
Abstract
A growing number of clinical trials are testing Chinese acupuncture in the management of headache disorders. Little is known, however, about the relationship between International Headache Society diagnostic criteria and traditional Chinese medicine (TCM) diagnosis in primary headache disorders. We conducted a secondary analysis of the data of the prospective, controlled, blinded German acupuncture trials for migraine and tension-type headache. Data were collected from 1042 headache patients, of whom 633 were diagnosed with migraine and 409 with tension-type headache. We found that the diagnoses of migraine and tension-type headache were mirrored by different patterns of TCM diagnoses, with the patterns Liver Yang Rising, Liver Fire Rising, and Phlegm appearing to be best suited to differentiating between migraine and tension-type headache. Although not unexpected, given that the diagnosis of primary headache disorders in both diagnostic systems is based largely on the nature and quality of patient-reported symptoms, this finding suggests that migraine and tension-type headache are associated with different patterns of TCM diagnosis.
Introduction
Acupuncture is gaining increasing importance for the treatment of headache in Western medicine. As recently as 2001, a major Cochrane review concluded that acupuncture had some value for the treatment of idiopathic headaches but that the quality and quantity of evidence were not fully convincing (1). The authors stated that there was an urgent need for well-planned, large-scale studies to assess the efficacy and cost-effectiveness of acupuncture under real-life conditions. Since then, several trials have been published meeting those criteria (2). For migraine (MIG), Linde et al. found that both verum and sham acupuncture were superior to a waiting list control, and Diener et al. demonstrated that for MIG, 11 acupuncture treatments, whether verum or sham, given over 6 weeks, were at least as effective as standard medical prophylaxis with drugs on a daily basis over 6 months (3,4). For tension-type headache (TTH), Endres et al. showed that acupuncture treatments over 6 weeks lowered the number of headache days from 15.6 to 6.0 per month (5). Coeytaux et al. demonstrated that medical management by headache specialists was significantly improved when supplemented with acupuncture (6), and Witt et al. found that acupuncture is a cost-effective treatment in patients with primary headache (6,7). For TTH, limited efficacy of verum acupuncture compared with sham acupuncture was demonstrated by a recent meta-analysis of all randomized controlled trials up until August 2007 (8).
In Western medicine, according to diagnosis of headache using the classification of the International Headache Society (IHS), MIG and TTH are the two most prevalent diagnoses (9). Although clearly defined criteria exist for these diagnoses, individual patients can differ considerably, for example with regard to the quality and exact location of pain (including individual tender points), type of onset, or sensitivity to environmental factors (psychological stress, weather conditions), which often makes it difficult to attribute symptoms to an IHS diagnosis of either MIG or TTH (10). In contrast, the approach taken in traditional Chinese medicine (TCM) is to associate headache with the location of the pain, which is then associated with sets of acupuncture meridians or patterns of Chinese syndromes (11,12). According to the concepts of TCM the life energy Qi flows through 12 main organs and 12 meridians, arriving at the surface at 359 classical acupuncture points. In certain conditions such as headache, blockages may hamper the free flow of Qi, resulting in pathological conditions of too little Qi (deficiency) or too much Qi (excess) in certain organs or areas of the body. Activating acupuncture points is supposed to dissolve these Qi blockages. For a typical headache treatment, 12–25 needles are inserted, about half of them in the region of the head. Major acupuncture textbooks emphasize that because acupuncture is imbedded in Chinese medicine, a genuine TCM diagnosis, based on meridians and syndromes, is fundamental for a successful acupuncture treatment of headache. The major randomized clinical trials mentioned above are among the first to have taken this claim into account and designed study protocols where acupuncture points are selected according to affected meridians and Chinese syndromes (13,14). In this study, we present an analysis of the GERAC headache trials in order to explore the relationship between TCM and diagnoses of MIG and TTH.
Methods
Patients
Patients with MIG or TTH enrolled in this randomized controlled, multicentre, patient- and observer-blinded trial were recruited from office-based physicians (149 physicians for MIG and 122 for TTH) in 11 federal states in Germany during the time from 2002 to 2005. The design of this trial (GERAC-Germany Acupuncture Trials) has been described in detail elsewhere (3,5,13,15).
