
Abstract
Background
Headache is common in adolescents and affects schoolwork and relations with friends and family. In most previous epidemiological surveys, only the most bothersome headache has been documented. The aim was to determine headache prevalence not only taking into account the most bothersome headache, but also to compare characteristics of the most bothersome and less bothersome headaches, and to investigate headache-related disability.
Methods
A cross-sectional school-based study was conducted in which 493 representative adolescents aged 12–18 years were recruited by stratified cluster sampling and interviewed. Headache diagnosis was made according to the new classification system of the International Headache Society (ICHD-3 beta), and the Pediatric Migraine Disability Assessment (PedMIDAS) was used to evaluate disability.
Results
The one-year prevalence of any headache type, definite migraine, probable migraine and tension-type headache was 88%, 23%, 13% and 58%, respectively. The point prevalence of any headache was 38%. Nine percent of participants fulfilled criteria for more than one headache diagnosis. The most bothersome headache had a significantly longer duration (p < 0.001) and higher intensity (p < 0.001) than the less bothersome headache, but similar frequency (p = 0.86). Adolescents with headaches lost up to nine days of activity each year, implicating headache as a major health issue.
Conclusions
Headaches are very common and disabling among adolescents. The full extent of this health problem is better appreciated if inquiry is not limited to the most bothersome subtypes.
Background
Headache is one of the most common health problems in adolescents (1,2) and can negatively affect quality of life and lead to impairments in daily functioning such as school performance and recreational activities (3,4). Surveys conducted in different countries and cultures show considerable variation in the estimated prevalence of headache, and a recent review reported an overall median of 5% for one-year prevalence of headache in adolescents (1). Many studies have considered only the most bothersome headache in adolescence, whereas others have limited the prevalence estimates to strict diagnoses, thereby disregarding the existence of probable migraine (PM) and probable tension-type headache (PTTH) (5,6).
The main objectives of the present epidemiological study were to determine the prevalence of headache, taking into account more than one type of headache in each participant, to compare the differences in the characteristics of the most bothersome and other headaches, and to investigate headache-related disability in adolescents in the general population.
Methods
Study population and sample selection
The study population was students from secondary schools and high schools in Sør-Trøndelag County in Norway. Sampling was stratified by grade and location. Data were collected in 2011–2012. As of January 1, 2011, Sør-Trøndelag County had 294,066 residents: 173,486 in the city of Trondheim, 83,451 in the inland/mountain region and 37,129 by the coast (7). To obtain a sample distribution corresponding to the distribution of the population in the county, the schools were initially drawn with the following probabilities: 59% from the urban region, 28% from the inland-mountain region and 13% from coastal municipalities. The study sample was recruited in equal proportions from three grade cohorts from two types of schools: eighth grade (age 12–13 years), 10th grade (age 14–15 years) both from secondary schools, and 12th grade (age 16–18 years) from high schools. There are large differences in school size with more students in schools in urban vs rural areas, and a higher number of schools were therefore needed to be drawn from rural areas to obtain the required number of participants. First we drew what grades we should invite, then the school. Then all the students in the drawn-class level of the current school were invited to attend the study. At the time of the study, there were 74 secondary or high schools in Sør-Trøndelag County. Thirteen of these were invited to participate in the study: four of the 26 schools in an urban area and nine of the 48 schools in a rural (inland/mountain or coastal) area. Of the initial 13 schools invited, seven schools declined to participate in the study and were replaced by seven new schools (four from the inland/mountain area, one from the coastal area, and two from the urban area). The four schools in urban areas that agreed to participate were two secondary schools (individuals in the eighth and 10th grades) and two high schools (individuals in the 12th grade). Of the latter, one school specialized in vocational training, and one specialized in theoretical sciences. The nine schools in rural areas that agreed to participate were four secondary schools from the coastal region, three secondary schools from the inland/mountain region, one high school from the coastal region, and one high school from the inland/mountain region. Data from the inland/mountain and coastal regions were combined and labeled “rural.”
Recruitment procedure
There were 899 eligible students invited to participate in the study. The interviewer (ABK) held an information meeting with principals, inspectors and teachers from each of the selected schools to motivate them to participate in the study. The interviewer met with all students who had been selected for participation, and they also received written information about the study. As an incentive, students were offered a cinema ticket for participation. Norwegian law requires parental consent for children younger than 16 years of age to participate in research; therefore, the interviewer also provided optional meetings for parents with children in these age groups with the purpose of informing them about the study.
