
Abstract
In conformity with current views on patient empowerment, we designed and evaluated the effects of home-based behavioural training (BT) provided by lay trainers with migraine to small groups of fellow patients. The primary aims of BT were to reduce attack frequency and increase perceived control over and self-confidence in attack prevention. In a randomized controlled trial the BT group (n = 51) was compared with a waitlist-control group (WLC), receiving usual care (n = 57). BT produced a minor (-21%) short-term effect on attack frequency and clinically significant improvement in 35% of the participants. Covariance analysis showed a non-significant trend (P = 0.07) compared with WLC. However, patients’ perceived control over migraine attacks and self-confidence in attack prevention increased significantly with large effect sizes. Patients with high baseline attack frequency might benefit more from BT than those with low attack frequency. In conclusion, lay trainers with migraine strengthened fellow patients' perceived control, but did not induce a significant immediate improvement in attack frequency.
Introduction
Although migraine is highly prevalent and burdensome in daily life, many patients do not seek medical treatment (1). Extending the reach of education and treatment is thus a pressing issue and should be realized cost efficiently, given the high prevalence. One method is to involve migraine patients as lay trainers, which has proved effective in educating patients with frequent episodic migraine from a clinic-based population (2). The present study extends the role of lay trainers with migraine from the clinic to the open population and from education to training of skills to prevent migraine attacks.
The pharmacological treatment of migraine is focused on abortion and prevention of attacks, and its efficacy is well established (3). Attack prevention can also be accomplished with behavioural treatment or training (BT). According to meta-analyses, BT reduces attack frequency by 35–55% and is significantly superior to control conditions (4–6). BT is targeted at attack prevention through the following strategies: (i) detection and modification of migraine triggers; and (ii) employment of physiological self-regulation skills, which may be supported with cognitive techniques (4, 7). Individual home-based BT was found to be as efficacious as clinic-based BT and fivefold more cost-effective (8, 9). These treatment formats were based on less than half of the usual clinical contacts (3–4 instead of 8–12) and supplemented with written manuals and telephone support. Home-based BT and the employment of lay trainers with migraine accord with the current focus in healthcare and society on ‘patient empowerment’. This view holds that patients are experts in their chronic disease, share responsibility for its management and should therefore be involved in achieving efficient and effective healthcare (10–12). According to a meta-analysis, such health educational programmes significantly reduce disease parameters in hypertension (blood pressure) and diabetes (blood glucose control) (13) and increase self-efficacy, although pain in arthritis is not affected (14, 15). A recent study has shown that intensive education provided by lay trainers with migraine to their fellow-sufferers, supplementary to medical treatment, significantly decreases migraine disability and reduces headache days in the latter group (2). These results suggest that a home-based self-management approach might work in migraine and that lay trainers with migraine might be able to deliver such training to a group of fellow patients (9, 16–21).
This study presents immediate pre and post training results of a home-based BT provided by lay trainers with migraine to a small group of fellow patients at home. The primary aims of BT were to reduce attack frequency and increase feelings of control and self-confidence in attack prevention. The secondary aims were to improve patients' quality of life and to reduce migraine-related disability. Finally, this study also explores factors that might explain the changes in outcomes after BT.
Methods
Patients
According to the power analysis (22), 50 patients were required in each group, as a minimal between-group difference in attack frequency of 30% was needed to exceed the placebo effect (23). To account for potential drop-out, more patients were recruited (24). Patients were included according to the scientific guidelines of the International Headache Society (IHS) subcommittee on clinical trials (25). Participants had to be aged 18–65 years, fulfil the IHS criteria for migraine with (G43.1) or without (G43.0) aura (26) and have an attack frequency of one to six per month. Excluded were patients with headache occurring on ≥ 15 days per month, a migraine duration of < 1 year, migraine onset at age > 50 years referring to underlying organic disease (25), and an above average score (> 178) on the Symptom Checklist 90 (SCL-90) (27), indicative of psychopathology.
