
Abstract
The aim of this study was to assess the efficacy of non-pharmacological prophylactic treatments of migraine in children. Databases were searched from inception to June 2004 and references were checked. We selected controlled trials reporting the effects of non-pharmacological prophylactic treatments in children with migraine. We assessed trial quality using the Delphi list and extracted data. Analyses were carried out according to type of intervention. A total of 19 trials were included. Relaxation, relaxation + biofeedback, relaxation + biofeedback + cognitive behavioural treatment were more effective compared with waiting list controls. Relaxation + behavioural therapy was more effective than placebo. There is conflicting evidence for the use of oligoantigenic diets. A few non-pharmacological treatments such as relaxation may be effective as prophylactic treatment for migraine in children. Because of the small number of studies and the methodological shortcomings, conclusions on effectiveness have to be drawn with caution.
Introduction
Migraine is an important clinical problem in school-age children with a prevalence of 2.7% to 11% (1). It is characterized by attacks of intense, throbbing, unilateral headache, often accompanied by nausea, vomiting, photophobia and phonophobia (2, 3).
Treatment of paediatric migraine includes an individually tailored regimen of both pharmacological and non-pharmacological measures. Pharmacological interventions include the use of symptomatic medication such as analgesics, and the use of prophylactic medication. The non-pharmacological modalities include life-style adjustments (e.g. dietary adjustment), reassurance, stress management, biofeedback and other behavioural therapies.
High-quality controlled trials preferably summarized in a systematic review form the basis for evidence-based treatment guidelines. One review is available evaluating amongst others 17 behavioural treatment studies of migraine in children, concluding that thermal biofeedback and biofeedback plus progressive muscle relaxation seem more effective than other behavioural, psychological or drug treatments (4). The authors included also studies without a control group and excluded 35% of the behavioural treatment studies, which they considered to be methodologically inadequate or lacking statistical information. In a recent Cochrane review (5), a summary is made concerning psychological therapies in the management of chronic and recurrent pain in children and adolescents. Unfortunately, the authors did not specify their findings by type of headache and age.
The present systematic review distinguishes itself from these reviews by evaluating the literature systematically using up-to-date methodology recommended by the Cochrane Collaboration (6), reporting according to the Quality Of Reporting Of Meta-analyses (QUOROM) statement and by including the most recent literature up to June 2004. In this article, the authors present a systematic review of controlled trials concerning the efficacy of non-pharmacological prophylactic treatments of migraine in children. The authors have also reviewed the results of pharmacological prophylactic treatments. This is the subject of a separate article (Part 2).
Methods
Search strategy
MEDLINE, EMBASE, PsycINFO, Web of Science and Cinahl were searched from inception to June 2004 using the terms ‘migraine’, ‘headache’, ‘cephalgia’, ‘cephalalgia’, ‘child∗’, ‘infant’, ‘teenage’, ‘adolescent’ or ‘p(a)ediatric’ together with the search strategy for identifying randomized (RCT) and clinical controlled trials (CCT) described by Robinson and Dickerson (7). The Cochrane Controlled Trials Register, Cochrane Library, issue 2, 2004, was searched using the words ‘migraine’, ‘headache’, ‘cephalgia’, ‘cephalalgia’, ‘child∗’, ‘infant’, ‘teenage’, ‘adolescent’ or ‘p(a)ediatric’. Additional strategies for identifying trials included searching the reference lists of review articles and included studies.
Study selection
Only RCTs and CCTs including non-pharmacological prophylactic interventions used in the treatment or management of migraine in children (age < 18 years), with criteria designed to distinguish migraine from other types of headache, were selected. The use of a specific set of diagnostic criteria (e.g. IHS 1988) (3, 8) was not required, but migraine diagnoses had to be based on at least some of the distinctive features of migraine, e.g. headache attack lasts 2–48 h, unilateral location, pulsating quality, moderate to severe intensity, aggravation by routine physical activity, nausea and/or vomiting, photophobia and phonophobia. Studies with at least one of the following headache outcome measures were included: intensity, frequency, duration, headache or improvement. No language restriction was applied.