Questionnaire and interviews
The questionnaire was developed for school-based studies of headache in Sweden (8–10), translated to Norwegian and adapted to the diagnostic criteria from the International Headache Society (IHS) (11). All interviews were conducted face to face by the same experienced nurse in a suitable room at the school during a regular school day and lasted, on average, 20 minutes. As an opening question, the student was asked whether he or she had experienced headache during the past year. For those who answered “No” to this question, the interview stopped. For those who answered “Yes,” a structured interview was conducted to determine the headache characteristics. The researcher asked if the student had experienced more than one type of headache during the last year. If positively endorsed, the characteristics and associated symptoms of headache were documented for up to two headache types. Students were asked to report the frequency, intensity (on a three-point scale: 1 = mild, 2 = moderate, 3 = severe) and duration of episodes, as well as the accompanying symptoms. At the very end of the interview, students were asked to assess the severity of any headache that they had experienced during the interview on a 100 mm visual analog scale (VAS) with the following end points: “None” and “As bad as it could be” (12).
Headache classification
Headaches were classified as episodic migraine with or without aura (MA or MwoA), chronic migraine (CM), probable migraine, episodic tension-type headache, infrequent (ITTH) or frequent (FTTH), chronic tension-type headache (CTTH) or medication-overuse headache (MOH) according to the International Classification of Headache Disorders, third edition beta (ICHD-3 beta) (13). PTTH was merged with definite TTH. MOH was defined as having any headache (including the most bothersome headache and any other headache) for more than half of the days during the last three months and treating it with medication on at least 10 days per month. Headache that did not fulfill any criteria according to ICHD-3 beta was labeled “unclassifiable.” One of the authors, a neurologist (ML) with extensive experience in the diagnosis and epidemiological research of headache, verified all final diagnoses.
The study was conceived at the time criteria of headache classification from the IHS (ICHD-2) (11) was the prevailing set of diagnostic criteria. But information on headache duration was collected in such detail that data could instead be evaluated using the contemporary criteria of headache classification from the IHS (ICHD-3 beta) (13).
Pediatric Migraine Disability Assessment (PedMIDAS)
Students were also asked to complete the PedMIDAS, which was developed to assess disability in children and adolescents with chronic pain, including headache, and has been used in clinical studies and epidemiological surveys (14–16). It consists of six questions addressing the number of days totally or partially lost because of headache for the last three months (91 days) in three domains (school, home and social activities). A total score was calculated for each adolescent by summing the number of days reported for each of the items for all headaches as recommended by the creator of the PedMIDAS (14). The PedMIDAS grading system was used to indicate the degree of headache disability. Grade I means little to no disability (0–10), Grade II means mild disability (11–30), Grade III means moderate disability (31–50) and Grade IV means severe disability (>50) (15).
Statistics and data analysis
Descriptive data were expressed as means and standard deviations (SD), as the percentage with 95% confidence interval (CI) for continuous variables, and as the median and interquartile range for ordinal variables. The chi-square test was used to examine associations between categorical variables and Pearson product-moment correlations were used to examine associations between continuous variables. Differences between independent group means and medians were examined using Mann-Whitney tests and Kruskal-Wallis tests for ordinal variables. Differences between independent group means and medians were examined using analysis of variance (ANOVA) to examine assosiations between continous variables. The Wilcoxon test was used for paired within-group comparisons. To account for the risk of mass significance due to statistical comparisons, a highly conservative Bonferroni-adjustment was applied throughout using an alpha lowered to 0.002 (0.05 divided by 25 analyses). IBM SPSS Statistics for Windows version 20 was used for all statistical analyses.
Ethics
The Norwegian Ethical Committee for Medical Research and the Norwegian Social Science Data Service approved the research protocol.
Results
The flow of participants in the study is presented in Figure 1. Of 899 invited students, written consent was obtained from 519 (58%). Twenty-six of the adolescents did not attend the interview. Of these students, 15 were sick, six did not attend the interview because of an unknown cause, two were on vacation, one withdrew from the study, one had practical studies outside school and one had exams. After the interviews were completed, five students were excluded because they were older than 18 years. Thus, the final study population consisted of 488 adolescents, 57% girls (n = 276) and 43% boys (n = 212), with an age range of 12–18 years. The distributions across grades and school location (urban/rural area) are presented in Table 1.
