
Abstract
The SMILE study was conducted among migraine patients consulting in primary care in France. The first phase aimed to describe the study sample of patients at entry to the study, especially emotional dimension (Hospital Anxiety and Depression scale), functional impact (abridged Migraine Specific Questionnaire), stress (Perceived Stress Scale) and coping behaviours (brief COPE inventory avoidance subscale, Coping Strategies Questionnaire catastrophizing subscale), as well as treatments used and their effectiveness and treatments prescribed at end of consultation. Results indicate that consulting migraine patients suffer frequent migraine attacks, exhibit substantial levels of anxiety, functional impact and stress, and often use maladaptive coping strategies. Abortive treatments appear ineffective in most patients (74%). Patients with more affected psychometric variables and treatment ineffectiveness are more likely to be deemed eligible for prophylactic treatment. These data highlight the seriousness of migraine and maladjustment of patients consulting in primary care.
Introduction
About 20% of individuals in France suffer from migraine, but only one-fifth of them are medically followed up (1). Nevertheless, headache is one of the most common patient complaints to general practitioners (GPs) and neurologists. The population of migraine patients consulting may thus be somewhat different from those not consulting. Although several studies have described the general population of migraine patients in France (1–4), none was aimed specifically at describing the population of consulting migraine patients. However, a French community-based survey has compared the profile of consulting and non-consulting migraine sufferers and found that those consulting voiced more negative feelings of enduring the attacks and resignation. Thus, psychological factors may encourage migraine patients to seek medical assistance (4).
A number of studies have consistently shown evidence for comorbidity of migraine with psychiatric disorders, particularly anxiety and depression (5–8). A study conducted mainly in patients attending English migraine clinics has found approximately 50% and 20% of patients with anxiety and depression, respectively, according to the classical Hospital Anxiety and Depression (HAD) scale (9, 10). Similar proportions of anxious and depressed migraine patients (28% and 4%, respectively, plus 19% with both anxiety and depression) were observed in France in the general population using the same instrument (11). In contrast, a large population-based Norwegian survey has reported a notably low prevalence of migraine (12.3%), with only 9% of anxious and 5% of depressed migraine patients plus 6% having both anxiety and depression (12).
The first objective of the SMILE study was to obtain a detailed description at entry to the study of the clinical and psychometric profile (anxiety, depression, stress, coping strategies) of migraine patients attending general or neurological private practices in France. A second objective was to describe the treatments (acute and especially prophylactic treatments) used by and prescribed to consulting migraine patients and to analyse their effectiveness on migraine and anxiety at the time of entry, then prospectively 2 and 4 months after the consultation. A third objective was to compare physicians' perceptions of severity and impact of migraine and of affective symptoms in their patients with the perceptions reported by the patients themselves, and to examine the influence of physicians' perceptions on migraine medical management.
This study describes the overall methodology of the SMILE study, the characteristics of the physician and patient populations, and the treatments used and prescribed. Other results will be presented in forthcoming articles.
Methods
This was an office-based, prospective, observational study carried out in France among GPs and neurologists by the opinion poll institute THS Healthcare from November 2005 to July 2006. The study was declared to and approved by the French Commission on Data Processing and Liberties. No Ethics Committee approval of study protocol was required, as the study was only observational and had no impact on the medical management of migraine patients. Participating physicians received a fee as compensation for each patient inclusion, but patients received no compensation for participation.
Study physicians were recruited by mail or telephone from the total number of GPs and neurologists appearing in the database of physicians known to be habitual prescribers of migraine prophylactic medications. Of these, 1618 physicians (39.9% of all physicians recruited) agreed to participate.
Each participating physician was to include the first four consecutive patients consulting for migraine who were aged ≥ 18 years and not currently treated with a substance known to be endowed with migraine prophylactic properties (used either specifically for the prevention of migraine headaches or for other reasons). As this was an observational study, no other inclusion/exclusion criteria were used. However, the fact that the patients included were really migraine sufferers was ascertained a posteriori using the criteria defined in the International Classification of Headache Disorders, 2nd edn (ICHD-II) for migraine without aura (category 1.1) (13)—aura was not taken into account because of the risk of confusion with photophobia or other non-specific visual disorders.
