
Abstract
We aimed to investigate the effectiveness of acupuncture in addition to routine care in patients with primary headache (> 12 months, two or more headaches/month) compared with treatment with routine care alone and whether the effects of acupuncture differ in randomized and non-randomized patients. In a randomized controlled trial plus non-randomized cohort, patients with headache were allocated to receive up to 15 acupuncture sessions over 3 months or to a control group receiving no acupuncture during the first 3 months. Patients who did not consent to randomization received acupuncture treatment immediately. All subjects were allowed usual medical care in addition to study treatment. Number of days with headache, intensity of pain and health-related quality of life (SF-36) were assessed at baseline, and after 3 and 6 months using standardized questionnaires. Of 15 056 headache patients (mean age 44.1 ± 12.8 years, 77% female), 1613 were randomized to acupuncture and 1569 to control, and 11 874 included in the non-randomized acupuncture group. At 3 months, the number of days with headache decreased from 8.4 ± 7.2 (estimated mean ± S.E.) to 4.7 ± 5.6 in the acupuncture group and from 8.1 ± 6.8 to 7.5 ± 6.3 in the control group (P < 0.001). Similarly, intensity of pain and quality of life improvements were more pronounced in the acupuncture vs. control group (P < 0.001). Treatment success was maintained through 6 months. The outcome changes in non-randomized patients were similar to those in randomized patients. Acupuncture plus routine care in patients with headache was associated with marked clinical improvements compared with routine care alone.
Introduction
In Western societies, headache is one of the most common symptoms. In a nationwide survey, 21% of men and 36% of women reported headache in the week before (1). This is consistent with international data (2). The social and economic impact of the high prevalence of headache is enormous (3, 4). Patients with chronic headache undergo great restrictions in their quality of life (5), even between the attacks (6). Because of the unclear aetiology, a causal therapy is missing. Guidelines recommend treatment with several drugs (including antidepressants or medication originally developed for the treatment of epilepsy) for patients with chronic headache (7–9). On the basis of the risk of a drug-elicited headache, patients often request therapies without drugs. One of the most applied therapies without drugs in patients with headache is acupuncture. Studies comparing the effectiveness of acupuncture vs. drug therapy seem to support the equivalence between acupuncture and fluranizine (10).
A systematic review of acupuncture in patients with headache yielded ambiguous results (11): in half of the 16 trials comparing verum and sham (placebo) acupuncture in migraine and tension-type headache patients, verum acupuncture was reported to be significantly superior. Most of the studies were assessed to have methodological and/or reporting shortcomings, and it was concluded that well-planned, large-scale studies are needed to assess the effectiveness and cost-effectiveness of acupuncture under real-life conditions (12).
In 2000 the German Federal Committee of Physicians and Health Insurers proposed that large research initiatives on acupuncture could be conducted by health insurance companies for several pain syndromes (13).
As one part of these research initiatives we designed the present study as a pragmatic trial to investigate the effectiveness of acupuncture in addition to routine care compared with routine care alone in patients with primary headache. In addition, we examined whether the effects of acupuncture differ in randomized and non-randomized patients, whether treatment effects last over a longer period of time, and whether patient and physician characteristics are associated with particular treatment outcomes.
Materials and methods
Design
The present Acupuncture in Routine Care (ARC) study included a multicentre randomized controlled trial plus a non-randomized cohort. Patients who agreed to randomization were allocated to an acupuncture group that received immediate acupuncture treatment or to a control group that received delayed acupuncture treatment 3 months later. Patients who declined to be randomized were included in a third arm and also received immediate acupuncture treatment (non-randomized acupuncture group). The study period per patient was 6 months and was comprised of a 3-month treatment phase followed by 3 months of follow-up.
The ARC study is part of a large acupuncture research initiative funded by a group of statutory health insurance companies that provide coverage to approximately 10% of the German population. The study protocol was approved by the local ethics review boards, and the study itself was conducted according to standard guidelines [i.e. Declaration of Helsinki and Good Epidemiological Practice (European Epidemiology Federation)]. All study participants provided written, informed consent.