In order to assure equal attention to patients in all treatment groups, patients were diagnosed according to IHS criteria as well as TCM criteria before being enrolled in the study and randomized into the treatment groups. All the physicians involved had to have completed a minimum of 140 h of acupuncture training and have passed a nationally recognized examination, have at least 2 years of clinical experience in acupuncture, and have completed a 1-day training seminar covering treatment modalities and documentation prior to the trial.
Migraine
The main inclusion criteria for MIG were: German-speaking patient; aged 18–65 years; and willingness to provide written informed consent. Subjects had to report between two and six MIG attacks in the past 4 weeks, first MIG attack before the age of 50 years, MIG diagnosis at least 26 weeks before study entry, and duration of MIG attacks 4–72 h without acute medication or at least 2 hours with acute medication. Additionally patients had to have at least one of the following: nausea, vomiting, photophobia, or phonophobia. The main exclusion criteria were: severe MIG attacks with inability to go to work on more than 4 days a month; other neurological disease; secondary headache; neuralgia of the face or head; more than 6 days of non-migrainous headache per month; previous unsuccessful treatments with beta blockers; drug abuse; pregnancy; lactation; insufficient contraception; and intake of antipsychotic or antidepressant drugs. Patients were also excluded if they: had participated in another clinical headache trial; had taken analgesics on more than 3 days a month for other chronic pain; used prophylactic medication for MIG in the past 6 months; were receiving cortisone treatment; had epilepsy had a psychiatric disease; had any acupuncture treatment during the previous 12 months; or had any prior use of acupuncture for headache (to maximize blinding).
Tension-type headache
The main inclusion criteria for TTH were: German-speaking patient; aged 18–65 years; and willingness to provide written informed consent. Subjects had to meet IHS diagnostic criteria for TTH: at least 10 headache days per 4 weeks, with a headache day defined as a day on which headache lasts at least 4 hours or when analgesics are taken for headache pain, in which case the headache pains could persist for less than 4 hours. The principle exclusion criteria were: duration of symptoms less than 6 months; >1 MIG headache day per 4 weeks; medication overuse headache or other secondary headaches; other severe pain disorders; use of analgesics other than aspirin, acetaminophen and NSAIDs; TTH prophylaxis during the previous 12 months; any acupuncture treatment during the previous 12 months; any prior use of acupuncture for headache (to maximize blinding).
TCM diagnosis
In TCM, the concepts of ‘MIG’ and ‘TTH’ do not exist. Instead, diagnosis for headache is based on multilateral information including quality and location of pain, the corresponding acupuncture meridians, internal/external factors and multiple body function states, all of which are taken into consideration to arrive at the final TCM diagnosis, which includes TCM syndromes and affected meridians (11,12). Because until now no standard diagnostic procedure or category has existed for chronic headache in TCM, we defined a diagnostic protocol in accordance with literature sources (about 40 acupuncture textbooks, either German, American or translated from Chinese) and discussions with leading experts in Germany in this field (13). The experts had at least 8 years of clinical experience with acupuncture (mean 20 years), and had published and taught in the field of acupuncture. In all, 12 different diagnoses were identified as being related to headache: four meridian diagnoses and eight TCM syndromes (see below). The same diagnostic criteria were used for all the patients in our study, both MIG and TTH groups.
Meridian diagnoses were according to the location of the pain. Headaches are classified in TCM as: (i) Shaoyang (TW-GB channels, on the sides of the head); (ii) Yangming (LI-ST channels, forehead); (iii) Taiyang (SI-BL channels, occiput); and (iv) Jueyin (PC-LR channel, top of the head).
Syndrome diagnoses were based on information from analysing organ functions, internal/external factors, clinical symptoms, and tongue diagnosis. Four syndromes (5–8) are considered to be more specific for headache. These are: (5) Liver Qi Stagnation, (6) Liver Yang Rising, (7) Liver Fire Rising, and (8) Phlegm. The final four diagnoses (9–12) are attributed more to deficiencies (Qi, Blood, Yang), possibly underlying headache problems: (9) Spleen Qi Deficiency, (10) Liver Blood Deficiency, (11) Kidney Yin Deficiency, and (12) Kidney Yang Deficiency.
Two other syndrome patterns that are also responsible for chronic headache were not included in this protocol because they were judged to be related to symptoms that would have led to exclusion in our trial: Liver Wind Rising, often leading to serious neurological symptoms in addition to MIG, and Liver Blood Stagnation, often accompanied by tumour, stroke (Blood Stagnation of the CNS), or severe pain syndromes of the cervical spine (11,16). Here it is important to mention that the organ name of the TCM syndrome is simply a traditional convention, not referring to physiological or anatomical properties as known in western medicine.