A total of 6109 patients were included before March 2006. After exclusion of 329 patients for file incompleteness (no patient or physician questionnaire returned) and of 363 patients not satisfying inclusion criteria (age < 18 years, n = 4; blank patient questionnaire, n = 17; ongoing use of a prophylactic treatment, n = 218; non-migraine patients, n = 124), a total of 5417 patients included by 1550 physicians [1467 GPs (94.6%) and 83 neurologists (5.4%)] remained for analysis (Fig. 1). As this was an observational study, no analysis of patients not meeting inclusion criteria was performed.
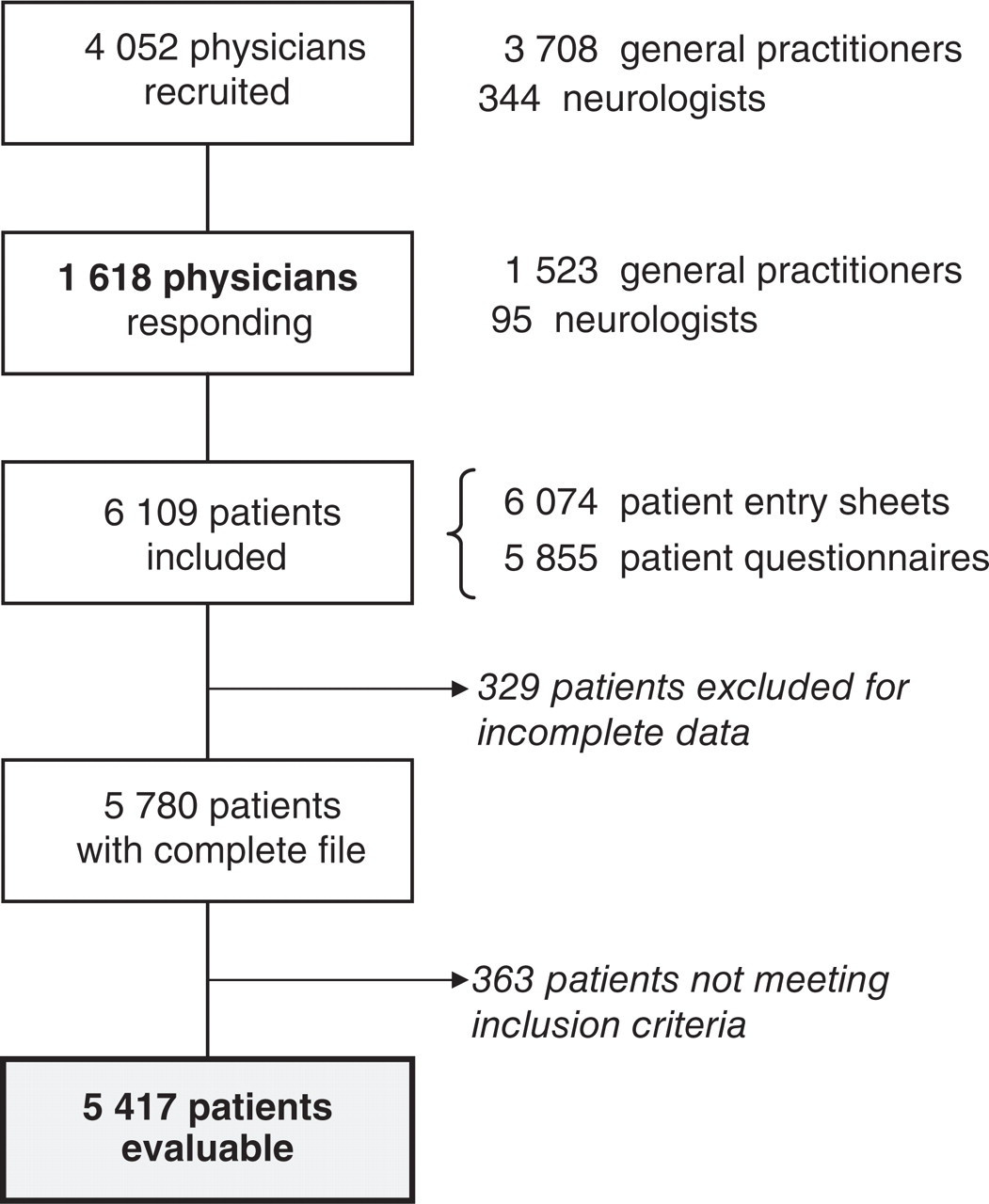
Patient selection phase of the SMILE study.