Patients
Patients insured by one of the participating statutory health insurance companies were recruited after they had contacted a participating physician due to primary headache. If patients requested acupuncture, or if the physician considered acupuncture to be a suitable treatment option, they were informed about the study. In addition, they received patient information including the relevant facts about study design, study procedure and acupuncture treatment. Subjects who met the inclusion criteria, provided informed consent and signed an agreement for randomization were randomized using a central telephone randomization procedure. For randomization we used blocks of 10, and the random list was generated with SAS (SAS Inc., Cary, NC, USA). Patients who declined randomization were included in the non-randomized acupuncture group. Patients were only included in the study if both the physician baseline questionnaire and the patient consent form following randomization were received. Upon successful inclusion, patients were sent the baseline questionnaire by standard mail.
To be included, patients had to meet the following criteria: clinical diagnosis of primary headache (> 12 months) and at least two headaches per month; age ≥ 18 years; written informed consent. Physicians classified patients according to the criteria of the International Headache Society to differentiate between patients with migraine (episodic or chronic) and those with tension-type headache (frequent episodic or chronic) (13). Other forms of primary headache which did not meet criteria for migraine or tension-type headache were not classified, and patients with migraine were not differentiated into migraine with or without aura. The exclusion criteria for patients were headache caused by somatic diseases such as hypertension, meningioma or meningoencephalitis.
At baseline the number of days with headache was assessed for the months before randomization.
Interventions
Physicians interested in participating in the study were required to have at least an A-diploma, which represents 140 h of certified acupuncture training. This and other training include wide variations in style and acupuncture technique.
Each patient in the randomized and non-randomized acupuncture group received up to 15 acupuncture sessions during the first 3 months and no acupuncture between 3 and 6 months. The aim was to assess the effectiveness of acupuncture in usual care. Because of this, each patient could be treated individually and the number of needles and the acupuncture points used were chosen at the physicians’ discretion. Only needle acupuncture (with disposable one-time needles) was allowed, whereas other forms of acupuncture treatment (e.g. laser acupuncture, electro-acupuncture, moxibustion) were not permitted. Furthermore, only manual needle stimulation was allowed. The control group was not allowed to use any kind of acupuncture during the first 3 months. In all three treatment groups, patients were allowed to use any additional conventional treatments as needed.
In accordance with German federal regulations, the participating health insurance companies covered 100% of the acupuncture costs for patients who agreed to randomization and 90% of costs for patients who participated in the study but did not agree to randomization.
Outcome measurements
The patients completed standardized questionnaires (including sociodemographic characteristics) at baseline and after 3 and 6 months. The primary outcome measure was the number of days with headache per month. Because the improvements observed in all three groups were essentially proportional to the headache at study entry, we also calculated the 3-month percent reduction of headache days for each patient (with negative values indicating an additional headache day loss despite therapy; in each case, the maximum possible improvement/deterioration was scaled to 100%). If headache days increased for an individual patient during follow-up, the percentage was calculated with respect to the maximum possible loss and given a negative sign. Treatment responders were also calculated: a patient with a reduction of ≥ 50% was considered to be a treatment responder.
Further secondary outcome parameters included the Short Form (SF)-36 physical and mental component scales and its subscores assessed over the last 7 days. Data on cointerventions (e.g. analgesics) as prescribed medication were provided by the health insurance companies. Furthermore, patients where asked about the use of other treatments (including other complementary interventions) in each questionnaire. Side-effects were evaluated using patient and physician questionnaires after 3 months. In order to study the maintenance of therapeutic success in the acupuncture groups and the effect of delayed acupuncture treatment in the control group, changes from baseline to 6 months were calculated analogously.