Flow of study participants. Prevalence of ICHD-3 beta headache disorders for the total sample and by sex, age and school location. ICHD-3 beta: International Classification of Headache Disorders, third edition beta; MwoA: migraine without aura; MA: migraine with aura; PM: probable migraine; ITTH: infrequent tension-type headache; FTTH: frequent tension-type headache, CM: chronic migraine, CTTH: chronic tension-type headache; MOH: medication-overuse headache; Uncl: unclassifiable headache; 95% CI: 95% confidence interval. an adolescent can have more than one headache diagnosis. The row for MA, for example, shows the characteristics of those adolescents for whom either type of headache is MA.

One-year prevalence of headache
Of the 488 participants, 429 reported experiencing a headache in the past 12 months, giving a one-year prevalence of 88% (95% CI, 85–91%; Table 1). The prevalence of headache was significantly (p < 0.001) higher in girls than boys (93% vs 80%), but was similar across grades (p = 0.24) and urban and rural locations (p = 0.057). Of the 488 participants who reported headaches, 7.4% (n = 36, 18 girls, 18 boys) had headaches only associated with another illness such as cold or flu.
The one-year prevalence of definite migraine (i.e. MwoA, MA or CM as first or second headache) was 23% (95% CI, 19.3–26.7%), and the one-year prevalence for PM was 13% (95% CI, 10.0–16.0). With Bonferroni adjustment there was no significant difference between girls and boys (p = 0.002), grades (p = 0.47) or urban and rural locations (p = 0.059). The prevalence of migraine subtypes is presented in Table 1.
The overall prevalence of any TTH (i.e., ITTH, FTTH, PTTH or CTTH as first or second headache) was 58% (95% CI, 54–62%; Table 1), similar in boys and girls (p = 0.79), across grades (p = 0.15) and in urban and rural locations (p = 0.79). The prevalence of TTH subtypes is presented in Table 1.
Sixty-five adolescents (45 girls, 20 boys) considered themselves to have more than one type of headache, and 45 of them fulfilled diagnostic criteria for more than one diagnosis. All of the latter reported migraine as the most bothersome headache (23 MA, 14 MwoA, one CM, seven PM). Six adolescents also had definite or PM as the less bothersome headache (four MwoA, two PM). The remaining 39 adolescents with two diagnoses had TTH as the less bothersome headache (26 FTTH, 13 ITTH).
Point prevalence of headache
A total of 160 adolescents (38%) experienced headache during the interview. Of these, 104 (65%) rated the severity ≤ 20 mm on the VAS, 37 (23%) rated the severity 21–40 mm on the VAS, 12 (8%) rated the severity 41–60 mm on the VAS, and seven (4%) rated the severity > 60 mm on the VAS. The results of analysis of variance (ANOVA) showed no main effects of sex and grade on the VAS score (p = 0.24 and 0.77, respectively) and no sex and grade interaction (p = 0.34). Student's t-test showed no significant difference between rural and urban locations (p = 0.11).
Frequency of headache
Frequency, intensity, and duration of most bothersome headache by sex, age and school location.

Figures in numbers and percentages within parenthesis.
Frequency, intensity, and duration of headache by headache diagnoses.

Figures in numbers and percentages within parenthesis. MwoA: migraine without aura; MA: migraine with aura; PM: probable migraine; ITTH: infrequent tension-type headache; FTTH: frequent tension-type headache, CM: chronic migraine, CTTH: chronic tension-type headache; MOH: medication-overuse headache; Uncl: unclassifiable headache; 95% CI: 95% confidence interval. an adolescent can have more than one headache diagnosis. The column for MA, for example, shows the characteristics of those adolescents for whom either type of headache is MA.
Among the 45 adolescents (9% of all participants) who fulfilled ICHD-3 beta criteria for more than one type of headache, there was no significant difference in headache frequency between the most bothersome and the less bothersome headache (p = 0.86). The frequency of the most bothersome headache was <1 day a month for 18 adolescents (40%), one to three days a month for 18 adolescents (40%), one to three days a week for seven adolescents (16%), and every other day or more often for two adolescents (0.4%). The frequency of the less bothersome headache was <1 day a month for 12 adolescents (27%), one to three days a month for 16 adolescents (36%) and one to three days a week for 17 adolescents (38%).
Duration of episodes
The duration of the most bothersome headache is presented by sex, grade and school location in Table 2 and by headache diagnoses (also considering any second headache) in Table 3. There was no significant difference in the duration of the most bothersome headache between girls and boys (p = 0.99), across grades (p = 0.17), or between urban and rural areas (p = 0.074; Table 2).
