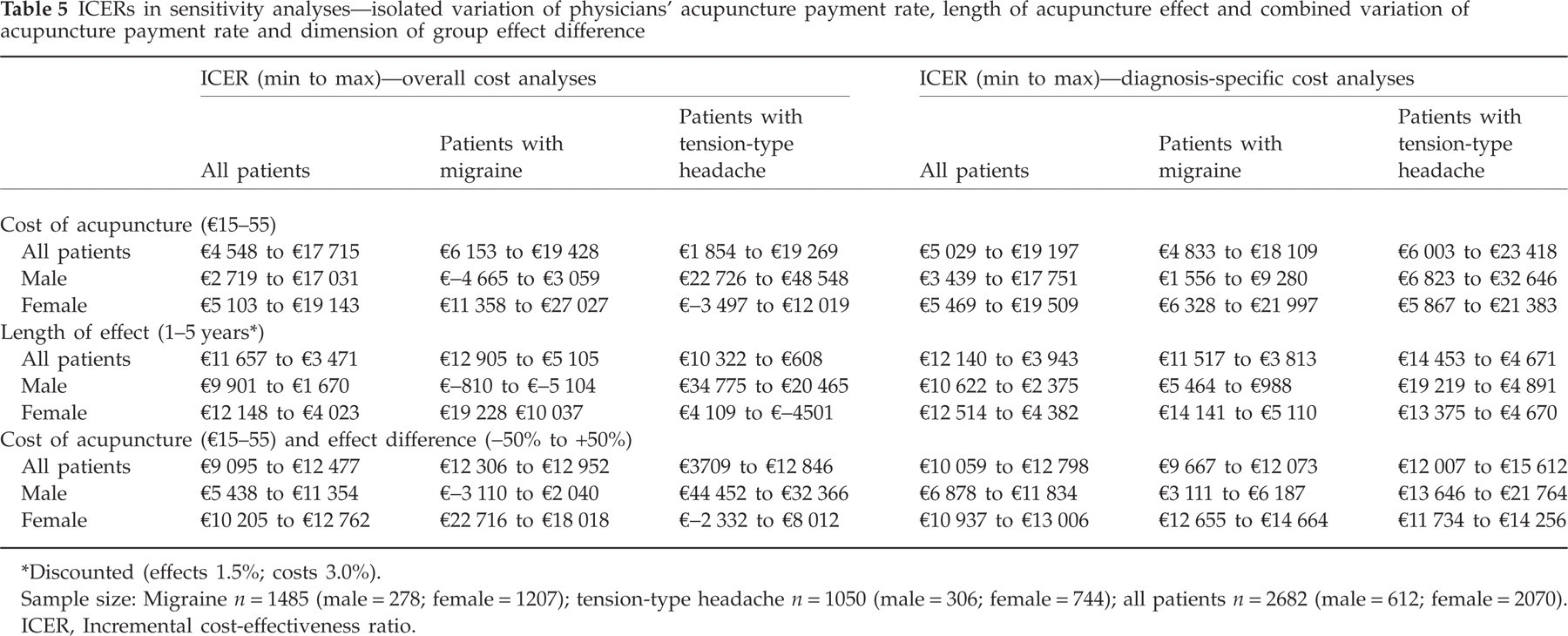
Discounted (effects 1.5%; costs 3.0%).
Sample size: Migraine n = 1485 (male = 278; female = 1207); tension-type headache n = 1050 (male = 306; female = 744); all patients n = 2682 (male = 612; female = 2070).
ICER, Incremental cost-effectiveness ratio.
The cost acceptability curves represent the probability of cost-effectiveness against different threshold values ranging from €0 to €50 000. In female patients, acupuncture treatment reaches a maximum overall cost-effectiveness probability of approximately 100% vs. a probability of approximately nearly 100% (98.8%) in men (Fig. 1).

Probability that acupuncture treatment in patients suffering from headache is cost-effective against different threshold values of society's willingness to pay.
Sensitivity analysis
Table 5 presents results of the sensitivity analyses in detail. Changing the parameter ‘physician payment rate’, of itself (i.e. without regard to any effect this might have on treatment effects), led to major changes in the cost-effectiveness of acupuncture. Similar, changing the parameter ‘effect duration’, of itself, had a marked influence on the cost-effectiveness of acupuncture treatment. Subsequently, we investigated whether a decrease in the effectiveness of acupuncture treatment due to a reduction in the physician payment rate (or, conversely, an improvement in the effectiveness of acupuncture treatment due to an increase in the payment rate) might affect the cost-effectiveness of acupuncture treatment. However, the calculations showed that neither scenario would lead to major changes in the cost-effectiveness of acupuncture treatment, confirming the robustness of our findings.
Discussion
Compared with routine care alone, in patients with headache acupuncture in addition to routine care was associated with a better QoL, but also with higher costs. This increase in costs was primarily due to the costs of acupuncture treatment itself and was not compensated for by savings in other areas during the study period. The ICER for all patients was between €11 657 (overall) per QALY gained and €12 140 (diagnosis-specific) per QALY gained. If we adopt a threshold of €50 000 per QALY gained, acupuncture in addition to routine care would thus appear to be cost-effective.