Two authors (L.D., J.B.) independently screened titles and abstracts of studies identified by the literature search for eligibility. Potentially relevant studies were retrieved as full papers and again independently reviewed by two authors (L.D., J.B.). Disagreements regarding the inclusion were resolved through consensus, or by arbitration of a third author (A.P.V.).
Methodological quality and data extraction
Two authors (L.D. and J.B. or A.P.V.) independently assessed the methodological quality of the included trials using the Delphi list (9). The Delphi list is a generic criteria list developed by international consensus and consists of the following nine items: (i) randomization; (ii) adequate allocation concealment; (iii) groups similar at baseline; (iv) specification of eligibility criteria; (v) blinding of outcome assessor; (vi) blinding of care provider; (vii) blinding of patient; (viii) presentation of point estimates and measures of variability; (ix) intention-to-treat analysis; and one extra item was added: (x) withdrawal/dropout rate (>20% or selective dropout) unlikely to cause bias. This item was added because it was found relevant for these studies. All selected methodological criteria were scored as yes (= 1), no (= 0) or don’t know (= 0). A quality score was computed by counting the number of positive scores, with equal weights applied on all items. In case of a disagreement, consensus was used to resolve disagreement. When consensus could not be reached, a third author made the final decision (J.B. or A.P.V.).
Extraction of data from the original reports was performed by one author (L.D.) and checked by a second (A.P.V.). Disagreements were resolved by consensus. Extracted information included (if available) demographic data, detailed description of the intervention and control (i.e. dose given, study duration), outcome measures and information on adverse effects.
Data analysis
We calculated standard mean differences (SMD) with 95% confidence interval (CI) for continuous outcomes or relative risks (RR) with 95% CI in case of dichotomous variables. RR > 1 and a SMD > 0 represent a better outcome for the first mentioned intervention group. For all data we include data only on those whose results are known (available case analysis).
In case of a cross-over trial ideally we would like to restrict our analysis to first period data only, or, in case of a sufficient wash-out period and no carry-over effect, data of both periods could be combined. In this review we analysed the cross-over trials as if they were parallel-group trials, because none of them provided separate data of each treatment period or data concerning the existence of a carry-over effect.
If relevant data were available, and studies were found clinically homogeneous, a quantitative analysis (statistical pooling) was performed. In other cases, a qualitative analysis was performed using a rating system with levels of evidence (10). The evidence was judged to be strong when multiple (two or more) high quality RCTs produced generally consistent findings. Results were considered consistent if 75% or more of the studies reported similar results on the same outcome measure. It was judged to be moderate when one high-quality RCT and/or multiple (two or more) low-quality RCTs and/or CCTs produced generally consistent findings. Evidence was considered to be limited when only one low-quality RCT and/or CCT existed and conflicting if the findings of existing trials were inconsistent. No evidence was considered when no RCTs or CCTs were found or when the authors provided no sufficient data for analysis. We regarded trials with methodological quality scores of ≥6 as of high quality (10).
Results
Search results
A total of 3492 publications were identified by our broad and sensitive search strategy (see Fig. 1). Finally, a total of 19 studies were included in this review.