To our knowledge, validated, standardized approaches to ascribing TCM diagnoses to patients with MIG or TTH have not been reported in the published literature. Therefore, for the purposes of this study, the acupuncture experts in the GERAC group developed a patient questionnaire by a two-step Delphi system to assist the physicians in choosing the appropriate syndromes. Firstly, two experts (first author and G. Stux) made suggestions for the items of the questionnaire; secondly, this proposal was discussed with two other experts from the study group; and thirdly, these results were incorporated into the questionaire. Although it has not yet been validated, the GERAC headache questionnaire is the most exact and formal approach to TCM syndromes for headache currently available.
For each TCM syndrome the questionnaire provided six to eight questions concerning the typical clinical symptoms (supplement 1). Each question had to be answered on a scale from 1 to 4 according to the severity of the symptom. The tongue diagnostic characteristics were also described in the questionnaire as hints for the physicians. The questionnaire was completed either by the physician during the interview with the patient, or by the patients themselves. For each patient, up to five diagnoses (from a total of four channel diagnoses and eight syndrome diagnoses) could be selected by the physician.
Outcome measures
Our main objective is the analysis of the distribution pattern of all 12 TCM diagnoses. The distribution of the 12 TCM diagnoses in MIG and TTH patients was compared independent of their allocation to treatment.
Statistical analysis
The present publication is a secondary analysis of the study data. The primary objective of the GERAC trials was not to compare TCM diagnoses, but rather to compare responder data among the different treatment groups. Therefore, the results must not be used as posteriori formal statistical proof of an unequal distribution of the TCM diagnoses but nevertheless as evidence for this unequal distribution.
We compared the distribution of the TCM diagnoses in the two headache groups using Fisher's exact test. The Bonferroni correction was used to adjust for multiple tests. A P-value of <0.004 was considered statistically significant. To determine the probabilities of the individual diagnoses, additional confidence intervals were calculated using the binomial function. Because the confidence intervals are used only to determine how accurately the probabilities have been determined, no multiple tests are necessary and hence no adjustment to the significance level of <0.05. All analyses were performed using SAS software version 9.13 (SAS Institute Inc, Cary, NC).
Results
Pattern of TCM diagnoses
Number of TCM diagnoses per patient
For 75% (n = 471) of MIG patients and 79% (n = 321) of TTH patients, 2, 3 or 4 of the total of 12 possible diagnostic patterns were identified by the diagnosing physician. No TCM diagnosis was given for 6% (n = 23) in the MIG group and 1% (n = 6) in the TTH group. Even though only a maximum of five TCM diagnoses were allowed, six diagnoses were given in seven TTH cases, and seven diagnoses were given in one MIG and one TTH case. (Fig. 1)
Number of TCM diagnoses per patient in the total population. MIG: n = 633. TTH: n = 409 (ITT). Physicians could select from 12 possible diagnoses. They were asked to attribute not more than five TCM diagnoses per patient. MIG, migraine; TCM, traditional Chinese medicine; TTH, tension-type headache.
Combined data for MIG and TTH
Data were collected from 1042 patients. The most common channel diagnosis was Shaoyang headache (50%, n = 518). The most common syndrome diagnoses were Liver Qi Stagnation (n = 586) and Liver Yang Rising (n = 579), at about 56% each, followed by Spleen Qi Deficiency (48%, n = 497). The Liver Fire Rising (n = 126) and Kidney Yang Deficiency (n = 131) syndromes had the lowest frequency at 12% (Fig. 2, Table 1).