Study questionnaires
Four types of documents were to be completed, strictly independently, by the physician or the patient:
a 24-item physician questionnaire to be completed by the physician, which captured information about the physician's demography and professional activity, usual management of migraine, especially for patients with anxiety and/or stress;
a 20-item patient entry sheet, to be completed by the physician, enquiring about patient sociodemography, inclusion criteria, physician's perceptions about migraine severity (frequency and intensity of attacks), existence of anxiety or stress, estimated functional impact, usual treatment of migraine attacks and estimated patient satisfaction with the treatment, perceived medication overuse, patient eligibility for prophylactic treatment, proposition of initiation of a prophylactic treatment, final prescriptions at the end of the consultation, and possible influence of perceived anxiety or stress on the prescriptions;
a 50-item patient questionnaire, to be completed by the patient, which queried about patient sociodemography, ICHD-II diagnostic criteria for migraine without aura (13), migraine history, frequency of headaches, migraine impact on everyday life, affective symptoms, coping strategies, stress, acute treatment(s) of attacks, severity of treated attacks on a scale from 0 to 10, and acute treatment effectiveness; similar questionnaires, without description of migraine but with additional description of the treatments used since the consultation, especially prophylactic treatments, were to be completed 2 months and 4 months after the consultation and returned to the sponsor by mail;
a 4-month agenda of headaches (migraines or other headaches) with indication of the treatments taken for each migraine attack.
Psychometric tests
French versions of four psychometric scales were used to assess affective symptoms, migraine functional impact and coping behaviour:
anxiety and depression were measured using the HAD scale (10, 14); scores of ≥ 8 were retained for the characterization of both anxiety and depression, since these scores have been shown to be associated with high sensitivity and specificity for the detection of anxiety and depression in general practice (15, 16);
stress was assessed using the abridged form (PSS4) of the original Perceived Stress Scale questionnaire (17), which is the most widely used psychological instrument for measuring the perception of stress;
functional impact of migraine was assessed using an abridged version of the Migraine-Specific Quality of life (MSQ) questionnaire (18); the abridged form (MSQ4) was developed to allow easy use of the MSQ questionnaire in general practice (19);
maladaptive avoidance coping strategy was evaluated using the behavioural disengagement subscale of the brief version of the COPE inventory (20–22);
maladaptive pain coping strategy was evaluated using the catastrophizing subscale of the Coping Strategies Questionnaire (CSQ), which is a widely used measure of pain coping strategies (23, 24).
Evaluation of acute treatment effectiveness
Medications used for the acute treatment of migraine were classified either as specific (triptans, combination aspirin–metoclopramide, ergotamine derivatives) or non-specific [paracetamol, non-steroidal anti-inflammatory drugs (NSAIDs)], or as recommended (triptans, combination aspirin–metoclopramide, ergotamine derivatives, NSAIDs, aspirin) or not recommended (paracetamol, opioids). Acute treatment effectiveness was assessed using the set of four questions designed by the French Society for the Study of Migraine Headache (SFEMC). This questionnaire was designed to capture information about (i) significant migraine relief 2 h after drug intake; (ii) treatment tolerability; (iii) use of a single drug unit; and (iv) rapid resumption of normal social, family or professional activities (25). Patients who gave four ‘yes’ responses were considered to be using an effective treatment.
Data analysis
The percentages of patients with anxiety or depression were expressed by the relative proportions of patients exhibiting HAD anxiety or depression scores of ≥ 8 (both scales spanning the range 0–21). The PSS4 score was the sum of scores from 1 to 5 at the four items of the questionnaire (scale span 4–20). The MSQ4 score was the mean of scores from 0 to 100 at the four items of the questionnaire (scale span 0–100). The brief COPE avoidance score was the sum of scores from 1 to 4 at the two items of the questionnaire (scale span 2–8). The CSQ catastrophizing score was the sum of scores from 1 to 4 at the four items of the questionnaire (scale span 4–16).
Statistical analysis was essentially descriptive. Quantitative variables were described by the mean and standard deviation (SD). Categorical variables were described by the numbers and relative proportions in the relevant categories. Where appropriate, differences between groups were compared by Student's t-test (if the size of the groups to be compared was > 30) for quantitative data or by the Z-test for categorical data. Differences were considered significant or not significant (NS) at P < 0.05 or P > 0.05, respectively.
Results
The characteristics of the study samples of 1550 physicians and 5417 patients are presented in Tables 1 and 2, respectively.
Characteristics of the sample of study physicians

Indicates a significant difference vs. the national reference (P < 0.01).
SD, Standard deviation.