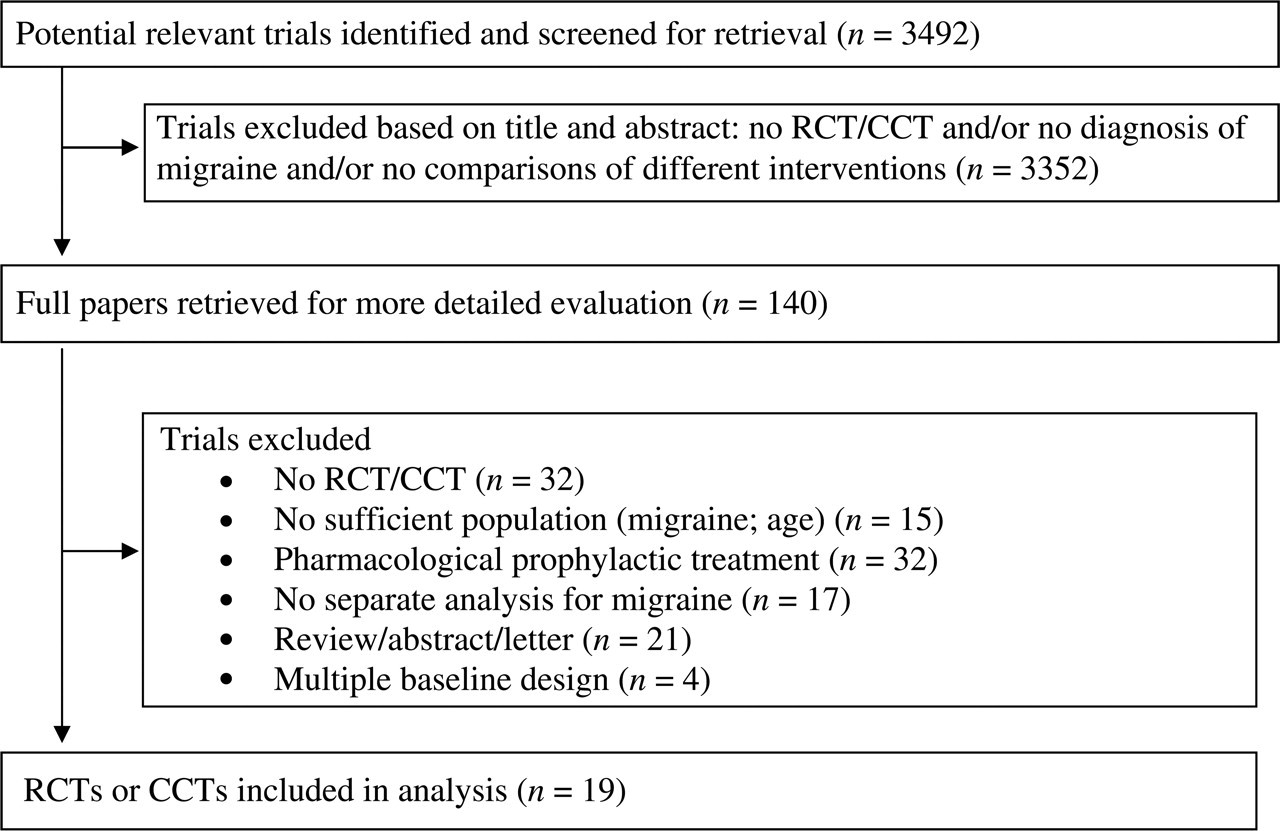
Quorum statement flow diagram.
Description of studies
Full details of the included studies are presented in Table 1.
Study characteristics of included studies




RCT, randomized controlled trial; CCT, controlled clinical trial; PG, parallel group; CO, cross-over; C, control 1; I, intervention; HA, headache; IHS, International Headache Society 1988; QS, quality score on Delphi list with positive items in parentheses; N, number of subjects in the trial; RR, relative risk with 95% confidence interval; SD, standard deviation; SMD, standard mean difference with 95% confidence interval; EMG, electromyography.
Participants
The number of included participants in each trial ranged from 17 to 136 (mean 44 ± 29 patients), with a total of 834 patients included. Most studies were small; out of 44 study groups, 29 (66%) included not more than 15 subjects and only one study included over 30 subjects in each of the three study groups. The mean percentage of participants who dropped out was 11.4% (range 0–36.1%). The mean age of participants was 11.7 ± 1.6 years (range 3–18 years). Overall, the percentage of girls was generally the same as boys (mean 55.6%; range 20.0–75.6%). Seven trials used the criteria of the International Headache Society to classify migraine (see Table 1), one trial used the Ad Hoc Committee's criteria, while the remaining studies used varying definitions. Two studies used a cross-over design.
Interventions
The interventions used could be divided into behavioural treatments and life-style adjustments or acupuncture. For behavioural treatment comparisons were made between relaxation and placebo (11–13), biofeedback and placebo (11, 14–16), cognitive behavioural therapy (CBT) and placebo (13, 17). There were six studies with remaining comparisons (13, 18–21). For life-style adjustments comparisons were made between instructions to improve sleep hygiene and placebo (22), red and blue colour tint glasses (23), inclusion and exclusion of foods high in vasoactive amines (24), di- or oligoantigenic diet and placebo (25, 26), fish oil and olive oil (27), and acupuncture and placebo (28).