Pattern of TCM diagnoses for MIG and TTH combined. Diagnosis: (1) Shaoyang (TW-GB meridians), (2)Yangming (LI-ST meridians), (3) Taiyang (SI-BL meridians), and (4) Jueyin (PC-LR meridian); (5) Liver Qi Stagnation, (6) Liver Yang Rising, (7) Liver Fire Rising, (8) Phlegm, (9) Spleen Qi Deficiency, (10) Liver Blood Deficiency, (11) Kidney Yin Deficiency, and (12) Kidney Yang Deficiency. MIG, migraine; TCM, traditional Chinese medicine; TTH, tension-type headache. Pattern of TCM diagnosis for MIG and TTH separately
P < 0.001. Fisher's exact test with Bonferroni correction for multiple testing. MIG, migraine; TCM, traditional Chinese medicine; TTH, tension-type headache.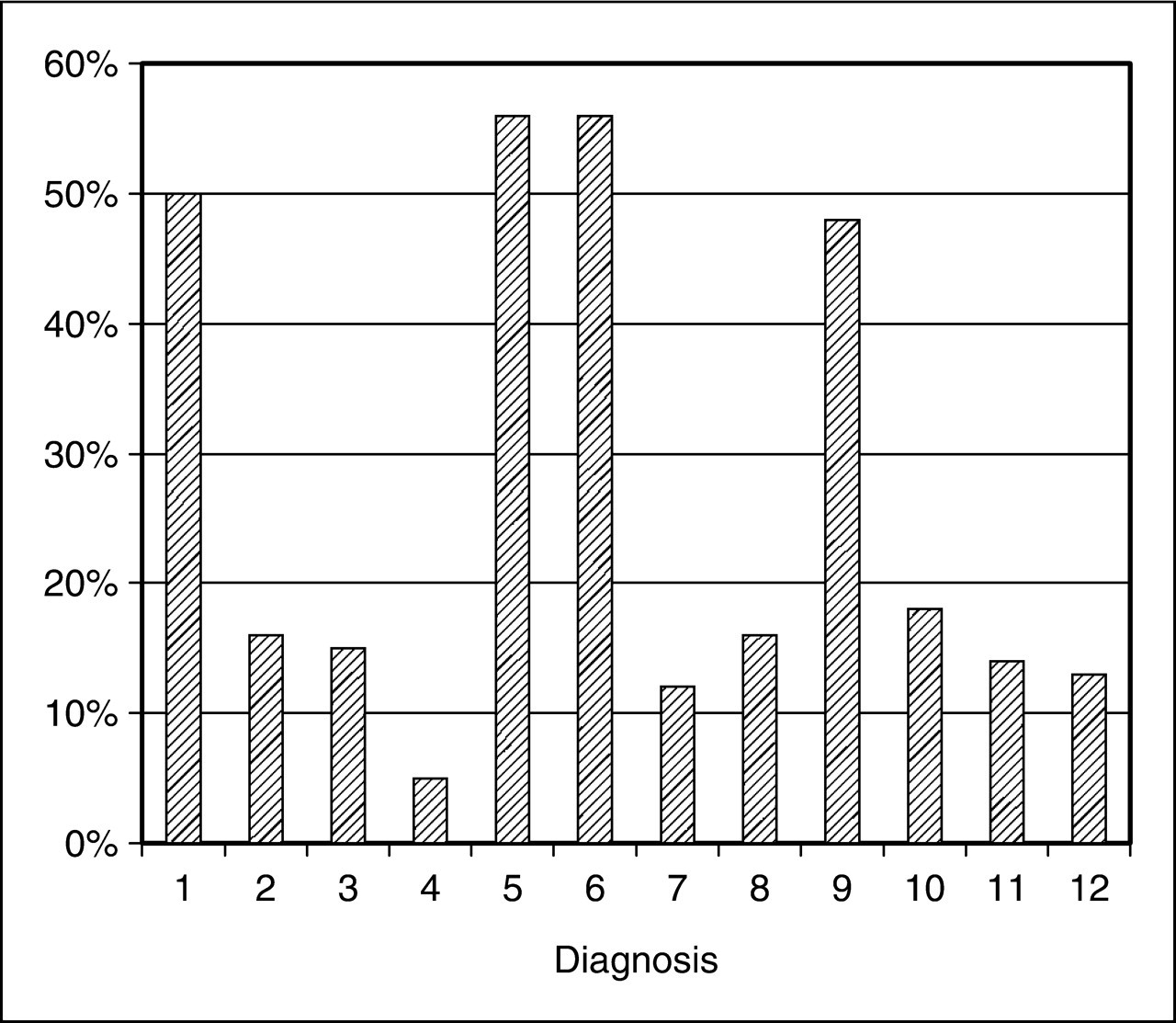

Comparison between MIG and TTH
There were 633 MIG patients and 409 TTH patients. Significant differences in the frequency of the diagnoses were seen only for the diagnoses Taiyang (SI-BL meridians), Liver Yang Rising, Liver Fire Rising, Phlegm, Liver Blood Deficiency, Kidney Yin Deficiency, and Kidney Yang Deficiency (P < 0.001).
