
Abstract
To the best of our knowledge, persistent visual symptoms, lasting months or years without evidence of infarction, a rare complication of migraine with aura, has been reported in only 20 patients. We report the case of a 43-year-old woman with a 31-year history of migraine with typical visual aura. At presentation, she experienced a visual aura in her right hemifield followed by a pulsating headache. The visual symptoms persisted. There were no abnormal findings on neurological and ophthalmological examinations, EEG, visual evoked potentials (VEPs), brain computed tomography and magnetic resonance imaging (MRI). Both brain single photon emission compted tomography (SPECT) and brain perfusion MRI revealed decreased left fronto-parieto-occipital and right occipital blood perfusion. A perfusion MRI, performed 7 months after symptom onset and almost complete extinction of symptoms, was normal. As previously reported, we demonstrated a cortical hypoperfusion by SPECT in a case of persistent visual aura. For the first time this finding was confirmed by perfusion MRI.
Introduction
In the Classification and Diagnostic Criteria for Headaches Disorders, Cranial Neuralgias and Facial Pain (1), migraine with aura is decribed as follows: ‘an idiopathic, recurring disorder manifesting with attacks of neurological symptoms unequivocally localizable to cerebral cortex or brain stem, usually gradually developed over 5–20 minutes and usually lasting less than 60 minutes. Headache usually follows neurological symptoms but may be completely absent’.
In the recently published International Classification of Headaches Disorders (2), among the complications of migraine was inserted a rare but well-documented form characterized by aura symptoms persisting for more than 1 week without radiographic evidence of infarction. To the best of our knowledge, only 20 cases of such a complication have been reported as ‘sustained visual aura’ or ‘persistent positive visual phenomena’(3–9).
We report a new case studied with brain single photon emission computed tomography (SPECT) and, for the first time, with perfusion magnetic resonance imaging (MRI).
Case report
A 43-year-old woman had a 30-year history of low frequency migraine with typical visual aura. She experienced an average of two migraine attacks a year characterized by blurring of central vision, followed by the vision of a pattern of colours with changes, ‘like looking through a kaleidoscope’, that spread from the centre to the right hemifield, spontaneously disappeared within 10–25 min, giving way to a pulsating, unilateral, temporo-orbital left headache of severe intensity lasting up to 12 h, always associated with nausea, photophobia and phonophobia. A precipitating factor was never identified in this patient.
At presentation, she reported a visual aura in her right hemifield followed by a pulsating headache whose intensity changed from severe to moderate over 3 h after treatment with rizatriptan. The visual symptoms, consisting of a bright halo on the right edge of the objects and a scintillating scotoma with grey and white squares, ‘like a chessboard’, in the right hemifield, became persistent after a fluctuating course of 24 h.
There were no abnormal findings on neurological and ophthalmological examination, including visual acuity, colour vision, kinetic and computerized perimetry and ophthalmoscopy. Routine haematological assays, electroencephalography, visual cortical evoked potentials, Doppler ultrasonography of intracranial and extracranial arteries, brain computed tomography and MRI were all normal.
In the following days the visual symptoms partially receded, but the bright halo at the right edge of the objects and the pattern of the ‘chessboard’, though less impressive, persisted and reading was difficult since the final letters of some words were missing when she was looking from left to right.
A brain SPECT with technetium Tc99m hexamethylpropyleneamine oxime (Tc99m-HMPAO), performed 1 month after symptom onset when the visual deficit was still significant, revealed decreased left fronto-parieto-occipital and right occipital blood perfusion (Fig. 1).