In the 45 adolescents who fulfilled ICHD-3 beta criteria for more than one type of headache, the duration of the most bothersome headache was significantly (p < 0.001) longer than that of the less bothersome headache. The duration of the most bothersome headache was <2 hours in seven adolescents (16%), two to four hours in three adolescents (7%), four to 24 hours in 25 adolescents (56%), one to three days in 12 (27%) adolescents, and >3 days in one adolescent (2%). The duration of the less bothersome headache was <2 hours in 10 adolescents (22%), two to four hours in 19 adolescents (42%), four to 24 hours in 14 adolescents (31%), and one to three days in two adolescents.
Headache intensity
The estimate of headache intensity is presented by sex, grade and school location in Table 2 and by headache diagnoses (also considering any second headache) in Table 3. A minority of adolescents reported headache intensity as mild (18%), whereas 57% reported headache intensity as moderate and 25% reported headache intensity as severe (Table 3). The mean headache intensity and standard deviation was 2.1 ± 0.7, the median was 2 and the interquartile range was 2.
There was no significant difference in the intensity of the most bothersome headache between girls and boys (p = 0.093), across grades (p = 0.17), between urban and rural school locations (p = 0.13).
In the 45 adolescents who fulfilled ICHD-3 beta criteria for more than one type of headache, there was a significantly (p < 0.001) greater headache intensity in the most bothersome vs the less bothersome headache. The intensity of the most bothersome headache was either moderate (n = 9, 20%) or severe (n = 36, 80%), whereas the intensity of the less bothersome headache was mild (n = 19, 42%) or moderate (n = 26, 58%).
Headache-related disability
Headache-related disability (PedMIDAS scores) by diagnoses.
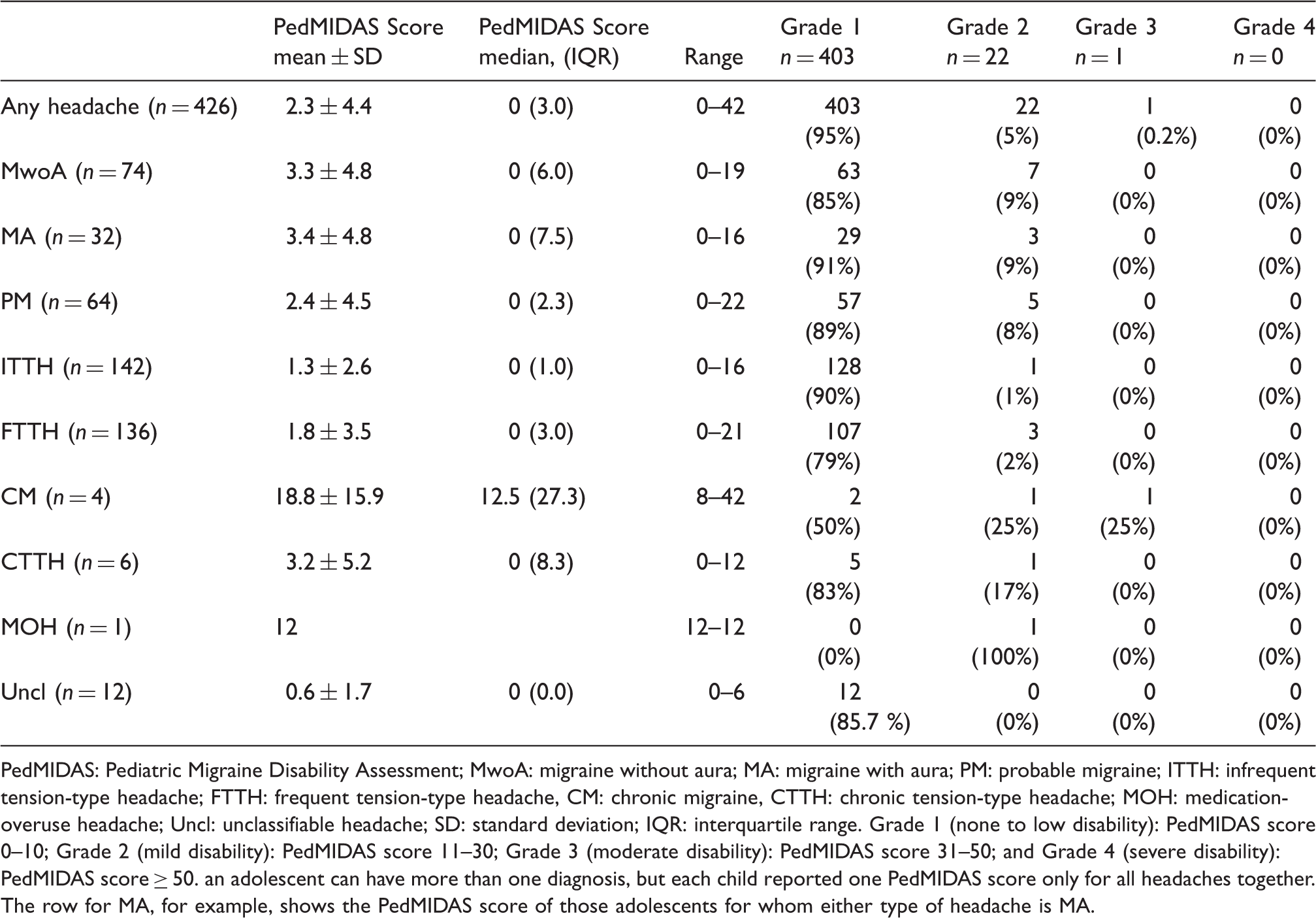
PedMIDAS: Pediatric Migraine Disability Assessment; MwoA: migraine without aura; MA: migraine with aura; PM: probable migraine; ITTH: infrequent tension-type headache; FTTH: frequent tension-type headache, CM: chronic migraine, CTTH: chronic tension-type headache; MOH: medication-overuse headache; Uncl: unclassifiable headache; SD: standard deviation; IQR: interquartile range. Grade 1 (none to low disability): PedMIDAS score 0–10; Grade 2 (mild disability): PedMIDAS score 11–30; Grade 3 (moderate disability): PedMIDAS score 31–50; and Grade 4 (severe disability): PedMIDAS score ≥ 50. an adolescent can have more than one diagnosis, but each child reported one PedMIDAS score only for all headaches together. The row for MA, for example, shows the PedMIDAS score of those adolescents for whom either type of headache is MA.