Characteristics of the sample of study patients

Indicates a significant difference between the groups of patients consulting GPs or neurologists (P < 0.01).
SD, Standard deviation.
Description of the sample of physicians
The study sample of GPs differed from the national reference by the men:women ratio (slightly higher for study GPs) and the number of GPs aged 30–39 years (slightly lower for study GPs). The sample of study neurologists differed from the national reference by the proportions working in Ile-de-France and South-East of France (slightly lower and greater, respectively, for study neurologists) (Table 1). Overall, the study populations of participating GPs and neurologists were close to the corresponding national populations of physicians.
Most study physicians were aware that many migraine patients suffer from anxiety (GPs, 81%; neurologists, 64%; P < 0.01) and that stress is a trigger factor of migraine attacks (GPs, 90%; neurologists, 92%; NS), and most of them (97% of study GPs and neurologists) agreed that anxiety and stress may promote medication overuse. More than half of the physicians (GPs, 58%; neurologists, 63%; NS) stated that the existence of anxiety and/or stress guided them on the choice of the prescribed therapy (acute or prophylactic treatment of migraine, anxiolytic treatment).
Nearly all study physicians stated that they used to prescribe prophylactic treatments (99% of GPs; 100% of neurologists), mainly to patients with frequent migraine attacks. They estimated at 34.1 ± 24.7% (GPs, 33.0 ± 24.1%; neurologists, 54.1 ± 27.2%; P < 0.01) the proportion of their patients who were treated with a prophylactic drug.
Description of the sample of patients
The sample of study patients consisted of 4329 women and 1088 men (80% and 20%, respectively), of whom 5169 (95%) consulted a GP and 248 (5%) a neurologist. The mean patient age was 41.4 ± 12.4 years (minimum 18 years; maximum 88 years; women, 41.3 ± 12.3 years; men, 42.0 ± 12.4 years; no significant difference in age breakdown between sexes). Patients consulting a GP were older than those consulting a neurologist (Table 2).
The mean migraine history duration was 10.9 ± 9.6 years (minimum 1 year; maximum 68 years) and > 10 years for 33% of study patients (32% of patients consulting a GP; 47% of those consulting a neurologist; P < 0.01).
At entry to the study, the average intensity of past migraine attacks was described as severe by 66% of patients, moderate by 38% and/or mild by 3% (some patients reported different types of headache). The mean estimated frequency of headaches was 7.5 ± 5.0 days per month (minimum 1; maximum 31), with 39% of patients reporting 1–5 days with headache per month, 43% of patients 6–10 days, and 15% > 10 days. Based on these statements, 4719 patients (87%) were classified as having episodic migraine and 551 (10%) as having chronic daily headaches (≥15 days with headache per month).
Affective symptoms
Of the 5151 migraine patients with HAD scores available, 3428 (67%) suffered from anxiety (HAD anxiety score ≥ 8), of whom 1415 (28% of all patients) had anxiety alone and 2013 (39% of all patients) had both anxiety and depression (both HAD anxiety and depression scores ≥ 8). Only 124 patients (2%) exhibited depression alone and 1599 patients (31%) were neither anxious nor depressed.
For the patients who responded to the four questions of the MSQ4 (n = 5361) and of the PSS4 questionnaire (n = 5352), mean scores were 50.3 ± 20.3 and 10.6 ± 3.1, respectively, indicating substantial levels of functional impairment and stress.
For the patients who responded to the two questions of the avoidance subscale of the brief COPE inventory (n = 5399) and the four questions of the catastrophizing subscale of the CSQ (n = 5356), mean scores were 4.0 ± 1.5 and 9.5 ± 2.8, respectively.
All measures of affective symptoms, functional impact, stress, maladaptive coping strategies showed worse results (P < 0.01) for patients deemed eligible for prophylactic treatment by study physicians compared with those deemed ineligible (Fig. 2).