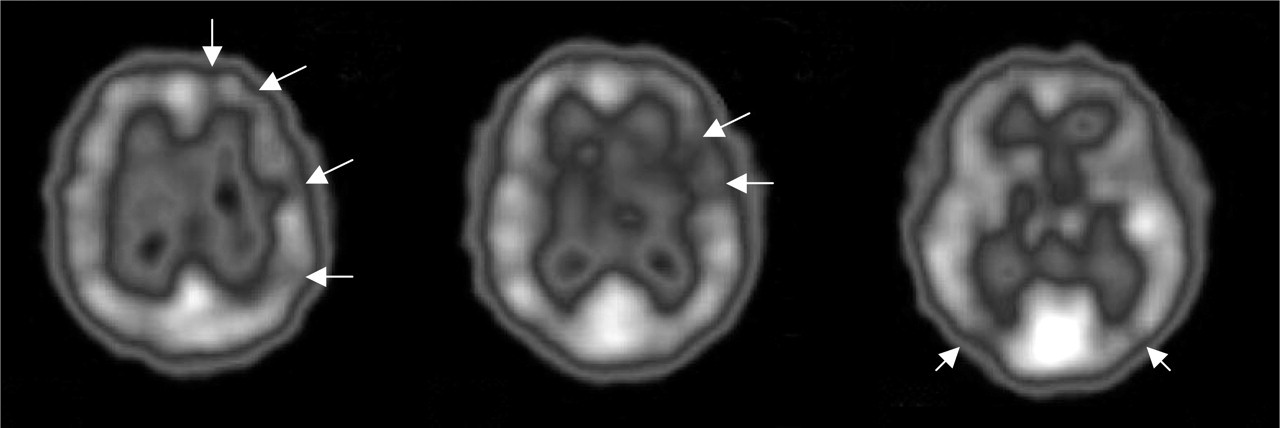
Brain single photon emission compted tomography with technetium Tc99m hexamethylpropyleneamine oxime of the patient with persistent aura without infarction. A decreased left fronto-parieto-occipital and right occipital blood perfusion (arrows) are shown.
The patient underwent two brain perfusion MRI examinations by using a 1.5-T magnet (Intera Master; Philips, Best, the Netherlands). The perfusion weighted images were acquired during the first pass of a paramagnetic contrast media (0.02 mmol/kg; injection rate 5 ml/s). Forty dynamic scans (11 slices, slice thickness 7 mm, TR = 610 ms, TE = 30 ms, FA = 40°, total scan time = 1.16 min) were obtained. The data were transferred on a separate console (Easy Vision; Philips). Measurements were obtained bilaterally at the level of the grey matter of temporal, occipital, parietal and frontal lobes and signal intensity vs. time curves were obtained. In each lobe, four measurements were performed. The regions of interest were chosen at random. The first examination, performed 6 weeks after symptom onset, showed a decreased perfusion ranging from 18% to 25% in the left hemisphere compared with the right (occipital lobe 18%, temporal lobe 18%, parietal lobe 25%, frontal lobe 21%). At that time the visual symptoms were partially receding but still markedly interfered with the patient's ability to read. A new perfusion MRI examination, performed 7 months after symptom onset, when the patient had had an almost complete reduction of symptoms (only a slight difficulty in reading remaining), showed a normal perfusion in the left hemisphere without differences with the contralateral hemisphere. Figure 2 shows the signal intensity vs. time curves relative to occipital lobes.
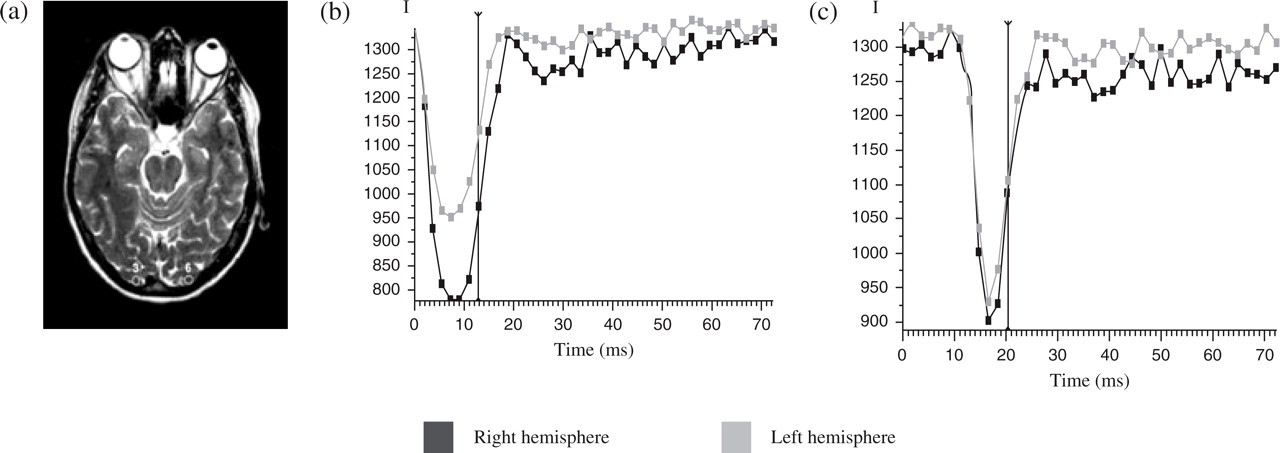
Perfusion magnetic resonance imaging of the patient with persistent aura without infarction. (a) The regions of acquisition (3, 6) of the signal in the occipital lobes. (b) The decrease of the intensity of the signal (I) in the left occipital cortex 6 weeks after the onset of the symptomatology. (c) The restoration of the intensity of the signal in the 7-month follow-up examination.