To our knowledge, this is the first German analysis to have evaluated the cost-effectiveness of acupuncture treatment in patients suffering from headache. The large sample size allows for a robust estimation of costs.
Although a cost-effectiveness analysis based on costs per headache day would have been more disease specific, it was decided to perform a cost–utility analysis based on QoL data. The advantage of cost–utility analyses is that QoL includes treatment benefits and side-effects. The source of costs in the present study consisted of data from the social health insurance funds. Thus, private expenses, such as over-the-counter medication or non-prescribed physical therapy, could not be included in the analysis. Nevertheless, by using the social health insurance funds databases, we were able to take into account all patient contacts with the German healthcare system apart from purely out-of-pocket expenses. In this context, it is important to note that approximately 88% of the German population is insured by a social health insurance fund (26). All included patients were insurants in one of the participating social health insurance funds. These patients could choose their physicians freely and the costs of their visits are usually covered. However, at the time of the study, the statutory health insurance companies did not reimburse acupuncture treatment. Only if they paid for it out of pocket might it have been possible for patients of the control group also to receive acupuncture outside the study context. Nevertheless, we feel their incentive to do so was limited because of the control group's waiting-list design. All patients in the control group knew that they could receive acupuncture at no cost simply by waiting for 3 months. The aim of the present study was not to assess the efficacy of acupuncture treatment. Because the study was performed as a pragmatic trial in a real-life setting, we were not able to control for all possible confounders; furthermore, we had no sham control. However, these factors do not change the major findings of our study.
Although it is conceivable that our results do not reflect real-life cost-effectiveness, the algorithm developed by Brazier tends to generate ICERs that are somewhat higher than those generated with other methods (27). Thus, our analysis is based on a conservative appraisal method.
Another limitation arises from the short duration of the study. Cost and effectiveness data were available for a period of only 3 months after baseline, because after 3 months patients in the waiting list control group were also offered acupuncture treatment. Therefore, we were unable to investigate possible long-term health economic effects in the present study. However, the current QALY calculation was a conservative approach, because it assumes a linear decrease in acupuncture effects between 3 and 12 months after study onset. Actually, clinical follow-up of the present study indicates that acupuncture effects were maintained over at least 6 months for both TTH and migraine (28–30). Furthermore, the results of a similar study have demonstrated that acupuncture benefits were maintained even after 1 year (24). The cost-effectiveness of acupuncture clearly depends on the length of effects, since maintaining short-term effects (or in case of a steep decline in effects) would require repeat acupuncture sessions at increased overall costs, resulting in a decreased cost-effectiveness ratio. We also performed additional sensitivity analyses according to a variety of assumptions, including modelling effect durations and projecting acupuncture session costs ranging from €15 to €55. We considered the possibility that a reduction in a physician's payment could potentially result in inferior treatment effects, leading to a less favourable ICER and a decreased likelihood of cost-effectiveness. Up to now, acupuncture has not been reimbursed by the German social health insurance funds on a routine basis. Therefore, the used payment rate for an acupuncture session was determined arbitrarily. This was necessary because in the German healthcare system the fees for services reimbursed by social health insurance funds are fixed administratively and are not necessarily related to the actual costs incurred by the physicians performing the service. The fee used in our base case scenario (i.e. €35 per acupuncture session as paid during the project) is meant to include the costs of needles and other consumables. Acupuncture treatment is now included in a nationwide list of reimbursable healthcare services. The fee for this treatment for low back pain and osteoarthritis of the knee is a result of negotiations between the general practitioners' organizations and the social health insurance funds in the German Federal Committee of Physicians and Health Insurers. As a result, the recently concerted fee per acupuncture session is between €15 and €25 (31).
The present study represents the first calculation of ICERs for acupuncture treatment in patients with headache in Germany. A cost-effectiveness analysis of acupuncture in primary care patients with headache in the UK has also yielded ICERs comparable to those reported in our study (24). A recent study, which was also part of the ARC studies (11), has investigated an ICER of €12 469 per QALY gained for acupuncture in patients with chronic neck pain (32). There is a lack of studies focusing the incremental cost-effectiveness of other treatment options compared with usual care in patients with headache. However, in light of these figures, acupuncture appears to be a cost-effective treatment in patients with headache.
Conclusion
This study has shown that using acupuncture in addition to routine care to treat patients with primary headache results in a marked and clinically relevant benefit and is cost-effective.
Footnotes
Competing interests
None to declare.
Acknowledgements
We thank Katja Wruck and Dagmar Selim for data management, Iris Bartsch and Beatrice Eden for data acquisition, the members of the advisory board (Dr Bodo Liecker, Dr Konrad Beyer, Dr Josef Hummelsberger, Hardy Müller, Dr Albrecht Molsberger, Dr Helmut Rüdinger, Dr Wolfram Stör, Dr Gabriel Stux) for helpful advice and Niels Balthasar and Jürgen Schwabe for health economic data management. In addition, we would like to express our gratitude to all participating patients and physicians. The trial was initiated at the request of the German health authorities (Federal Committee of Physicians and Social Health Insurance Companies, German Federal Social Insurance Authority) and sponsored by the Techniker Krankenkasse, a German statutory sickness fund. All decisions on design, data collection, analysis, interpretation, and publication were left completely to the discretion of the researchers.