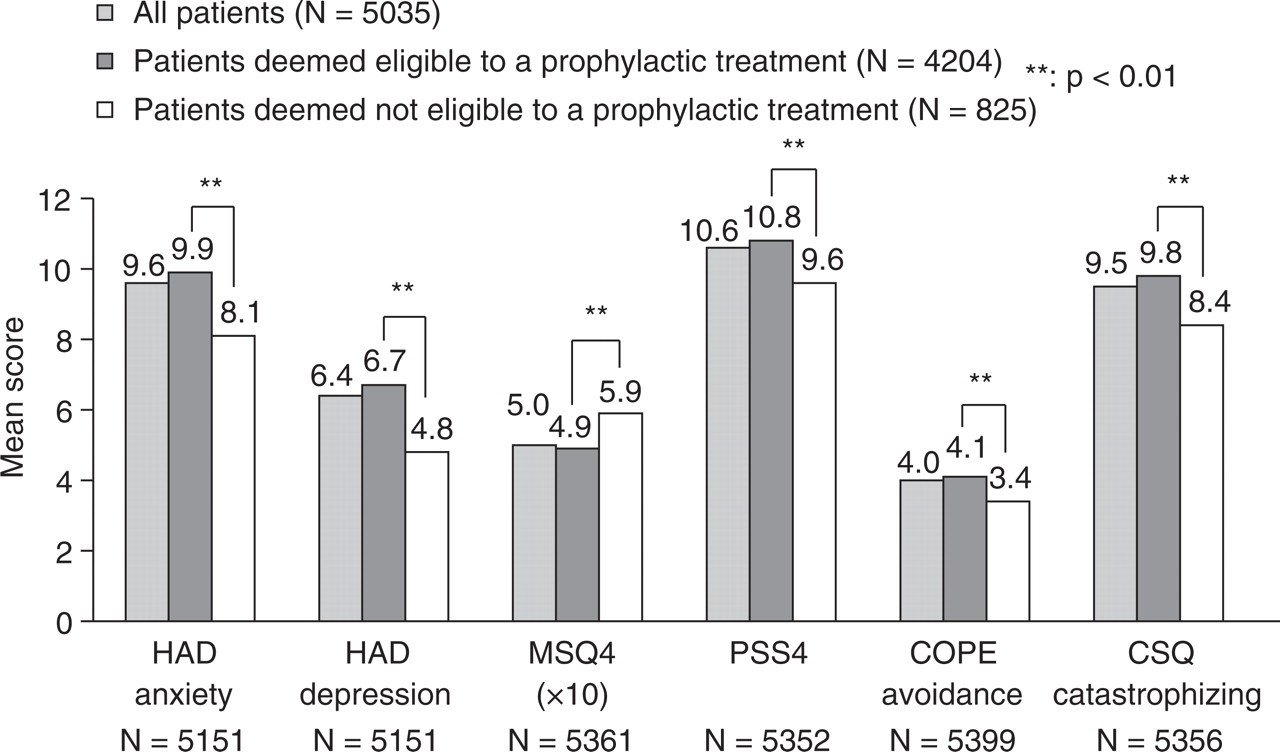
Anxiety, depression, functional impact, stress and maladaptive coping behaviours in all migraine patients and those deemed eligible or ineligible for prophylactic treatment by study physicians. HAD anxiety and HAD depression indicate Hospital Anxiety and Depression subscales (10). MSQ4 indicates abridged Migraine Specific Quality-of-life questionnaire (18, 19). PSS4 indicates abridged Perceived Stress Scale (17). COPE avoidance indicates brief COPE inventory avoidance subscale (21, 22). CSQ catastrophizing indicates Coping Strategies Questionnaire catastrophizing subscale (23, 24).
Acute management of migraine by study patients and treatment effectiveness
Most patients (n = 5035; 93%) used to take a medication to treat migraine attacks. Specific, recommended and other medications used as first-line acute treatments are presented in Table 3. The most frequently used first-line medications were triptans (32% of patients), followed by paracetamol (20%) and NSAIDs (18%).
First-line medications used by study patients who used to take (a) medication(s) to treat an attack

NSAIDs, Non-steroidal anti-inflammatory drugs.
Hypnotics, antidepressants, anxiolytics …
The mean severity of treated attacks as estimated on a scale from 0 to 10 was 6.8 ± 1.9. The mean number of drug units taken as first-line treatment was 3.1 ± 2.3 and the mean total number of units taken for a whole attack was 4.7 ± 3.7. The number of drug units taken at migraine onset according to the medication used is shown in Table 3. This number is minimal for specific and recommended medications, medium for non-specific recommended medications, and maximum for other medications.
Approximately half of patients reported some efficacy of the first-line medication used: 53% stated that they felt significant relief of migraine at 2 h after intake, 40% that they used a single drug unit, and 49% that they could rapidly resume normal activities. Most of them (91%) reported good treatment tolerability. On the whole, however, 74% answered ‘no’ to at least one question of the SFEMC/National Agency for Accreditation and Evaluation in Health (ANAES) questionnaire, indicating overall acute treatment ineffectiveness. This proportion was significantly higher among patients deemed eligible for prophylactic treatment (79%) compared with those deemed ineligible (50%; P < 0.01) (Fig. 3).