Statistics
Confirmatory testing of the primary and secondary outcomes (using SPSS 11.5; SPSS Inc., Chicago, IL, USA) was based on the intention-to-treat population using the maximal available dataset. Sensitivity analyses were performed for the primary outcome either by replacing missing data according to the last value carried forward principle or using various hot deck methods or regression-based multiple imputation. The test procedure was performed in order to maintain a global significance level of α= 5%. Using covariance analysis, we tested the two-sided null hypothesis H0.1: mean number of days with headache after 3 months’ acupuncture = mean number of days with headache after 3 months control between the randomized groups, separately for each diagnosis (migraine or tension-type headache). With 527 patients per group, the study would have had 90% power to detect a difference of 1 day in days with headache assuming a mean of 10 days with headache and a
In order to identify factors affecting improvements in headache, and for a better understanding of patient selection due to the acceptance of randomization, common linear mixed models for the patients with migraine and tension-type headache with outcome variables as responses, physicians as random effect and baseline variables as fixed effect regressors were fitted to the data of the three groups using a backward selection procedure. Mixed models were chosen to comply with the potential cluster structure of the data, because several patients were included by the same physician. As potential regressors, we prespecified several characteristics of the physicians (age, years of professional experience, type of acupuncture diploma, hours of acupuncture training, years of acupuncture experience, diagnosis in the context of traditional Chinese medicine, and percent of practice time with acupuncture treatment) and of the patients (sex, age, education, baseline values of the outcome variables, baseline physical and mental quality of life scores, the duration of complaints prior to the study, and the study group to which each patient was assigned) before the study started. For each variable, an interaction term with diagnosis was included to study potential differences between migraine and tension-type headache. For the final model, significant variables were selected in a stepwise backwards procedure based on likelihood ratio tests. In addition, we considered the selected regressors as potential modifiers of the acupuncture effect and added the corresponding interaction terms to the model, backwards selecting if they were significant. All reported P-values are two-sided.
Results
Patient inclusion, baseline characteristics, and treatment
Between January 2001 and 2003 a total of 15 278 patients with headache were recruited for the study by 4686 study physicians (see Fig. 1 for patient selection). A total of 3404 patients accepted randomization and were allocated to the acupuncture or the control group. Two hundred and twenty-two patients (98 acupuncture, 124 control) could not be included in the analysis because the study office did not receive the consent form or the patients did not receive the study intervention. The remaining 15 056 patients (1613 acupuncture, 1569 control, 11 874 non-randomized acupuncture) were included in the intention-to-treat analysis. After 3 months, data were available for 85% of the patients (acupuncture 1447, control 1424, non-randomized acupuncture 9947).

Flow chart.
Migraine was diagnosed in 47.8% of patients (5.3% chronic migraine) and tension-type headache in 46.3% (12.0% chronic tension-type headache); 5.9% had primary headache but did not meet definite criteria for migraine or tension-type headache.
The randomized groups were comparable with regard to baseline characteristics (except for the duration of disease and the mental component score from the SF-36; see Table 1). Between the randomized and non-randomized acupuncture groups, however, there were significant differences. Patients who did not consent to randomization were on average half a year older compared with randomized patients. Non-randomized patients were also more likely to have experienced more intensity of pain and had, on average, suffered from headache one and a half year less than randomized patients. Quality of life was less reduced in randomized patients in all SF-36 subscales, with the exception of general health perception and vitality and both component scores. Patients in the acupuncture groups received 10.3 ± 2.6 acupuncture sessions (randomized acupuncture 10.3 ± 2.6; non-randomized acupuncture 10.2 ± 3.7; P = 0.411). Most patients (76.4%) received 5–10 acupuncture sessions, whereas 18.8% received > 10 sessions and 4.8% fewer than five sessions.