The results of a Mann-Whitney test using the PedMIDAS score as a dependent variable showed no significant effect of sex (p = 0.94) or location (p = 0.17). For grade, the Kruskal-Wallis test showed no significant (p = 0.069) difference.
Discussion
The present study is the first Scandinavian survey on headache in adolescents in the general population to use the new ICHD-3 beta classification system (13). The prevalence of headache (88%) and definite or probable migraine (36%) was higher than in most previous epidemiological surveys (1). Nine percent of the adolescents fulfilled criteria for more than one headache type, with the most bothersome headache type having a longer duration and a higher intensity than the less bothersome headache type. Headaches reduced the daily activities of adolescents by about nine days a year.
The prevalence of definite migraine was much higher than the median (8%) reported in previous epidemiological studies (1). In addition most previous epidemiological studies have not taken into account PM in the total migraine prevalence, as is recommended by experts (17). By doing this, the total prevalence in our study becomes 36%. This approach is relevant considering the fact that the delineation between definite and PM is dependent on which version of the ICHD classification criteria is chosen. The definition of attack duration for definite migraine is stricter in the ICHD-3 beta criteria than in previous ICHD 2 diagnostic criteria (two to 72 hours vs one to 72 hours) (11). Depending on which one of these one uses, the ratio between definite and PM differs. In our material, 13 of the 64 adolescents (20%) with PM according to ICHD-3 beta would have had definite migraine if the ICHD-2 criteria (one to 72 hours) had been used. A similar exercise was performed in a sample of Hungarian schoolchildren. Depending on whether the authors applied more liberal pediatric migraine duration criteria (one to 72 hours) only to adolescents aged younger than 15 years (ICHD-1) or to all children/adolescents (as in ICHD-2 and ICHD-3 beta), the migraine prevalence was either 9.1% or 12.5% in the same material (18). Alternatively, our higher prevalence rate also may reflect a real increase in the prevalence of headaches in general, and of migraine in particular, as reported in a series of Finnish surveys covering several decades (1).
To our knowledge the point prevalence of headache in adolescents has earlier been investigated only in a Swedish sample aged 13–19 years (19), where 10% reported ongoing headache. In comparison, our value (38%) is high. One must then bear in mind that our question about current headache was given at the very end of an interview in school, which may have triggered episodic headache among some participants. Further we did not attempt to define a minimum cutoff on the scale to qualify as being headache and everything above zero was counted.