Meridian diagnoses: In both MIG and TTH groups the most common diagnosis was Shaoyang headache (TW-GB meridians on the sides of the head), diagnosed in 53% (n = 336) of the MIG cases and 44% (n = 182) of the TTH cases (P < 0.008). The least common meridian diagnosis was the Jueyin headache (related to the PC–LR meridians and the vertex of the head), diagnosed in 5% (n = 30) of MIG cases and 7% (n = 27) of TTH cases. The largest difference in frequency of occurrence between TTH and MIG was found in the Tai Yang headache (related to the BL—SI meridians and the medial area, extending from the occiput to the inner angle of the eye); TTH headaches are more frequently related to this area than are MIG headaches (P < 0.001) (Fig. 3, Table 1).
Pattern of TCM diagnosis for MIG and TTH separately. Diagnosis: (1) Shaoyang (TW-GB meridians), (2) Yangming (LI-ST meridians), (3) Taiyang (SI-BL meridians), and (4) Jueyin (PC-LR meridian); (5) Liver Qi Stagnation, (6) Liver Yang Rising, (7) Liver Fire Rising, (8) Phlegm, (9) Spleen Qi Deficiency, (10) Liver Blood Deficiency, (11) Kidney Yin Deficiency, and (12) Kidney Yang Deficiency. MIG, migraine; TCM, traditional Chinese medicine; TTH, tension-type headache.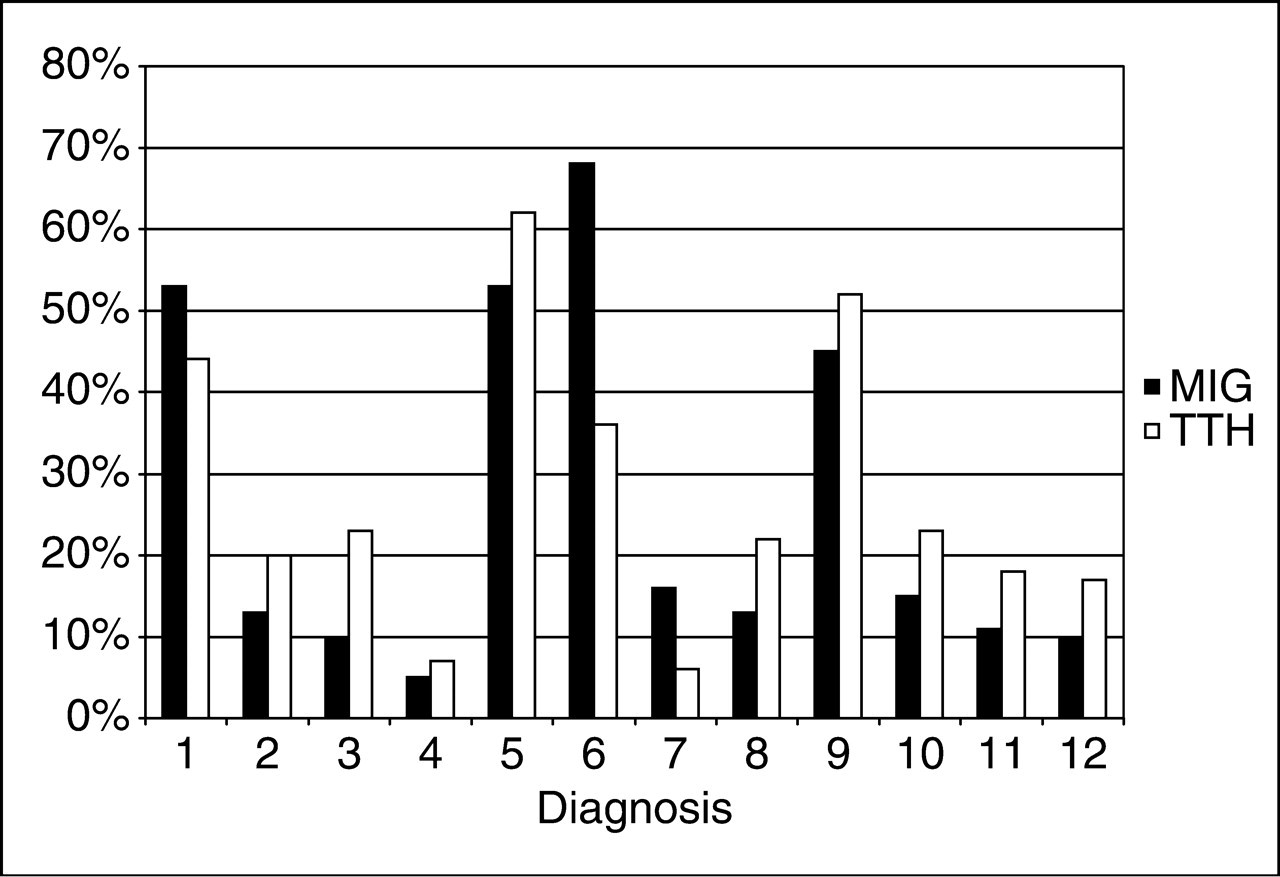
Syndrome diagnoses: In the MIG group the most commonly diagnosed syndrome was Liver Yang Rising (68%, n = 430), followed by Liver Qi Stagnation (53%, n = 334) and Spleen Qi Deficiency (45%, n = 286). In the TTH group, the most frequently identified syndrome was Liver Qi Stagnation (62%, n = 252), followed by Spleen Qi Deficiency (52%, n = 211) and Liver Yang Rising (36%, n = 149). The level of significance (P < 0.001) was reached for Liver Fire Rising and Liver Yang Rising, which were predominant in MIG, and Phlegm, which was predominant in TTH. Overall, TTH patients had more diagnoses related to ‘Deficiency’ with Spleen Qi Deficiency, Liver Blood Deficiency, Kidney Yin Deficiency and Kidney Yang Deficiency all being found more frequently in TTH than in MIG; the difference is significant (P < 0.001) for diagnoses of Liver Blood Deficiency, Kidney Yin Deficiency and Kidney Yang Deficiency (Fig. 3, Table 1).
Discussion