Baseline characteristics of study population
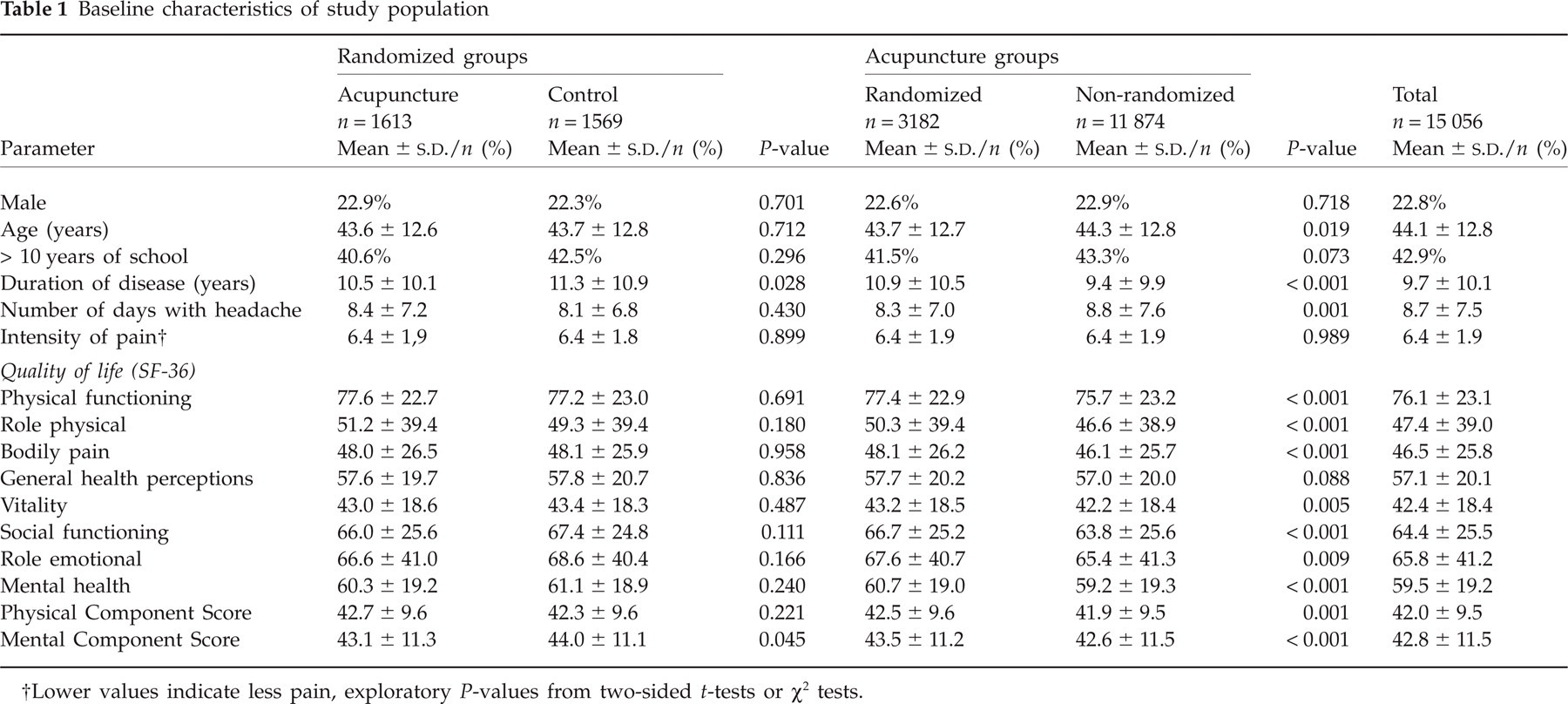
Lower values indicate less pain, exploratory P-values from two-sided t-tests or χ2 tests.
Randomized comparisons
The development of the number of days with headache in both randomized groups and the non-randomized group is depicted in Fig. 2. In the primary analysis at 3 months, reduction of headache days was more pronounced in the acupuncture than in the control group {by 2.86 [

Development of the number of days with headache per month.
In intensity of pain and quality of life (on all SF-36 subscales and both component scores), the 3-month improvement was significantly more pronounced in the acupuncture than in the control group (see Table 2a). In all but two parameters (number of days with headache, bodily pain), reduction rates were not significantly different between migraine and tension-type headache.
Patients with migraine/tension-type headache: number of days with headache and secondary outcomes for the three treatment groups: 3-month changes from baseline

Non-randomized comparisons
Comparison of the randomized and non-randomized acupuncture groups (Table 2b) after 3 months revealed that the acupuncture effect was more pronounced in non-randomized patients with regard to six of the 10 SF-36 subscales and the physical component scale.