The study was carried out in cooperation with the Dutch Society of Headache Patients and profited from its support and website for recruitment. To reach a broad population, members of the patient organization were invited, local headache specialists could refer patients, and newspapers, magazines and websites of the research centres were used. Migraine patients interested in BT, which was provided by an experienced fellow patient, were asked to respond if they did not suffer from daily headaches and were living in or around the research centres at Rotterdam (including Leiden) and Utrecht (including Amsterdam). The selection of participants was based on: (i) a standard questionnaire covering the IHS classification criteria (26), which also inquired whether subjects had consulted a physician and had been diagnosed with migraine; (ii) a 4-week headache diagnostic diary; (iii) the SCL-90 psychopathology screening list. The presence of migraine with aura was derived from the IHS questionnaire and headache diaries. Two headache specialists were consulted for a second opinion on included patients and to verify the diagnoses in case of doubt, and to rule out headache due to medication overuse. The Ethics Committee of the Erasmus Medical Centre approved the study.
Study design and procedure
The study design was a randomized, controlled trial in which eligible patients were randomly allocated to the BT condition or to a waitlist-control (WLC) condition. The WLC condition was chosen in view of the difficulty previous studies have had in realizing a placebo procedure that was plausible and also provided non-therapeutic control for attention (28, 29). Comparison with a professional therapist group was not an aim of this study; the focus was whether or not this innovative approach might work. Moreover, such an equivalence study would require a much larger sample size and considerable resources. Parallel measurements were conducted in both groups pre-BT (4 weeks) and post-BT (4 weeks). The WLC group received BT after the waitlist period.
Participants were randomized by a statistician within blocks of the four cities blinded to the investigators, and were centrally assigned to BT or WLC according to a random number table. Participants were notified about their allocation prior to baseline measurement, because information about the start of BT was considered ethical and also necessary, because BT sessions had to be planned during baseline measurement. A research assistant assigned patients and trainers to BT training groups and scheduled the training sessions. He also blinded headache diaries to the researchers, to prevent assessment bias when they scored the diaries for the analyses.
BT was provided to three cohorts of the BT and WLC condition, respectively, and cohorts were separated by approximately 6 months to account for summer and winter vacations. Data collection took place from July 2003 to July 2006. The relatively low number of trained migraineur lay trainers produced a backlog of potential participants in the first year. In consultation with the patient organization, it was decided to allocate all enrolled but delayed patients to BT in the second year.
Home-based, group-delivered behavioural training and waitlist-control
BT was based on an established clinical protocol for individual treatment (30–33) and tailored to the format of a home-based group intervention. Patients received a written manual, an organizer for homework assignments, diary ratings and self-evaluations, and a CD-ROM with auditory relaxation exercises. The intervention consisted of BT strategies that are central to attack prevention in migraine: (i) identification and modification of triggers and affective, cognitive and behavioural premonitory symptoms; and (ii) use of physiological self-regulation skills. The main relaxation technique was autogenic training, which is commonly used in migraine and according to meta-analyses produces medium effect sizes in headache improvement (5, 34, 35). In addition, breathing exercises and cue-controlled relaxation were learned, as well as additional strategies to reduce physical or mental exertion proactively (through time-out or taking breaks) or arousal (through self-assurance and positive thinking).
BT consisted of seven 2-h sessions spread over 10 weeks. Sessions 1–3 were conducted weekly and focused on (i) detection of migraine triggers and premonitory symptoms (36, 37) by daily monitoring, and (ii) acquisition of relaxation skills by stepped practice of autogenic and breathing exercises twice per day at home. Trigger and symptom detection was supported by personal feedback of the trainer and group members and resulted in a personalized map of triggers and premonitory symptoms, which was tailored to the individual case. Relaxation skills were trained progressively by stepwise inclusion of cue-controlled relaxation, whereas autogenic exercises were condensed over time. Sessions 4–6 took place every 2 weeks and focused on: (i) application of relaxation skills and other proactive strategies under the condition that premonitory symptoms or triggers prevailed, while continuing the daily exercises at home; and (ii) a personalized prescription for migraine and health. Each participant formulated individualized target conditions of being at risk for developing a migraine attack, as well as individualized actions and lifestyle changes to reduce this risk and prevent attack occurrence. Evaluation took place in session 7, which included the specification of individual goals and actions to maintain training skills.