This secondary analysis of data from a prospective, controlled study of 1042 headache patients, made up of 409 patients with TTH and 633 patients with MIG, strictly selected according to internationally recognized diagnostic criteria (IHS), is to our knowledge the first attempt to describe the pattern of TCM diagnoses associated with MIG or TTH as such, as well as differences in the frequencies of TCM diagnoses associated with MIG and TTH separately. The analysis shows that at least 75% of headache patients were diagnosed with two to four different TCM patterns. The typical primary headache patient suffers from Liver Qi Stagnation and/or Liver Yang Rising accompanied by Spleen Qi Deficiency and the pain is located on the side of the head, affecting the Shaoyang axes with the GB and TW meridians. Liver Fire Rising and Liver Yang Rising are more characteristic of MIG, while Phlegm is more common in TTH. TTH patients are more likely to suffer from deficiency syndromes, especially Liver Blood Deficiency, Kidney Yin Deficiency and Kidney Yang Deficiency, and TTH headache more often affects the area of the Taiyang BL—SI meridian axis. Liver Yang Rising, Liver Fire Rising and Phlegm appear to be the most important TCM diagnoses for differentiating between MIG and TTH, the first two being found more often in MIG and the last being found more often in TTH. Other characteristics that may be useful for headache diagnosis within the system of TCM, although they did not meet our level of significance, are: Liver Qi Stagnation is more frequent in TTH, MIG headache is predominant in the Shaoyang region (side of the head) and TTH is predominant in the Yangming region (forehead). Spleen deficiency is very common in both types of headache and the Jueyin Region is so rarely affected that neither diagnosis is useful for differentiating between MIG and TTH. The observed differences in the proportions of TCM syndromes between patients with MIG and TTH range between 7% % (diagnoses 11 and 12) and 32% (diagnosis 06). This underpins the concept of Chinese medicine that relies on two to four diagnoses to differentiate between the different types of headache; also it is in accordance with our results, showing that more then 75% of the headache patients received two to four different TCM diagnosis.
The above findings support the main claims of TCM textbooks regarding TCM syndrome diagnosis in headache, which are that Liver Fire Rising, Liver Yang Rising and a typical location on the side of the head are more characteristic of MIG, while Phlegm and deficiency syndromes are more characteristic of TTH (11–13,16).