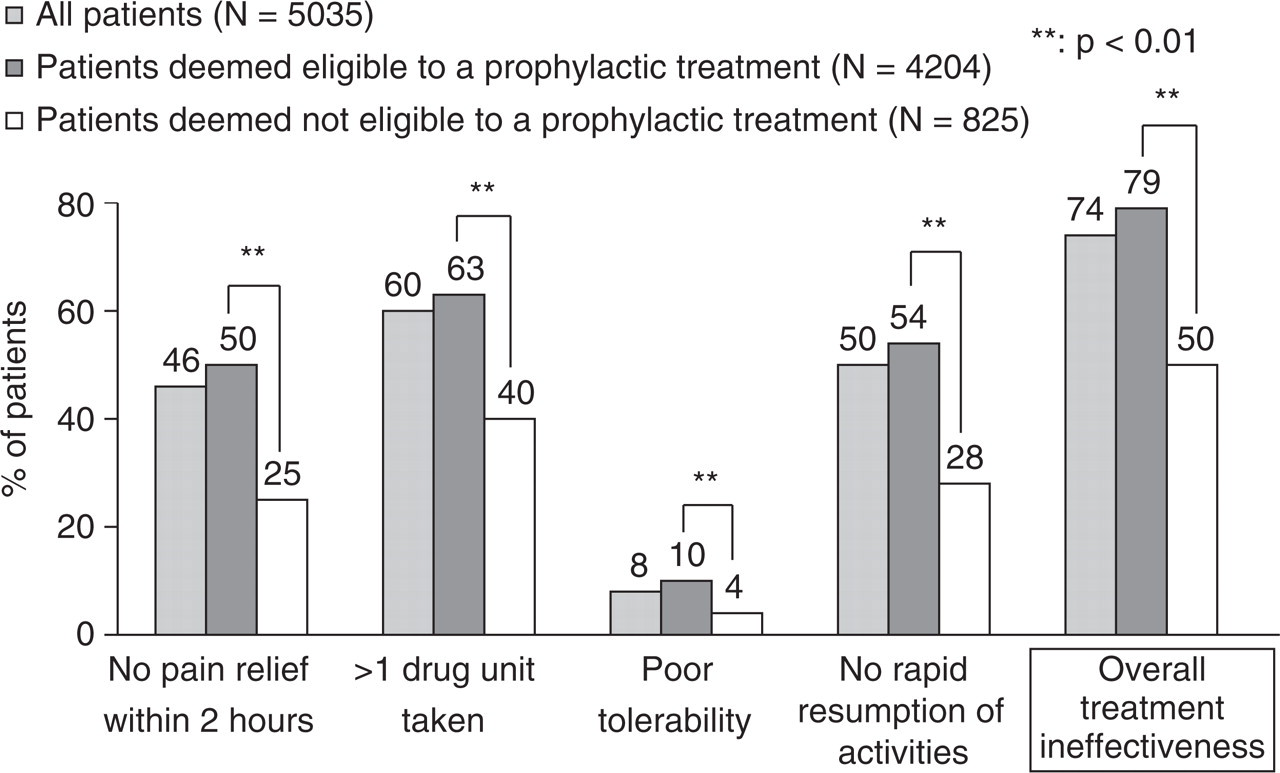
Effectiveness of the first-line acute treatment of migraine attacks in all patients and those deemed eligible or ineligible for prophylactic treatment by study physicians.
Treatments prescribed at end of consultation
A treatment for migraine (new or repeat prescription) was prescribed to nearly all patients (97%). The treatments prescribed at the end of the consultation by GPs and neurologists are presented in Table 4. Study neurologists prescribed recommended acute treatments (specific or non-specific) more frequently than GPs (P < 0.01), especially triptans and NSAIDs, whereas study GPs prescribed more frequently non-recommended treatments (paracetamol, opioids or other medications) (P < 0.01). Furthermore, GPs were found to prescribe prophylactic treatments more often than neurologists (P < 0.05) (Table 4).
Treatments prescribed at the end of the consultation

NSAIDs, Non-steroidal anti-inflammatory drugs.