BT was delivered in smalls groups of two to four patients and its feasibility was established in a pilot study (16, 38). The WLC group continued their current treatment, i.e. care as usual. All participants were urged not to change their medication or start alternative migraine treatments while in the trial and to inform the researchers in case this was unavoidable. To keep participants informed and committed to the study, they received a newsletter about the research project once per year.
Lay trainers with migraine
Five lay trainers with migraine were recruited as part of the pilot study (16, 38) and nine were recruited during the trial. They lived in the vicinity of Rotterdam/Leiden (n = 8) or Utrecht/Amsterdam (n = 6) and underwent training consisting of three steps: (i) self-experience through receiving BT for their own migraine attacks; (ii) application of individual BT to one new patient under supervision of the first author; and (iii) provision of BT to a small group of new patients under continued supervision. Potential lay trainers with migraine could participate in step 2, provided that they were motivated to become a lay trainer and were successful in managing their own migraine attacks.
Trainers received a structured manual of the content and procedure per BT session, which included directives for basic trainer skills regarding instructions and evaluations of registration assignments and relaxation exercises, time-management of the sessions, and the provision of feedback and motivational or emotional assistance to trainees. They kept a brief evaluation form per session with track records per trainee. This form served as the basis for supervision by e-mail and telephone provided by the first author after BT sessions 1, 3 and 6. In addition, trainers participated in three 3-h workshops led by the second author, directed at the promotion of basic trainer skills while safeguarding their own migraine management. A fourth workshop focused on advanced knowledge of relaxation training and was given by an expert in the field of relaxation. The lay trainers with migraine received a payment of €150 (€14/h) for individual BT and €300 (€21/h) for a home-based group BT.
Measurements
The primary outcome variable, attack frequency per 4 weeks, was prospectively measured in a headache diagnostic diary according to the guidelines for clinical trials in prophylactic treatment (25). Pain intensity was rated by allocating the following score, every 6 h: 1, mild headache—I can do everything but with some difficulty; 2, moderate headache—I cannot do all or most things; 3, severe headache—I am unable to do things, bed rest is necessary. When migraine occurred, associated symptoms were registered per 24 h, as were brief descriptions of observed triggers or premonitory symptoms. Medication type and dosage unit for acute and preventive treatment were also registered per 24 h.
The two additional primary outcome variables, feelings of control and self-confidence regarding attack prevention, were assessed with questionnaire measurements of headache-specific locus of control and self-efficacy. Locus of control refers to the belief that the factors that influence the occurrence and relief of headache are within the individual's control (internal control) or are under external control, which is exerted either by chance or by a medical professional (39). Because the training was not designed to influence healthcare use, patients' belief in control by professionals was not further analysed. Self-efficacy refers to the confidence that one can take actions to prevent or manage headache episodes (40). We used a forward–backward method (41) to translate the 33-item Headache Specific Locus of Control Scale (HSLC) (39) and the 25-item Headache Management Self-Efficacy Scale (HMSE) (40) and tested their reliability in our sample. The (sub)scales of the HSLC and the HMSE yielded good to excellent internal consistency with a Chronbach α of, respectively, 0.91 (internal control,11-item subscale), 0.81 (external chance control, 11 items) and 0.90 (self-efficacy). The HMSE was translated during the first year of data acquisition and could therefore not be administered to about 25% of the total sample. The sum scores of the HSLC subscales were calculated separately to indicate the degree to which participants perceived self-control over migraine or attributed this control to chance. The sum score of the self-efficacy questionnaire was calculated (ranging from 25 to 175), whereby a higher score reflects stronger self-confidence in the patients' own capacity to prevent and manage attacks of migraine.