Multivariate analysis
Factors affecting 3-month headache days
According to the multivariate analysis, consistently over all headache patients and independent of the treatment group, the 3-month reduction of headache days was more pronounced with higher baseline pain intensity (P < 0.001), with higher baseline values on mental component score for quality of life (P = 0.001), and with lower age (P < 0.001). In both types of headache the reduction of headache days increased with the number of baseline headache days, but this dependency was far more pronounced in migraine than in tension-type headache (P < 0.001). On average, reduction was higher in tension-type headache (P < 0.001). In acupuncture patients only, reduction in headache days was higher with shorter duration of complaints (P < 0.001) and with higher routine percentage of acupuncture treatments of the physician (P < 0.001). After inclusion of these baseline variables, treatment responses were not any more significantly different between randomized and non-randomized acupuncture patients, i.e. the selection due to the randomization requirement could be completely explained by the model. After adjustment, the additional percent reductions of headache days were estimated to be 27.0% (24.0%, 30.3%) and thus similar to the unadjusted estimates (Table 2). The physician's acupuncture qualification (hours of training, years of experience) had no significant influence on the effect of the treatment.
Maintenance of acupuncture effects over 6 months
The 6-month follow-up results observed in the treatment groups are shown in Table 3. The 3-month successes were essentially maintained and only slightly reduced. In the randomized acupuncture group, the 6-month responder rate was 42.9% for migraine and 45.3% for tension-type headache. In the non-randomized group the responder rate was 45.0% for migraine and 47.9% for tension-type headache.
Patients with migraine/tension-type headache: number of days with headache and secondary outcomes for the randomized groups: 6-month changes from baseline

Lower values indicate better status.
Control group also received acupuncture.
Delayed acupuncture
After delayed acupuncture control, patients essentially kept up with the patients randomized to immediate acupuncture therapy (Table 3). There were no significant differences between the randomized groups. However, immediate acupuncture was slightly but not significantly superior to delayed acupuncture in the 6-month responder rate (44.4.0% vs. 40.9%, P = 0.148).
Side-effects
In 10.7% of patients (n = 1268), a total of 1519 side-effects were reported after receiving acupuncture: 63%, (n = 960) minor local bleeding or haematoma, 16% (n = 246) pain, e.g. needling pain, 3% (n = 41) local infections at needle insertion place, 8% (n = 125) vegetative symptoms and 10% (n = 147) other. No life-threatening side-effects were reported.
Discussion
Patients with headache treated with acupuncture in addition to routine care showed significant improvements in symptoms and quality of life compared with patients who received routine care alone. In patients who consented to randomization, treatment outcomes after acupuncture were similar to those in patients who declined randomization. All of the differences observed can be explained by differences at baseline. Besides the routine percentage of acupuncture treatments, physician characteristics, such as the level of formal acupuncture training or certification, did not influence treatment outcomes, whereas patients with shorter duration of complaints benefited more from acupuncture treatment.
The present study is, to our knowledge, the largest randomized trial of acupuncture to date, including 12% of physicians specializing in acupuncture and about 4% of all primary care physicians in Germany. The study took a pragmatic approach, aiming to evaluate acupuncture in a manner that would reflect as closely as possible the conditions of daily medical practice and maximize external validity. The study had high follow-up rates. We used conservative methods to deal with missing data. The additional inclusion of patients who declined randomization allowed investigation of any potential selection effects.
Obviously, such an approach also has its methodological limitations. In this study, neither providers nor patients were blinded to treatment. Although the main outcome was assessed by the patients, bias due to unblinding cannot be ruled out. To minimize social acceptability bias, all questionnaires were sent directly from and to the coordinating research institute. Because the specifics both of acupuncture treatment and of any cointerventions were left to the discretion of the physicians, the treatment regimens of patients in our study were highly variable. Another limitation was that our only source for drug use was health insurance data, and over-the-counter usage was not evaluated. Inclusion criteria were broad, which resulted in a heterogeneous patient sample with high co-morbidity and possibly some diagnostic misclassification. The differential diagnosis of the type of headache (migraine or tension-type headache), especially, was not done by a specialist and may in some cases be inaccurate. Although these issues might be considered limitations from an experimental perspective, the study design was chosen to reflect general medical practice. Usually it is standard in studies on patients with headache to use diary data. Due to the routine care situation and the large number of patients, we decided to use data from questionnaires. There may therefore be a little inaccuracy in the data due to not fully correct memory. Patients were asked to indicate the number of days with headache during the last month. Because of this short period, greater failures of memory can be excluded.