Contrary to most existing epidemiological studies, which have reported an increase in the prevalence of headache with age (4,16,20,21), the present study did not observe such a phenomenon. In a similar epidemiological survey of school children in Turkey (22), there was a decrease in the frequency of headache with age. In both the present study and the Turkish study, the questionnaires were supplemented with face-to-face interviews conducted by specially trained individuals to obtain important information on headache characteristics not extractible in surveys solely based on questionnaires.
The mean headache-related disability (PedMIDAS score 2.3 ± 4.4) was somewhat lower than estimates reported in previous general population-based studies (median 5, range 3–11) (4,16,20,21). Adolescents who suffered from migraine had substantially higher PedMIDAS scores than those suffering from TTH, findings in line with those reported by Lipton et al. (23). While our PedMIDAS scores were highest among adolescents with CM, they were comparable to those reported for children and adolescents without chronic headaches but substantially lower than among those with chronic headaches in a selected sample referred to a tertiary headache clinic (14).
High intensity and long duration were regarded by the adolescents as more bothersome characteristics than high frequency of headache, and this was evident both when they rated the most bothersome headache in the questionnaire and also when they were asked directly about their experiences with migraine. This is in line with results of a German study (24) in which children with different types of pain including headache regarded high intensity and long duration of pain as more annoying than high frequency of pain. In a Turkish study (25), the most sensitive headache characteristic of migraine was “severity of pain,” and the most sensitive definitive symptom for children with TTH was “duration of headache.” Overall, these findings have potential implications for interviews with young patients with headaches in school health care and clinics, and should be further investigated by qualitative methods.
The prevalence of chronic daily headache (CDH) of 2.8% is what would be expected based on earlier studies of CDH in this age group. In an American study from 2011 (23), the prevalence of CDH (last month) was 3.5% among 12- to 17-year-olds. In a study from Taiwan in 2006 (26), Wang et al. found that 1.5% of adolescents aged 12–14 years had primary CDH (without organic lesions) in the past year.
A limitation of the present study is the relatively small sample size leading to wide estimates of 95% CI for the less prevalent headache disorders such as MOH. A further limitation is that we did not achieve an ideal balance between urban and rural areas. This was an effect of the fact that consent to participation was more often given by the principals in the schools in the rural county. In addition there was a higher dropout rate among the students in the included schools in the city. A third limitation is that it was not possible to obtain information about the characteristics of non-participants and the reasons for non-participation because Norwegian law requires parental written consent for children younger than 16 years of age. Finally, there is a risk that offering an interview about headaches may have biased the sample to those with headaches.
A strength of the study was that the headache diagnosis was based on a thorough discussion with the participant in a face-to-face situation, where all the diagnostic symptoms could be determined, instead of solely relying on recognition-based (27–30) or self-considered diagnoses (29) as in earlier Scandinavian surveys. The interviews also made it possible to clarify the meaning and contents of the issues for those participants that had difficulties understanding them.
Conclusion
The majority of young adolescents experienced headaches, and they lost on average nine days of activity per year because of headaches, which disabled them in their daily life, thus constituting a major health problem. It is important to disseminate this information to school health care personnel so that they can identify headache in adolescents in its early stages and initiate or refer them for appropriate treatment.
Although our data on headache characteristics were obtained using standardized questionnaires and interviews, the outcomes of previous studies have suggested that the use of prospective paper and electronic diaries provide a more reliable picture of estimates of various headache features, although with somewhat inconsistent findings (9,31,32). Further validation of different assessment methods in this age group and comparisons between retrospective questionnaire/interview data and prospective diary data, preferably by the use of electronic diary formats, is recommended.
Clinical implications
This is the first epidemiological study applying the new diagnostic classification system of the International Headache Society (International Classification of Headache Disorders, third edition beta (ICHD-3 beta)) in a general population of adolescents. We found a very high prevalence rate of migraine. Intensity and duration of headache episodes rather than frequency seems to determine when adolescents regard headaches as most bothersome vs less bothersome.
Footnotes
Funding
This research received no specific grant from any funding agency in the public, commercial, or not-for-profit sectors.
Conflict of interest
None declared.
Acknowledgments
The authors express their gratitude to participating students, their directors and all staff of the 13 participating schools for their excellent cooperation and contribution to this study.
Further data from the underlying research material can be obtained upon request to the corresponding author.
Author participation includes: conception and design: B. Larsson, M. Linde; acquisition of data: AB. Krogh; analysis and interpretation of data: B. Larsson, M. Linde; drafting of the article: AB. Krogh, B. Larsson, M. Linde; revising it critically for important intellectual content: M. Linde, B. Larsson; giving final approval of the version to be submitted: M. Linde, B. Larsson.