The secondary outcome variables concerned health status, migraine-specific quality of life and migraine-related disability. Health status was measured with the Dutch version of the Medical Outcomes Study 36-item Health Survey (SF-36) (42, 43), which is a validated instrument for the self-evaluation of physical and mental health and commonly used in migraine (44). The SF-36 comprises four scales for physical health (physical functioning, role-physical functioning, bodily pain and general physical health) and four for mental health (vitality, social functioning, role-emotional functioning and general mental health). Raw scores were linearly converted to a 0–100 scale and mean scores were calculated for physical and mental health status, with a higher score indicating better health. Quality of life between attacks was established with the 20-item Dutch version of the Migraine-Specific Quality of Life Questionnaire (MSQOL) with a sum score ranging from 20 to 80 (45). This questionnaire is valid, highly reliable and related to psychological well-being, perceived severity of migraine, and disruption of life caused by migraine (46). Migraine-related disability was measured with the Migraine Disability Assessment Scale (MIDAS), which consists of five questions concerning the number of days lost to migraine in the past 3 months. Internal consistency, reliability and validity of the MIDAS were shown to be satisfactory (47). The sum score reflects the number of productive days lost in settings considered to be the most important in middle-aged patients, i.e. the workplace and at home (48). The HSLC, HMSE, SF-36, MSQOL and MIDAS were administered pre- and post- BT and WLC.
Data analysis
Data from the headache diagnostic diary were prepared as follows. To count attack frequency, migraine episodes were identified according to the IHS criteria (26): headache had at least two migraine characteristics (unilateral location, pulsating quality, moderate or severe pain intensity and aggravation by physical activity) plus at least one associated symptom (nausea/vomiting; photo- or phonophobia). Since triptan use for acute treatment modifies clinical features (25), the diagnostic criteria for migraine were adapted as follows. If a triptan was used, headache was qualified as a migraine attack if (i) at least two of the above-described characteristics were present, but associated symptoms were absent, or (ii) one migraine characteristic was present, together with at least one associated symptom. A migraine attack that was interrupted by sleep or recurred within 48 h was counted as one attack (25). Medication use for acute treatment was calculated by counting separately the dosage units of triptans and of analgesics over the 4-week diary period (25). Patients who had > 25% of the items of a specific (sub)scale of a questionnaire missing were removed from the analysis on the sum score concerned.
The analyses were first carried out in the total sample that entered the baseline measurement according to the intention to treat (ITT) principle and repeated on subjects who completed the study protocol (CP) (49). The CP analysis is reported as primary analysis and ITT results are added when these differed from the CP results, e.g. significant in CP analysis and non-significant in ITT analysis. Results are presented as mean prepost differences per group and mean between-group differences, both unadjusted and adjusted for baseline scores and accompanied by 95% confidence intervals, indicating the precision of the estimates. Wilcoxon's two-sample test (Mann–Whitney U-test) was used to test differences in dichotomous variables between the BT and WLC group. Independent t-tests were used for continuous variables. Analyses of covariance (
In order to control for Type I error in the primary and secondary analyses, Bonferroni's correction was performed: 1 − (1 − α)1/m, with an α of 0.05 and m indicating the number of tests (50). According to this formula, a significance level of 0.0125 is required for the results of the primary analyses, but also for those of the secondary analyses given that the present study involved four analyses. The model used was checked for violation of the assumptions of normality, and attack frequency, internal locus of control, self-efficacy, migraine-specific quality of life, migraine disability and mental quality of life were transformed (square root) because of a non-normal distribution of the scores. Missing values of migraine frequency post training were estimated by using the maximum likelihood method (51). Explorative analyses were performed to explain the primary outcomes. The Bonferroni correction was not employed here given the tentative character of these analyses. Treatment responder rate was calculated for attack frequency, with a reduction > 50% indicating a clinically significant improvement (52). Differential attack reduction for those who entered BT with a high (4–6) vs. a low (1–3) attack frequency at baseline was performed and tested by 2 × 2 (group × baseline frequency)
Results
Patient flow through the study and participant characteristics
Participant flow through the study and reasons for attrition are shown in Fig. 1. Of the 264 subjects who gave informed consent, 135 (51%) were excluded because they did not return the materials (n = 48) or did not meet the inclusion criteria (n = 87). Of the latter group, 63% had a headache frequency that was either too low or too high, 21% were excluded for diagnostic reasons provided by the headache specialists, and 16% scored above the SCL cut-off score for psychopathology. After randomization of the 129 participants (BT: n = 61, WLC: n = 68), 21 resigned or stopped. Of these patients, one in each condition resigned before baseline. Therefore, the ITT analyses included 60 subjects in the BT and 67 in the WLC group, while 108 patients were included in the CP analyses. Missing values due to missing headache diaries were 7% in the ITT analyses and 1% in the CP analysis.

Patient flow chart. BT, Behavioural training; CP, completed protocol; DSHP, Dutch Society of Headache Patients; ITT, intention to treat; WLC, waitlist-control.
Table 1 presents the characteristics of the 129 selected patients. At baseline, the BT and WLC groups were similar regarding demographics, migraine characteristics and medical history. The total MIDAS score (3, 24) showed a relatively high disability compared with population studies from the USA (5, 19) and the UK (8, 12, 47). The number of patients who changed their medication during the trial was comparable between the BT (18%) and WLC (18%) groups. The number of life events during the training period also did not differ significantly (BT, 39%; WLC, 30%).
Characteristics of the BT and WLC groups summarized for all patients and for subjects who completed the protocol
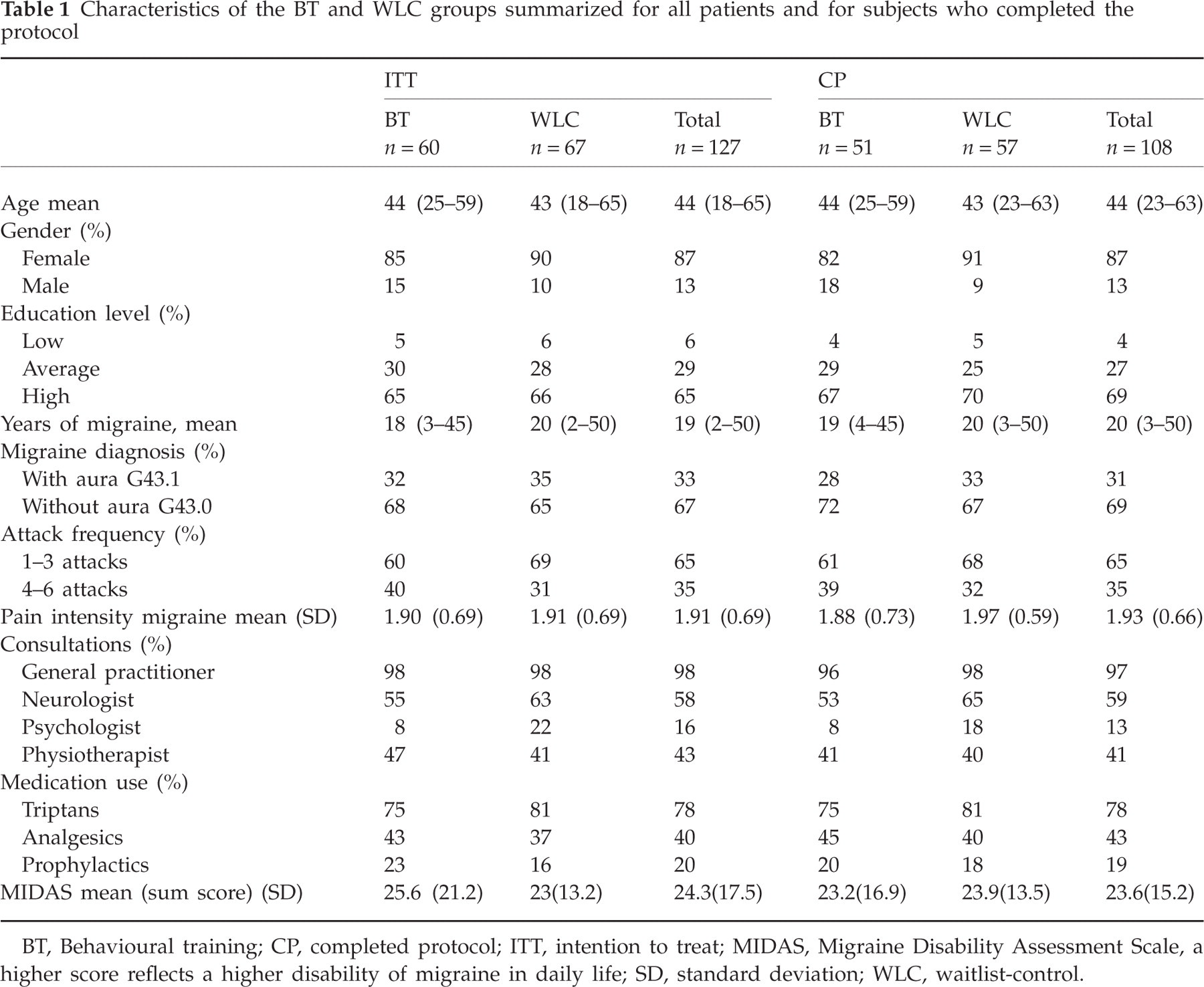
BT, Behavioural training; CP, completed protocol; ITT, intention to treat; MIDAS, Migraine Disability Assessment Scale, a higher score reflects a higher disability of migraine in daily life; SD, standard deviation; WLC, waitlist-control.
BT effects on primary outcomes
The results of the subjects who adhered to the training protocol are reported. Attack frequency was reduced in the BT group from 3.1 at baseline to 2.4 after training (−21%) per 4-week period. In the WLC group attack frequency changed from 3.1 to 2.9 (−6%). The overall effect size was small (−0.29) and a non-significant trend was found (P = 0.07) in the CP analysis. In the ITT analysis the difference was not significant. Patients' self-confidence in their own ability to prevent migraine attacks increased significantly and to a large extent (self-efficacy:effect size 0.79), which was also found regarding their belief that factors influencing the occurrence and relief of migraine attacks are under their own control (internal control:effect size 0.97). Patients' belief that migraine is a matter of chance or bad fate weakened significantly and to a medium extent (external control:effect size −0.73).