Our findings are also consistent with a survey by Coeytaux et al., who, although they use a different TCM terminology than we do, show that frequent headache is associated with a wide variety of TCM diagnoses, and that most patients appear to have Liver Yang and Qi disharmonies (10). There is a growing literature on the variability and reliability of TCM diagnosis by different practitioners for low back pain, arthritis, and other clinical conditions including headache. All these studies suggest that there is considerable variation among acupuncturists when it comes to the selection of TCM diagnostic patterns (17–22). This variability in diagnosis is not unique to Chinese medicine but also can be observed in Western medicine (e.g. differences in headache diagnosis by neurologists, orthopaedists and general practitioners), and there have been some attempts in the literature to assess the reliability of MIG and TTH diagnosis in Western medicine as well (23–25). To reduce this well-known variability in Chinese diagnosis, we provided the diagnosing physicians with an expert- and literature-based, predefined selection of possible TCM syndromes, supported by a patient questionnaire for Chinese syndromes that was specially developed for the GERAC headache trials and approved by experts.
The findings from this study may serve to inform, in a minor way, some unresolved issues in the scientific literature that pertain to the diagnosis of primary headache disorders. For example, the question of whether MIG and TTH represent two separate aetiologies as opposed to two points on a continuum has been actively explored in the literature for many years. In fact there is evidence in the literature that TTH and MIG do not exist as discrete pathophysiologic entities but form a continuum (23). By applying two different diagnostic systems (IHS criteria and TCM pattern and meridian diagnoses) to the same individuals who experience frequent headaches, we have demonstrated that: (i) there are differences in TCM diagnoses between patients with MIG compared with those with TTH; and (ii) there appear to be some variants or potential subcategories of both MIG and TTH that may correspond to established TCM diagnoses. Additional research is needed to further develop the idea that the TCM diagnostic system can: (i) help differentiate between MIG and TTH; (ii) identify subcategories of MIG or TTH; or (iii) be useful for prognosis or predicting clinical response to a given treatment.
Strengths and limitations
One of the strengths of our prospective study is the large patient population (n = 1042), clearly allocated to either MIG or TTH according to international recognized headache criteria. A clearly described procedure for TCM diagnosis makes our study reproducible. Furthermore, the large number of physicians involved (149 physicians for MIG and 122 for TTH) gives our data a high external validity for describing the situation of TCM diagnosis as it relates to acupuncture treatment in Germany.
Our data are compromised by several methodological factors. We did not design a strict algorithm that would lead from the patients' answers to the TCM diagnostic questionnaire inevitably to a specific Chinese diagnosis. Instead, the questionnaire assisted the physician in finding the appropriate Chinese syndrome pattern, but ultimately the physician was free to draw on the answers to the questionnaire, his own theoretical background and his own clinical experience to arrive at a final Chinese diagnosis or diagnoses. We believe that this procedure best reflects the clinical reality of the physician, because we did not force physicians to conform to the limitations of an artificial clinical situation created by the demands of a RCT design. Also, physicians could select up to five TCM diagnoses for a single patient. While in actual fact the physician might consider one syndrome to be more important than another, or might consider one syndrome to be the underlying cause for the others, we were only able to count all syndromes equally, without weighting. Because our data are based on a secondary analysis of the GERAC trial data, our findings do not prove but are suggestive of the differences in diagnostic patterns between MIG and TTH. Finally, the fact that the physicians who diagnosed subjects as having MIG vs TTH using IHS criteria were also the clinicians who ascribed TCM diagnoses to each subject introduces the possibility of bias if the clinicians had preconceived ideas about certain TCM diagnoses being associated with MIG or TTH.
Conclusion
The data from this study show that in TCM diagnosis for headache patients, physicians attribute between two and four TCM syndromes to a headache patient. Typical TCM syndromes for headache patients in general are Liver Qi Stagnation, Liver Yang Rising, and Spleen Qi Deficiency. While Liver Fire Rising and Liver Yang Rising are more characteristic of MIG, Phlegm is more common in TTH. Deficiency syndromes (Liver Blood Deficiency, Kidney Yin Deficiency and Kidney Yang Deficiency) are more present in TTH. Because our study is based on a secondary analysis, a future study should look at the distribution of Chinese syndrome patterns in headache as the primary outcome criterion.
Footnotes
Acknowledgements
We are thankful to Hans J. Trampisch for discussions on the topic, Cornelia Scharzweller, Kai Kronfeld and Daniel Wachtlin for the configuration of the data set, and Gabriel Stux for his contribution to the development of the GERAC headache questionnaire.
For each of the following symptoms, please indicate the frequency/severity on a scale from 1 to 4: