
Abstract
Background
Behavioral migraine approaches are effective in reducing headache attacks. Availability of treatment might be increased by using migraine patients as trainers. Therefore, Mérelle and colleagues developed and evaluated a home-based behavioral management training (BMT) by lay trainers (1). The maintenance of effects at long-term follow-up is studied in the present study.
Method
Measurements were taken pre-BMT (T0), post-BMT (T1), at six-month follow-up (T2), and at long-term follow-up, i.e. two to four years after BMT (T3). Data of 127 participants were analyzed with longitudinal multi-level analyses.
Results
Short-term improvements in attack frequency and self-efficacy post-BMT were maintained at long-term follow-up (dT0–T3 = −.34 and dT0–T3 = .69, respectively). The level of internal control that increased during BMT decreased from post-BMT to long-term follow-up (dT0–T3 = .18). Quality of life and migraine-related disability improved gradually over time (dT0–T3 = .45 and dT0–T3 = −.26, respectively).
Conclusions
Although the results should be interpreted with caution because of the lack of a follow-up control group and the inability to gather information about additional treatments patients may have received during the follow-up period, the findings suggest that lay BMT for migraine may be beneficial over the long term. If so, this could make migraine treatments more widely available.
Introduction
Migraine is a chronic neurovascular disease that is characterized by severe headache attacks (2,3). Therefore, migraine interferes with work activities and social life (4,5). Since the 1970s behavioral migraine interventions have been developed (6). These interventions are targeted at increasing participants’ perceived control over migraine, reducing the frequency and intensity of headache attacks, and decreasing migraine-related disability (7). Behavioral migraine approaches, such as relaxation training and cognitive-behavioral techniques, are effective in reducing headache attacks (6,8–10). Minimal contact versions of these approaches have proven to be equally effective as vis-à-vis treatments (11,12). An important advantage of minimal contact approaches is increased availability of therapy (11,13–15). Availability might even be more increased by using migraine patients as trainers. Additionally, lay trainers may decrease drop-out by being more motivating (16). For these reasons Mérelle and colleagues developed and evaluated a home-based behavioral management training (BMT) delivered by migraine lay trainers (MLTs) (17). BMT was primarily aimed at reducing the migraine attack frequency and increasing internal control over and self-efficacy in attack prevention.
The short-term efficacy of BMT was examined in a randomized controlled trial (1). The results showed that participants in the treatment group experienced 21% less migraine attacks immediately after the training. Migraine patients in the waitlist control (WLC) group experienced 6% less attacks. The difference between the treatment group and the WLC group did not reach significance (p = .07). However, participants in the treatment group did report significantly more self-efficacy in managing headache episodes and headache-specific internal control than participants in the WLC group. Moreover, effect sizes were large. No differences were found for quality of life and migraine-related disability. The WLC group received BMT directly after their waitlist period. In a six-month follow-up study, Mérelle and colleagues found that attack frequency in the total group of participants significantly decreased from post-BMT to six-month follow-up (−23%). Post-BMT improvements in headache-specific internal control and self-efficacy in managing headache episodes were maintained (18). Furthermore, quality of life improved from pre-BMT to six-month follow-up. These improvements cannot be explained by changes in medication use.
To our knowledge no long-term follow-up studies on BMT delivered by migraine patients have been conducted yet. Therefore, the primary aim of the present study was to study whether the changes in migraine frequency, self-efficacy in managing headache episodes, and headache-specific internal control were maintained or improved from post-BMT to two to four years after BMT. The secondary aim of the present study was to study whether the change in quality of life was maintained or improved. Furthermore, we evaluated whether any changes occurred over time in migraine-specific disability.
Materials and methods
Participants
At the time of inclusion (1), participants’ age ranged from 18 to 66 years old (mean (M) age = 44). All patients met the International Headache Society criteria (19) for migraine with (G43.1) or without (G43.0) aura. Headache attack frequency had to be between one and six attacks per month. Exclusion criteria were a headache frequency of 15 days or more per month, migraine duration of less than a year, a score of 178 or higher on the Symptom Checklist-90 (SCL-90) (20), and migraine onset above age 50. Migraine onset at an older age can be indicative of an underlying organic disease. The major reason to set up this study was an optimal applicability of behavioral strategies. Therefore, we did not restrict the study to ideal participants with two to four attacks per month. Instead, we chose a broad range of patients that allowed us to generalize the findings to the general population and could enhance the external validity of the study. We chose to exclude high frequency to minimize the risk of including patients with medication-overuse headache.
BMT
The BMT protocol was based on an established protocol for individual behavioral treatment (21–23). The two main strategies used to prevent migraine attacks were: 1) Detecting migraine triggers and premonitory symptoms (using registration assignments) and 2) Using skills for preventive self-regulation, including autogenic relaxation, diaphragmatic breathing, cue-controlled self-relaxation, positive thinking, and time-management. Treatment consisted of seven small-group (three to four migraine patients) sessions at the trainer’s home. The sessions had a duration of two hours each and were provided within a period of ten weeks. Sessions 1 to 3 took place once per week and focused on the acquisition of self-management skills regarding the early detection of triggers and premonitory symptoms and a stepwise training in self-relaxation. Sessions 4 to 6 took place every two weeks and focused on the application of these skills in daily life and in migraine-provoking conditions. In addition, participants developed a personalized action plan with lifestyle changes and self-regulation skills to be executed in case of a risk condition. The last session was used for evaluation and relapse prevention. In between the group meetings participants had to read some theoretical background information, to perform their autogenic and breathing exercises, and to complete their registration assignments.
Migraine lay trainers (MLTs)
MLTs received BMT themselves before becoming a trainer (17). Participants who were able to manage their own migraine attacks and were motivated to become a trainer provided BMT to one new patient under supervision of the third author. Next, the potential MLTs trained a small group of new patients under continued supervision. MLTs received an elaborate manual for every BMT session. MLTs briefly evaluated every session on a standard evaluation form, which was used for supervision after sessions 1, 3 and 6. Finally, MLTs participated in three workshops on trainer skills and a workshop on relaxation training. MLTs were paid a limited fee of 20 euros per BMT session, which also covered expenses of the BMT provision at their homes.
Measures
Headache diary
Migraine frequency was measured with a prospective headache diary. The use of a headache diary is in accordance with the guidelines for clinical trials in prophylactic treatment and the guidelines for behavioral trials (9,24). Participants recorded their headaches for four weeks per 24 hours. In case of a migraine attack pain intensity was rated per six-hour unit and was scored on a three-point scale: 1 (mild headache—I can do everything but with some difficulty), 2 (moderate headache—I cannot do all or most things) and 3 (severe headache—I am unable to do things, bed rest is necessary). Participants were asked to register additional characteristics and associated symptoms once a day. The data from the headache diary were prepared in the same way as in the study by Mérelle and colleagues (1).
Headache Management Self-Efficacy Questionnaire (HMSE)
To assess participants’ self-efficacy in managing headache episodes, the HMSE (25) was used. The HMSE consists of 25 items. All items are evaluated on a seven-point scale (from 1 = strongly disagree to 7 = strongly agree). A total score (ranging from 25 to 175) has been calculated by summing all the items. A higher score indicates a higher level of self-efficacy. Mérelle and colleagues translated the HMSE into Dutch and found its reliability to be satisfactory (1).
Headache-Specific Locus of Control Scale (HSLC)
The HSLC (26) was used to measure perceived control over migraine attacks. The HSLC consists of 33 items and three subscales: internal locus of control (11 items), external control chance (11 items) and health care professional locus of control (11 items). The health care professional locus of control scale was not used in this study. Every item is scored on a five-point scale (from 1 = strongly disagree to 5 = strongly agree). For the HSLC the subscale scores were calculated (ranging from 11 to 55). The psychometric abilities of the HSLC are satisfactory (27). Mérelle and colleagues translated the HSLC into Dutch. This Dutch version yielded good to excellent reliability (1).
Migraine-Specific Quality of Life Questionnaire (MSQOL)
The quality of life of the participants was measured by the Dutch version of the MSQOL (5,28,29). The MSQOL consists of 20 items, each of which is scored on a four-point scale. Scores can vary from 20 to 80, with lower scores indicating a lower quality of life. The Dutch version of the MSQOL has a good reliability and validity (5).
Migraine Disability Assessment Scale (MIDAS)
The MIDAS (24) was used to asses disability related to migraine attacks in migraine patients. The total score reflects the number of days lost during the past three months because of migraine in different settings (e.g. at work or at home). The reliability and validity of the MIDAS are acceptable (24).
Study design and procedure
The present study is a follow-up study (i.e. two to four years after BMT) of the randomized controlled trial Mérelle and colleagues performed between July 2003 and March 2007 (1,18). All participants of the original study (17) were invited to take part in this long-term follow-up study. Participants were informed about the follow-up study by an information letter, which was sent in November 2007 (two to four years post-BMT). This letter was sent by post, together with the headache diary and questionnaires. The study was approved by the ethics committee of the Erasmus MC, Rotterdam, The Netherlands.
As the WLC group received BMT directly after the waiting period, we added their data to those of the original BMT group.
Data analysis
Multi-level modelling (SPSS 17, MIXED module) was applied for longitudinal analysis. This analysis allows handling incomplete data with a minimal loss of information, as incomplete cases can be included in the analyses. Results of the measurements pre-BMT (T0), post-BMT (T1, 10 weeks), at six-month follow-up (T2), and at long-term follow-up (circa three years) are presented. Linear splines were used to test the differences in outcomes between time points (30). In addition to a linear time effect, knots were postulated at post-BMT (10 weeks) and at six-month follow-up (26 weeks), thereby respecting the differences in time span between the follow-ups. This procedure allows the estimated course of the dependent variable to bend at the intermediate time points (post-BMT and six-months follow-up). Non-significant knots (p out > 0.05) were deleted from the models until a final parsimonious model was reached that did not differ significantly from the original saturated model. This significance was determined with the deviance statistic (31). Migraine-related disability was log-transformed; other dependent variables were root-transformed because they were not normally distributed. There was no transformation needed for the HSLC subscale for external control chance (subscale HSLC). For all differences effect sizes are reported, with d = .2 indicating a weak effect, d = .5 indicating a medium effect and d = .8 indicating a strong effect (32).
Results
Patient characteristics
Demographic, psychological and migraine characteristics at baseline for all patients and drop-outs at long-term follow-up.

M: mean; SD: standard deviation. aIndependent-samples t-test, unless otherwise indicated. bFisher’s exact test. cChi square test.
Changes in primary outcomes
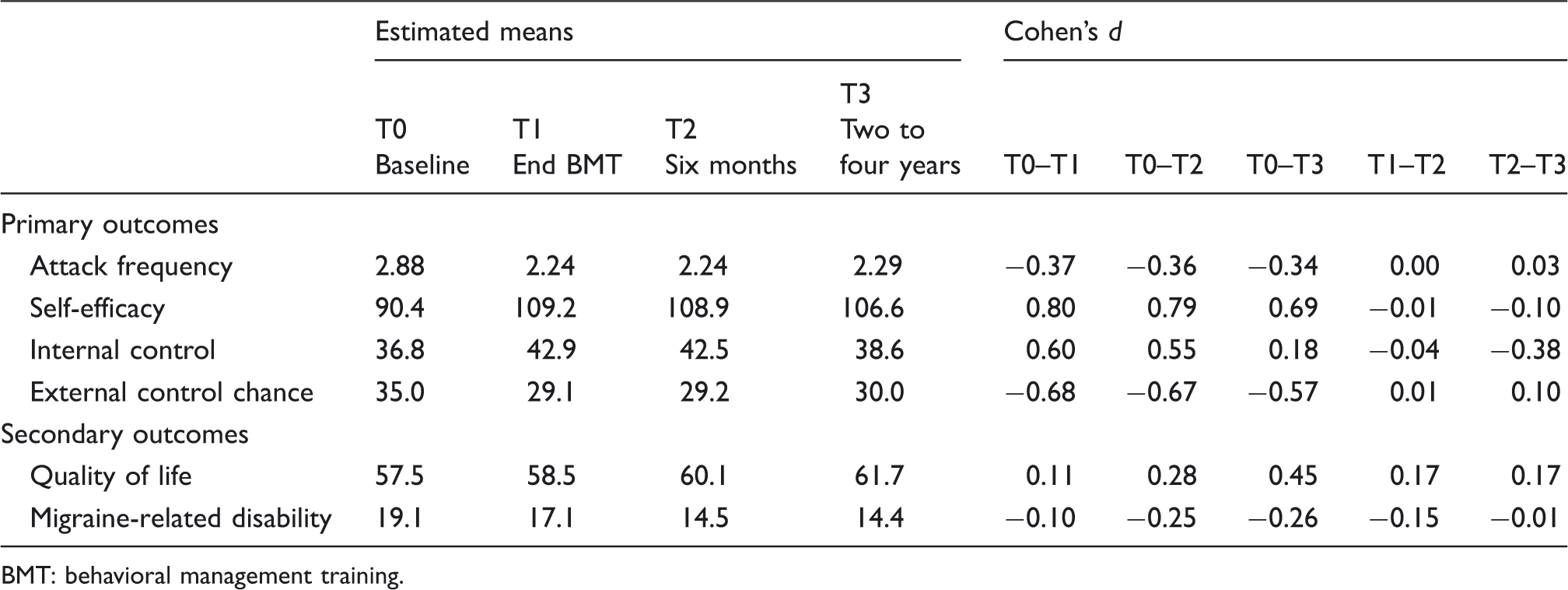
Attack frequency and self-efficacy in managing headache episodes improved from pre-BMT to post-BMT (dT0–T1 = −.37 and dT0–T1 = .80) and were maintained at six-month follow-up (dT0–T2 = −.36 and dT0–T2 = .79) and long-term follow-up (dT0–T3 = −.34 and dT0–T3 = .69). The level of perceived headache-specific internal control over migraine attacks increased during BMT (dT0–T1 = .60), but decreased from six-month follow-up to long-term follow-up (dT2–T3 = −.38). The gain in perceived headache-specific internal control between pre-BMT and long-term follow-up was nearly significant (dT0–T3 = .18, p = 0.059; not in table). External control chance decreased during BMT (dT0–T1 = −.68) and was maintained at long-term follow-up (dT0–T3 = −.57). Details about the mixed models and their regression weights are presented in Table 2. Estimated means, standard deviations, effect sizes, and p values are presented in Table 3. Graphic displays of the results are presented in Figure 1.
Graphic representation of effect sizes of primary and secondary outcomes. Parsimonious mixed models of transformed primary and secondary outcomes. df: degrees of freedom; T1: post-behavioral management training at 10 weeks; T2: six-month follow-up. a–2 log likelihood difference between complete and final model. Estimated means and effect sizes of primary and secondary outcomes. BMT: behavioral management training.

Changes in secondary outcomes
Quality of life improved from pre-BMT to long-term follow-up (dT0–T3 = .45). Migraine-related disability also improved gradually over time (dT0–T3 = −.26). Estimated means, standard deviations, effect sizes, and p values are presented in Table 3. Details about the mixed models and their regression weights are presented in Table 2. Graphic displays of the results are presented in Figure 1.
Discussion and conclusions
The findings of this follow-up study seem promising. Most positive short-term changes in migraine-related outcomes were maintained at long-term follow-up, i.e. two to four years after BMT. The short-term improvements in attack frequency and self-efficacy in managing headache episodes post-BMT were maintained at six-month follow-up and at long-term follow-up. Quality of life and migraine-related disability improved in the period from pre-BMT to long-term follow-up. Only headache-specific internal control decreased from post-BMT to long-term follow-up.
Results found at post-BMT and six-month follow-up slightly differ from the results found by Mérelle and colleagues (18). Mérelle and colleagues did not find any decreases in migraine-related disability (18) whereas in the present study migraine-related disability significantly decreased during BMT and at six-month follow-up and was maintained at the last follow-up. This difference in results has been caused by the use of different analyzing techniques, i.e. repeated-measurements analysis of variance (ANOVA) versus longitudinal multi-level analysis. With repeated-measurements ANOVA only complete cases are analyzed, whereas with longitudinal multi-level analysis all available data are analyzed.