Patient's self-selection in randomized studies of complementary and alternative medicine could be a relevant problem (14). Although a variety of designs have been recommended for including both randomized and non-randomized patients, only few studies have actually employed them to date (15) In our study, approximately three in four eligible patients refused randomization in spite of a (minor) financial incentive and the slight disadvantage of having a 50% chance of a 3-month delay before starting acupuncture treatment (following an average disease duration of 9.4 years). Although differences with respect to both baseline characteristics and treatment outcomes between randomized and non-randomized patients were small in absolute numbers, our findings indicate that randomization was associated with some selection effects. Therefore, the use of study designs that also include non-randomized patients appears to be desirable.
It is of note, however, that treatment benefits were similar in the randomized and non-randomized acupuncture groups after adjusting for baseline differences. This suggests that the results of randomized trials can be representative of routine medical care situations, at least in large pragmatic studies. Further support for this observation is derived from reports of similar results comparing randomized controlled trials with observational studies (16).
Both in randomized and non-randomized patients, the improvements in pain and quality of life after acupuncture were clinically relevant. An important finding of our study is that improvements seen immediately after completion of 3 months’ treatment continued for at least another 3 months.
Our pragmatic study cannot answer the question as to whether the effects observed may be due, at least in part, to ‘placebo’.
Our findings are consistent with another randomized trial comparing acupuncture treatment with usual care in patients with headache (17): patients in the acupuncture group experienced the equivalent of 22 days of headache fewer per year. According to the authors’ conclusion, ‘acupuncture leads to persisting, clinically relevant benefits for primary care patients with chronic headache, particularly migraine’.
Parallel to the present study, we also performed two smaller randomized controlled trials (each of 300 patients) comparing acupuncture with a sham intervention (minimal acupuncture–superficial needling at non-acupuncture points) and with a waiting list control in patients with chronic migraine and tension-type headache. Although acupuncture was clearly superior to the waiting list control, there were no significant differences compared with minimal acupuncture (18, 19). The results of other sham-controlled trials in patients with chronic headache are ambiguous, whereas comparisons with waiting list controls have consistently reported positive findings (12). This suggests that acupuncture in headache patients has relevant clinical effects, but that the selection and localization of correct points might make only a small difference. The finding that the formal qualification of the physician and the years of acupuncture experience had no significant influence on treatment outcome could be interpreted as a further indication that formal acupuncture training has only a limited role in the treatment effect. However, these results should be interpreted with caution, because the indicators in the present study might not adequately reflect the quality of a physician's treatment. Our study provides further evidence that acupuncture is a safe intervention. This is in agreement with large, previously published surveys (20, 21). When interpreting these findings, however, it must be borne in mind that all acupuncture in this study was administered by physicians.
Acupuncture is a relatively resource-intensive intervention due to the time involved for physicians and patients alike. In this context, the question of cost-effectiveness becomes important. To date, only one randomized trial of acupuncture for chronic headache has included a methodologically sound analysis of cost-effectiveness (22). The authors concluded that acupuncture is relatively cost-effective compared with a number of other interventions provided in the UK. Part of this study will also be a cost-effectiveness analysis that will be reported elsewhere (23).
In conclusion, our study has shown that treating patients with headache in routine primary care in Germany with additional acupuncture resulted in a clinically relevant and persistent benefit. Therefore, acupuncture should be considered a viable option for patients with headache.
Footnotes
Competing interests
None to declare.
Acknowledgements
The authors thank Katja Wruck for data management, Iris Bartsch, Beatrice Eden and Sigrid Mank for data acquisition, the members of the advisory board (Dr Konrad Beyer, Dr Josef Hummelsberger, Dr Bodo Liecker, Hardy Müller, Dr Albrecht Molsberger, Dr Helmut Rüdinger, Dr Wolfram Stör, Dr Gabriel Stux) for helpful advice, and all participating physicians and patients. This study was funded by the following health insurance companies: Techniker Krankenkasse (TK); Betriebskrankenkasse (BKK) Aktiv; BKK Bosch; BKK Daimler Chrysler; BKK Bertelsmann; BKK BMW; BKK Siemens; BKK Deutsche Bank; BKK Hoechst; BKK Hypo Vereinsbank; BKK Ford; BKK Allianz; BKK Vereins- und Westbank; Handelskrankenkasse (HKK); Innungskrankenkasse (IKK) Hamburg.