The patient was treated with lamotrigine 75 mg/day according to a previous report showing the possible efficacy of this drug (9). In this case the benefit of lamotrigine is difficult to demonstrate since visual symptoms were long-lasting and very slow to resolve. In fact, at 18-month follow-up, the patient still complained of slight visual disturbances, especially when reading.
She reported a much less severe episode of visual aura with progressive and spontaneous resolution within 3–4 months at age 40. In that occasion she was not referred to a neurologist.
Discussion
Visual migrainous aura consists of visual symptoms including positive features (i.e. scintillating scotomas, flickering lights, fortification spectrum) and/or negative features (i.e. loss of vision, scotomas, quadrantanopsia, hemianopsia), much rarely metamorphopsia or palinopsia.
Visual symptoms of typical migrainous aura seem related to a pathophysiological mechanism similar to spreading depression (SD) of Leão in the occipital cortex (10). SD is a neuronal depolarization wave with subsequent suppression of electrical activity that moves across contiguous cortical areas at a rate of about 2–5 mm/min after mechanical or chemical perturbation of the cortex in experimental animals. SD is followed by changes of the regional cerebral blood flow (rCBF). Several studies have demonstrated, before or simultaneously with the onset of aura symptoms, a decrease in rCBF lasting 30–60 min that starts in the occipital cortex, spreads anteriorly to the parieto-temporal region and spontaneously comes to a resolution (5, 11–17). Actually, the hypoperfusion is preceded by a wave of hyperaemia, shown both in animal and human studies (10, 18, 19). Occasionally, the hypoperfusion involves an entire hemisphere or both (5). SPECT studies showed a 17–35% reduction of rCBF (12, 13). This finding was confirmed by positron emission tomography (PET) and functional MRI studies that are less prone to technical flaws such as Compton's effect (14–16). Furthermore, in patients suffering from migraine with aura, a significant asymmetry of rCBF has also been reported between attacks (17).
The pathophysiology of sustained visual aura is not yet established. Pathophysiological mechanisms suggested in magnetic resonance spectroscopy studies in migraineurs with typical aura (19), i.e. abnormal energy metabolism in the brain, brain magnesium levels significantly lower than that of non-migraineurs, greater reactivity of N-methyl-D-aspartate receptors to glutamate, a lowered threshold to SD, and loss of inhibitory gabaergic interneurons, may combine to cause sustained visual aura. It has also been hypothesized that sustained reverberating waves of SD may be implicated. The results of SPECT and PET studies evaluating, respectively, CBF and cerebral metabolism have supported this hypothesis (4, 5, 8, 9).
Only 10 out of 20 cases of sustained visual aura reported in the literature have been studied with Tc99m-HMPAO SPECT. The study of rCBF in patients with persistent aura limited to one hemifield showed more frequently, as has been demonstrated in typical migrainous aura, a hypoperfusion in the posterior regions of the contralateral cerebral cortex (three patients) (5, 9), and, more rarely, a hypoperfusion of the whole hemisphere (one patient) (4). Of the six patients who complained of sustained aura that involved all the visual field, three had an oligoemia in the posterior regions of the cerebral cortex bilaterally and one in the left temporal lobe, whereas two showed a normal SPECT (5). Only three patients, who showed a unilateral hypoperfusion in the posterior regions, performed a second Tc99m-HMPAO SPECT after the remission of symptoms. In two of them the oligoemia disappeared totally (9), whereas in one patient a hypoperfusion persisted especially in the thalamus, in the temporal lobe and in the posterior cingulated gyrus (5).
A single study of two patients used fluorine-18 labelled deoxyglucose PET and showed a persistent increase of metabolic activity in the medial occipital cortex, thus supporting the hypothesis of a constant activation of the visual cortex (8).
In the present report a patient with sustained visual aura was studied for the first time with perfusion MRI. This examination showed a cortical hypoperfusion when the symptoms were present and the normalization of the cerebral perfusion at the remission of symptomatology. These findings demonstrated that: (i) the reduction of CBF occurs concomitantly with aura symptoms, and (ii) the decrease of CBF must be above the ischemic threshold since a cerebral infarction did not develop. Finally, it is worth mentioning that this patient had neither risk factors nor signs or symptoms of cerebrovascular disease that can account for changes in CBF.
Footnotes
Acknowledgements
The study was supported by a grant of the University of Trieste, Italy, Murst 60%.