It is an interesting finding that headache-specific internal control returned toward its original level, while the decrease in external control chance was mostly maintained at long-term follow-up. These results support the notion that internal control and external control are independent constructs instead of being opposite ends of one continuum (33). Someone can have internal and external beliefs at the same time. Furthermore, previous research suggests that internal control is not always associated with better health outcomes than external locus of control. It is also remarkable that headache-specific internal control decreased at follow-up, while the short-term increase in self-efficacy in managing headaches was maintained at follow-up. Self-efficacy refers to the confidence in one’s ability to use specific behavioral strategies to prevent and manage migraine attacks (25). The results might thus imply that three to four years after treatment participants are still confident that they are able to perform the self-management behavior that they learned during treatment (i.e. self-efficacy), but that they feel less optimistic about the overall degree in which migraines can be influenced by their own actions (i.e. internal control; see Seng and Holroyd (34)).
The strength of the present follow-up study is the length of the follow-up period. Research has shown that traditional vis-à-vis behavioral therapies are effective in the long term (35). To the best of our knowledge no study has examined the maintenance of effects of a behavioral management training provided by migraine patients at two to four years’ follow-up. Another strong methodological point is that longitudinal multi-level analysis is used to analyze the data. Longitudinal multi-level analysis is less biased than repeated-measurements ANOVA, for all participants of the original study are taken into account, including participants who dropped out at follow-up.
The most important limitation of the present study is that there was no control group anymore at follow-up, as withholding treatment to the WLC group was judged to be unethical. Therefore, we could not rule out that spontaneous recovery (or regression to the mean) partly accounts for the findings, taking into account that migraine usually decreases with aging (36). Also, we were unable to continue monitoring medication use during follow-up and cannot rule out effects due to medication changes. Furthermore, as in our initial investigations (1,18), we did not assess whether patients still used the behavioral and cognitive strategies they were taught during the BMT intervention.
Another important limitation is that the follow-up time was not the same for all participants. Some participants filled out the questionnaires two years after BMT, others filled out the questionnaires four years after BMT. Furthermore, the level of headache-specific internal control and quality of life significantly differed for patients who did and patients who did not participate in the long-term follow-up study. Drop-outs who did not remain in the study had less headache-specific internal control and a higher quality of life at baseline. These differences have resulted in slightly different short-time results reported by Mérelle et al. (17), who had conducted complete cases analyses. Given these concerns, it is important to interpret the present findings with caution.
In conclusion, BMT seems to improve the self-management skills of migraine patients, even at long-term follow-up. If the cost-effectiveness has been proven, BMT by lay trainers could be implemented on a large scale. This would make treatment for migraine patients more available. However, problems with finding suitable lay trainers may be a threat to large-scale implementation (17,18). Our results suggest that self-efficacy is an important component of self-management. Therefore, newly developed therapies for patients with migraine should include strategies to enhance self-efficacy. Future research should compare BMT delivered by lay trainers and BMT delivered by a professional. Additionally, it will be interesting to know if booster interventions using, for example, Internet or text messages intensify the long-term benefits of BMT. Also, future follow-up studies should include qualitative interviews to find out if migraine patients who have participated in BMT keep using learned strategies.
Clinical implications
It is known that behavioral therapy is effective in reducing migraine attacks. Additionally, minimal-contact versions of these approaches have proven to be equally effective and five times more cost effective than vis-à-vis treatments. Few therapies given by lay trainers have been developed. To our knowledge no long-term follow-up studies on this topic have been conducted yet. By using migraine patients as lay trainers, treatment availability might be increased.
Footnotes
Acknowledgments
The authors thank the participants and the Dutch Society of Headache Patients for making this study possible.
Funding
This research received no specific grant from any funding agency in the public, commercial, or not-for-profit sectors.
Conflict of interest
None declared.