Anxiolytics, antidepressants, hypnotics, homeopathy, magnesium …
A significant difference between the groups of patients consulting GPs or neurologists (P < 0.01 and P < 0.05, respectively).
Discussion
The SMILE study is the first prospective observational study conducted on a large sample of migraine patients consulting GPs and neurologists in France. This study reports the data collected at study entry. The results obtained highlight the serious character of migraine and profound maladjustment of patients consulting in primary care. Study patients generally had a long history (>10 years on average) of migraine headaches of severe intensity (66% of patients) with frequent attacks (every fourth day on average). As many as 10% of patients had chronic daily headaches. Two-thirds of patients suffered from anxiety. Stress and functional impairment were substantial and many patients exhibited maladaptive coping behaviours. Many patients used to take an elevated number of drug units to treat an attack (three units on average at migraine onset, nearly five units in total for a whole attack), especially when they used non-recommended medications. Considering migraine relief at 2 h, treatment tolerability, the number of drug units taken and length of time before resumption of normal activities (SFEMC/ANAES questionnaire), the usual acute treatment of migraine attacks appeared ineffective in 74% of patients.
The first objective of the SMILE study was to describe the profile of migraine patients consulting GPs or neurologists. In the SMILE study, the female:male ratio was 4.0. This proportion is higher than that usually reported for migraine patients in community-based surveys in France (2.2–2.8) (3, 4, 26), but similar to the female:male ratio of 4.18 reported among current consulters in a preceding French survey (4), which confirms that more female than male patients consult for migraine. A US survey has reported a female:male ratio of 2.9 for migraine in the general population, with 73% of women consulting vs. 49% of men, giving a comparable estimated female:male ratio of 4.3 among consulters (27). The mean age of SMILE patients (41 years) was identical to that of migraine patients in a community-based survey (26). Mean migraine history duration (11 years) was somewhat shorter than that observed in the preceding French community-based studies (13–17 years) (3, 4, 26). In the SMILE study, migraine history duration was less frequently > 10 years among patients consulting GPs than those consulting neurologists, although patients consulting GPs were generally older, indicating that patients with a lengthy history of migraine are more often followed up by neurologists. The intensity of migraine attacks was described as severe by 66% of consulting patients in the SMILE study. Very variable proportions of patients with severe/very severe pain intensity have been reported in previous community-based surveys, regardless of whether pain intensity was evaluated using a verbal scale (32–64% of patients with severe or very severe attacks) (3, 26) or a 0–10 numerical scale (50–87% of patients with pain intensity graded from 7 to 10 (4, 27). The mean frequency of headaches was 7.5 ± 5.0 days per month in the SMILE study compared with 6.9 ± 6.8 days over 3 months in a previous community-based study in France (4). More than half of study patients (58%) reported > 6 days with headache in a month, whereas in previous community studies only one-quarter of migraine patients (24–29%) reported one attack or more per week (3, 4, 27). On the whole, it appears that patients consulting for migraine are more likely to be female patients who experience more frequent attacks than the general population of migraine sufferers, which contains approximately 80% of non-consulters in France (1). However, since the data pertaining to migraine characteristics at inclusion rely on self-reports and are not prospectively recorded on diary cards, these results may to some extent be subject to recall bias.
Two-thirds of patients consulting for migraine (67%) suffered from anxiety (28% from anxiety alone, 39% from anxiety and depression) and 2% from depression alone. The proportion of patients with anxiety in the SMILE study was higher than that observed in two preceding community-based French and Norwegian surveys (51% and 24%, respectively) using the same HAD cut-off score of 8 (11, 12). This larger proportion of anxious patients was not unexpected, as anxious patients are known to be more prone to consult than non-anxious patients (28). However, the proportion of anxious patients in the SMILE study was also higher than that (50%) observed with the same HAD cut-off score in a study that included principally patients attending migraine clinics (> 600 patients) and a minority of patients (n = 87) recruited by face-to-face interviews from the general population (9). In this English study, there was no difference between the two groups in their levels of anxiety, despite a higher rate of patients experiencing frequent migraine attacks among those attending migraine clinics (33% of consulting patients with four or more attacks per month vs. 17% of patients from the general population). The elevated frequency of migraine attacks in our sample of migraine patients may thus not be the only cause of the higher rate of anxious patients in the SMILE study compared with community-based studies. It is of note that in their original publication Zigmond and Snaith proposed HAD scores of 8–10 to indicate possible cases of anxiety or depression and scores of 11–21 to indicate probable cases (10). The low threshold of 8, which has been shown to allow identification of both anxiety and depression with high sensitivity and specificity (15, 16), was retained for the SMILE study in order to identify as many anxious patients as possible. Using a higher cut-off score might have led to somewhat different study results.