Outcome measures
All studies used headache (HA) diaries to assess outcomes. Using this diary amongst others, HA frequency, intensity and duration were scored on a Likert-scale. In most studies (14 out of 19) a measure of clinical improvement was calculated. In these studies an improvement was regarded as being clinically relevant when the patients’ headache declined by ≥50%. This score is presented as ‘HA improvement’ outcome in Table 1 and is our primary outcome measure. When this outcome measure was not available, we used headache measures (frequency, intensity or duration).
Methodological quality
The quality score (with positive items in parentheses) is presented in the ‘Study quality’ section of Table 1. The median score for methodological quality was 4 (range 2–7). Using a cut-off point of six out of 10 criteria, only two out of the 19 studies (10.5%) were considered to be of high quality (27, 28). The most prevalent methodological shortcomings were blinding of the care provider (unclear 100%), a concealed randomization method (unclear 79%, negative 16%) and blinding of both the patient and outcome assessor (both unclear 84%).
Effectiveness of non-pharmacological prophylactic treatment
Relaxation treatment
Three studies compared relaxation with placebo (attention) or a waiting list condition (11–13), of which two studies presented data (11, 13). HA improvement was significantly higher in the autogenic relaxation group compared with the waiting list condition (11). No significant differences in HA frequency were found between progressive relaxation and attention control (13). Both studies were small, with 10–15 people in each treatment group.
We conclude that there is limited evidence for an effect of relaxation compared with a waiting list condition, but no effect compared with placebo.
Biofeedback treatment
One small study compared thermal biofeedback with placebo (hand cooling) (16) and two small studies evaluated the additional effect of biofeedback on relaxation (11) or relaxation + behavioural management (14). In the pooled analysis no significant differences were found (see Table 2). Two small studies evaluated biofeedback compared with waiting list control and also did not find significant differences (15, 16). In one very small study clinical-based thermal biofeedback was compared with home-based thermal biofeedback and no significant differences were found (18).
Pooled results of non-pharmacological prophylactic treatment

BFB, biofeedback treatment; CBT, cognitive behavioural treatment; REL, relaxation therapy; HA, headache; L, low-quality trial; n, number of trials (which can have more than one comparison); RR, relative risk [95% confidence interval]
–, no data available.
We conclude that no clear effectiveness of biofeedback can be found.
Cognitive behavioural therapy
One small study compared cognitive coping with placebo (attention) (13), and one small study evaluated the effect of additional pain behavioural management to thermal biofeedback treatment (17). We found no significant differences post treatment, but inconsistent results at 3–4 months’ follow-up. Richter et al. (13) also compared CBT with progressive relaxation and found no significant differences.
We conclude that there is no clear effectiveness of CBT, and CBT compared with relaxation seems to be equally effective.
Combined behavioural treatments
Two small studies compared relaxation + thermal biofeedback with a waiting list condition (11, 19). In the pooled analysis relaxation + thermal biofeedback gave significantly more HA improvement compared with the waiting list condition (see Table 2). In one small study no significant difference was found between relaxation + CBT and the waiting list condition (14), but clinical or home-based relaxation + behavioural therapies are more effective in pain reduction than placebo (20). In one study clinical-based relaxation + CBT was compared with home-based relaxation + CBT (20) and relaxation + stress management was compared with metoprolol or cephalic vasomotor feedback plus stress management in another study (21). In both studies no significant differences were found concerning HA improvement. In two small studies of relaxation + CBT + biofeedback (thermal or EMG) significant HA improvement was found when compared with a waiting list condition (14, 22).
We conclude that there is moderate evidence for an effect of relaxation + thermal biofeedback compared with a waiting list condition, and limited evidence for an effect of relaxation + CBT compared with placebo and between several behavioural treatment modalities compared with a waiting list condition.
Other non-pharmacological prophylactic treatments
Concerning life-style adjustments vs. placebo, one study (23) evaluated instructions to follow guidelines towards improving sleep hygiene and found significantly lower HA frequencies when compared with children who were not instructed. The use of red colour tint or blue tint glasses seems to be equally effective (24).