Figure 2 shows that 35% of the BT patients improved to a clinically significant extent, but 47% did not change and 18% responded adversely. In the waitlist condition, 19% of the patients were clinically changed, 60% did not change and 21% responded adversely. A non-significant trend was found when testing the clinical improvement of the BT group vs. the waitlist condition (P = 0.07). In the ITT analysis the difference was not significant.
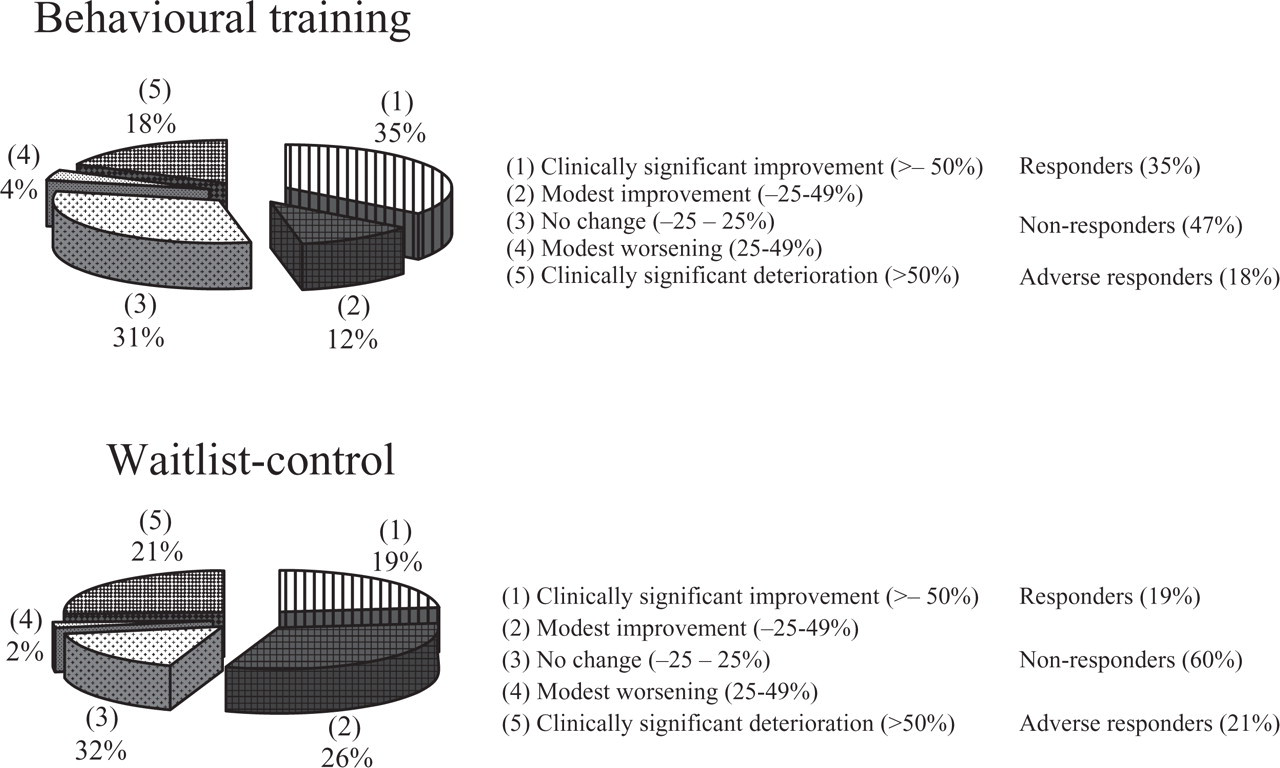
Treatment responder rate.
BT effects on secondary outcomes
Migraine-specific quality of life at baseline was similar in both groups and was not significantly changed post training (irrespective of the Bonferroni correction), indicating that BT did not affect patients' quality of life between attacks (Table 2). Immediate post-training differences in general physical and mental health status were unsubstantial, as were changes in migraine disability. Comparisons with the control condition yielded no between-group differences.
Between-group comparisons of changes in primary and secondary outcomes of subjects who completed protocol

Considered significant at P < 0.0125 after Bonferroni's correction.
Adjusted for baseline score (employed as covariate).
Square root transformation of scores.
Means pre and post, differences (Δ) in changes BT (behavioural training) vs. WLC (waitlist-control), 95% confidence intervals (CI) of Δ and standardized effect size (ES).
Migraine-specific QOL; a higher score reflects a higher quality of life between attacks.
Exploratory analyses