Regarding depression, the very low proportion of migraine patients with depression alone does not allow accurate interpretation. This low proportion was in fact not unexpected, since most of the time anxiety is comorbid with depression (29), especially in migraine sufferers (30). Most depressed patients are therefore to be found in the group of patients with both anxiety and depression.
One prominent result of this first phase of the SMILE study is the very low rate of migraine patients who used an effective abortive treatment of migraine attacks. According to the four-item SFEMC/ANAES questionnaire, as many as 74% of consulters used a treatment that was found to be ineffective, although 61% used recommended treatments (triptans, NSAIDs, ergot derivatives, aspirin alone or combined with metoclopramide). On average, study patients used to take a total of nearly five drug units for the treatment of a single attack, especially of non-recommended medications (paracetamol, opioids), which involves the risk of medication overuse. Finally, at the end of the consultation, recommended treatments were prescribed to only 46% of patients, more by neurologists than by GPs. Conversely, GPs were found to prescribe prophylactic treatments slightly more frequently than neurologists, but this may not reflect the management of migraine by GPs in real medical practice due to the specific characteristics of the sample of physicians recruited for the study (habitual prescribers of prophylactic treatments for migraine).
The results of the SMILE study indicate that consulting migraine patients present with relatively severe disease (frequent migraine attacks associated with substantial levels of anxiety, functional impact and stress). One might argue that recruitment of patients by physicians who were habitual prescribers of migraine prophylactic medications might have led to the selection of more severe and comorbid migraine cases. As SMILE is the first study in France to investigate the characteristics of consulting migraine patients, there are scant reference data—which indeed prompted the setting up of the SMILE study. A survey was carried out in the South of France on a sample of 176 migraine patients recruited, among 696 patients consulting for various pathologies, in the waiting rooms of 49 GPs (31). The mean age of these consulting patients (44.2 ± 16.8 years) was slightly lower than that of the SMILE patients (48.9 ± 7.4 years) and the women:men ratio was also lower (72/28 vs. 81/19, respectively). However, 50% these migraine patients reported a severe or very severe impact of migraine on social functioning, pain, emotional distress, well-being, cognitive functioning and vitality, as assessed by a score of > 60 on the Headache Impact Test (HIT)-6 scale (scale span of 36–78) (32). Comparatively, in the SMILE study, migraine functional impact as assessed using the MSQ4 questionnaire was 50.3 ± 20.3 on the 0–100 scale. These data suggest that the sample of migraine patients recruited for the SMILE study may be considered comparable in disease severity to the general population of patients consulting for migraine in general medical practice.
On the other hand, the high rate of patient eligibility for prophylactic treatment found in the SMILE study (83%) is probably the consequence of the open character of the study and the characteristics of participating physicians. Nevertheless, significant differences were observed between groups of patients according to eligibility or ineligibility for prophylactic treatment. It is remarkable that all psychometric measures (of anxiety, depression, functional impact, stress, maladaptive coping behaviours) were significantly linked with estimated eligibility for prophylactic treatment. Additionally, all four items of the SFEMC/ANAES questionnaire were also significantly linked with eligibility for prophylactic treatment. On the whole, these results may reflect, on the one hand, the perception by physicians of the relatively weak effectiveness of abortive treatments of migraine in a substantial proportion of patients and, on the other hand, the perception of the potential of prophylactic treatments for reducing the rate of recurrence of migraine attacks and therefore relieving migraine-related psychological disorders.
In conclusion, the results of the SMILE study highlight the seriousness of migraine and maladjustment of patients consulting in primary care, with high rates of anxiety, maladaptive behaviours and ineffectiveness of acute treatments of migraine. Further phases of the SMILE study will enable assessment of the evolution of migraine characteristics, especially severity and frequency of attacks as well as migraine-related mood disorders, stress, functional impact and coping behaviours, after 2 and 4 months of the treatment prescribed to study patients.
Footnotes
Acknowledgements
The authors thank Geneviève Bonnelye, TNS Healthcare, for managing the project, Séverine Ricard and Xavier Guillaume, TNS Healthcare, for carrying out the study and statistical work, and Jacques Legeai, Redasciences-Santé sarl, for his help in writing the study.