Concerning dietary manipulations vs. placebo, one small study showed that the exclusion of foods with vasoactive amines in a diet rich in fibre did not influence HA improvement (25). Two studies, however, showed that oligoantigenic diets (i.e. diets modified to exclude, for example, milk, eggs, food additives and vasoactive amine-containing foods) are more effective than placebo (26, 27). One small high-quality study compared the use of fish oil with the use of placebo (olive) oil and found no significant differences in HA improvement, quality of life and well-being, cholesterol and triglyceride levels (28).
One very small study of high quality compared acupuncture with placebo acupuncture. Acupuncture gave significantly lower HA frequency compared with placebo (29).
We conclude that there is limited evidence for an effect of instructions to follow guidelines towards improving sleep hygiene, and conflicting evidence for oligoantigenic diets when compared with placebo.
Discussion
Based on the available literature, we found that relaxation treatment alone or in combination with biofeedback or CBT is more effective than a waiting list control, as well as relaxation + CBT compared with placebo (limited evidence). Other non-pharmacological prophylactic treatment modalities that are probably effective in children with migraine are acupuncture and instructions to follow guidelines towards improving sleep hygiene. Relaxation, thermal feedback or CBT were equally effective when compared with placebo, as well as relaxation compared with CBT. There is conflicting evidence from three studies for the use of oligoantigenic diets.
Although systematic reviews offer the least biased method of summarizing research literature, our results must be interpreted with consideration of the low power and the quality of evidence from which they were obtained. First, we decided not to contact the authors for additional information, because 16 of the 19 trials included in this review were published before 2000 and most authors would be difficult to find. Second, our inclusion criteria greatly reduced the number of studies selected. Several studies included patients with different headache types and provided no separate analysis for migraine (30–32). Positive results for the use of behavioural treatments in children and adolescents have frequently emerged from open-label or non-controlled studies (33, 34) or time-lagged design studies (35, 36). Third, the methodological shortcomings of many of the currently available studies limit conclusions about the effectiveness of non-pharmacological prophylactic treatments. These shortcomings include the lack of credible blinding (in those cases in which blinding was possible), an unclear randomization method, and most studies suffered from inadequate data representation and statistical analysis (intention-to-treat analysis). There is, however, a difficulty in blinding the care provider and patients during non-pharmacological prophylactic treatment of migraine. Finally, most treatments have only been evaluated in one or two studies with small numbers of patients (low power), which limits the generalizability of the findings.
We do not consider our conclusions to be influenced by not contacting original authors and our strict inclusion criteria, but our conclusions are certainly influenced by the wide variety of treatment modalities, the low power and methodological shortcomings of the studies found. Therefore, we strongly recommend performing large high-quality RCTs evaluating most frequently offered non-pharmacological prophylactic treatments, because at the moment no firm conclusions can be drawn based on the available literature.
There are several reasons why most studies did not show significant differences. First of all, there is the lack of power in most studies. In small studies possible clinically relevant differences cannot be found significant. Furthermore, it is difficult for any prophylactic treatment to show additional benefit taking the favourable natural course of childhood migraine into account. Lastly, the lack of significant results may be due to the outcome measure ‘HA improvement’, which was a main outcome measure in most studies. It indicated that only people with over 50% improvement are considered improved, which is a large improvement. The Philadelphia panel advises cut-off scores for clinically relevant differences in musculoskeletal diseases of 15% improvement (37). Perhaps other outcome measures (like quality of life and satisfaction of child and/or parents) or other cut-off scores between recovered and not recovered may be considered in future trials.
In conclusion, this review shows that there is a clear need of high-quality research evaluating non-pharmacological prophylactic treatment of children with migraine. Favourably high quality studies should be performed and reported according to the Consolidated Standards of Reporting of Trials (CONSORT) statement to improve the quality of trials reports. Headache improvement should be used as the primary outcome measure, but lower cut-off points for recovered and not recovered are recommended. Quality of life and satisfaction of child and/or parents should also be used as an outcome measure in studies involving non-pharmacological prophylactic treatment of children with migraine
Footnotes
Acknowledgements
The authors thank the Netherlands Organization for Health Research and Development (ZONMw) for funding this research.
Conflict of interest
None declared.