After the training the use of triptans decreased (from 3.8 to 3.5) and the use of analgesics increased (3.0 to 3.8). The waitlist condition also showed a decrease in triptan use (4.2 to 3.7) and an increase in analgesics use (3.7 to 4.1). Neither of these changes in acute medication use reached significance for the BT group. However, in the ITT analysis the increase in analgesic intake was significant (t =−2.12, P = 0.04). Analysis of the change in attack frequency of patients without prophylactic treatment showed a similar result to that of all patients.
BT participants with high attack frequency showed a reduction from 4.8 attacks to 3.0 post training (−37%), whereas the WLC group showed a reduction of 5.2 to 4.6 attacks (−12%). Patients with high attack frequency had significantly more benefit from BT than those with low attack frequency, whose attack frequency changed from 1.9 to 2.0 attacks post training (P = 0.03).
Discussion
In the present study lay trainers with migraine offered home-based behavioural training to small groups of fellow patients that was aimed at the non-pharmacological prevention of migraine attacks. The study could not confirm that BT would reduce migraine attack frequency immediately after training. This effect was modest (−21% for BT participants and −6% for controls), and only a non-significant trend was found in the completed protocol analysis (P = 0.07). This non-significant finding for the primary outcome variable is in line with a review of Larsson (2005) showing that self-help or school nurse-administered approaches were inferior to therapist-delivered relaxation in youngsters with chronic headache (54). However, the results confirmed the expectations that BT would increase patients' feelings of control over migraine attacks (effect size 0.97) and confidence in their own capacity to prevent or manage attacks (effect size 0.79). These effects remained significant after correction for multiple testing. No effects were found for quality of life or disability.
The exploratory analyses yielded indications that patients with a high frequency of attacks had significantly more benefit from BT than those with a low frequency. This finding must be considered with caution, because the subgroups were rather small. Further, according to the ITT analysis the use of analgesics increased significantly after BT. The CP analysis also indicated that the use of analgesics increased, whereas the use of triptans decreased. This was observed in both conditions, but these findings remain inconclusive, as they were all non-significant. The use of prophylactics has been reported as a contraindication for behavioural treatment (53). This was not confirmed by the present study, since restricting the analysis to patients who did not use prophylactics did not affect the effect of BT on attack frequency.
Four aspects of the present study are discussed below, regarding the severity of the migraine problem in the present sample, the choice of the WLC condition, the employment of lay trainers with migraine and the importance of follow-up results. First, it is evident that the present results were obtained in a patient group characterized by relatively severe migraine and relatively impaired quality of life. The participants were under medical care for migraine, 11% had joined the patient organization (45), and migraine-related disability was high compared with an international population study (47). Second, a WLC group was used instead of a placebo-control group. Although we had good reason for it, use of a placebo-intervention could have produced improvement comparable to the present BT outcome (6, 28). Therefore, had we performed a placebo-controlled study the conclusions on attack frequency would have been the same.
Third, as regards the employment of lay trainers with migraine, our pilot study has shown that the present trainers sometimes suffered from fatigue or migraine themselves during the session and thus had to struggle to manage their own migraine (16). Other problems included leading a group and balancing attention, and difficulties in providing individualized feedback. Individualization, the tailoring of attention and findings to the individual case, has been shown to be an effective quality of peer educators in health education programmes (55). It might be more difficult and demanding to realize individualization successfully within a behavioural training programme than in a health educational programme, and the present BT application drew heavily on this ability of the trainer. However, none of the lay trainers with migraine dropped out of the present study and, despite the difficulty of the task, being a trainer was experienced as rewarding. Nevertheless, the question remains whether the task of training fellow patients is too demanding, given the complexity of BT and the presentation to a group. This issue remains unresolved, for two reasons. Since the effect of BT provided by healthcare professionals was established on the basis of individual treatment, future research needs to establish whether lay trainers with migraine might be successful with individual provision of BT (instead of a BT group application). Also, one could consider devoting more extensive care to the specific handling of individualization in preparing and supervising lay trainers with migraine who provide BT. This is a challenging question, especially given our present investment in training and supervision of patient trainers and the costs involved in increasing this investment.
Lastly, it might be too ambitious to aim for a significant decrease in attack frequency immediately after the present BT. The participants may still be in the process of learning to adapt their life-style at the end of BT. The significant increase in subjective control and confidence in attack prevention may reflect an increased ability of the participants to predict attack occurrence. This may also indicate that the anxiety of the migraine attack lessened, while its acceptance increased (56, 57). Longer-term effects of BT are therefore also of interest.
In conclusion, we have found that home-based behavioural training provided by lay trainers with migraine to small groups of fellow patients produced a minor (−21%) short-term effect on attack frequency and clinically significant improvement in 35% of the participants. Covariance analysis showed a non-significant trend (P = 0.07) compared with the WLC condition. In addition, BT convincingly strengthened perceived control over migraine and self-confidence in attack prevention. Last, BT did not alter quality of life or migraine-related disability. Follow-up data can show whether these effects are maintained or may improve over time.
Footnotes
Acknowledgements
The project was supported by grant no. 940-31-069 from the Netherlands Organization for Health Research and Development (ZonMw), The Hague and financial means provided by the Pain Expertise Centre Rotterdam. The authors thank the Dutch Society of Headache Patients, in particular M. van den Berg, PhD, P. B. Vriezen, ir, J. Kooi, ir, and A. Mensing for their cooperation. The neurologists J. L. van der Zwan and L. J. M. M. Mulder are thanked for the consultations provided to clinically support the migraine diagnoses of participants in the present study. A. Spuij, BA, supported the logistics of the study as research assistant. H. J. Duivenvoorden, PhD