
Abstract
Migraine is related to numerous factors such as hormones, stress or nutrition, but information about their actual importance is limited. Therefore, we analysed prospectively a wide spectrum of factors related to headache in migraineurs. We examined 327 migraineurs recruited via newspapers who kept a comprehensive diary for 3 months. Statistical analysis comprising 28 325 patient days and 116 dichotomous variables was based on the interval between two successive headache attacks. We calculated univariate Cox regression analyses and included covariables with a P-value of <0.05 in two stepwise multivariate Cox regression analyses, the first accounting for a correlation of the event times within a subject, the second stratified by the number of headache-free intervals. We performed similar analyses for the occurrence of migraine attacks and for the persistence of headache and migraine. Menstruation had the most prominent effect, increasing the hazard of occurrence or persistence of headache and migraine by up to 96%. All other factors changed the hazard by <35%. The two days before menstruation and muscle tension in the neck, psychic tension, tiredness, noise and odours on days before headache onset increased the hazard of headache or migraine, whereas days off, a divorced marriage, relaxation after stress, and consumption of beer decreased the hazard. In addition, three meteorological factors increased and two others decreased the hazard. In conclusion, menstruation is most important in increasing the risk of occurrence and persistence of headache and migraine. Other factors increase the risk less markedly or decrease the risk.
Introduction
Migraine is a paroxysmal neurological disorder affecting at least 10% of the general population (1, 2). It has a great impact on the lives of the affected individuals and exerts a burden in terms of pain, suffering and impaired quality of life (3). This imposes a large economic problem on society, particularly in terms of indirect costs due to lost work time and reduced productivity (4). Accordingly, migraine requires effective therapeutic management, including pharmacological and non-pharmacological treatment (1, 2, 5). The identification of trigger factors is frequentlyrecommended as a basic therapeutic strategy (6–9). Menstruation, environmental and psychological factors, sleep disturbance, tiredness, alcohol and nutrition are mentioned most often, but the actual impact of many trigger factors remains unclear (10, 11).
The vast majority of studies on trigger factors of migraine attacks is based on retrospectively recorded, subjective patient information. Accordingly, the validity of these data is reduced by recall bias, selective memory and the patients' need for causal explanations. Controlled studies are rare and restricted to single trigger factors such as menstruation, chocolate and alcohol (12–14). In one prospective study covering a period of 3 months, precipitating factors were reported for each headache period (15). However, the validity of this study was limited by recording only the patients' subjective explanations and disregarding the presence or absence of possible trigger factors on the days between headache attacks.
In addition, there is no comprehensive and systematic analysis clarifying whether conditions in everyday life such as environmental, physical or psychological factors, sleep or nutrition may prevent the occurrence of headache in migraineurs. Finally, it is unclear whether those factors have an impact on headache persistence.
The objective of the present study was therefore to examine prospectively a wide spectrum of factors related to migraine by means of a comprehensive diary filled in by the patients every night independent of the presence of headache. By applying sophisticated statistical analysis and considering the classification of each single headache attack, the aim was to identify factors which increase the risk of occurrence of headache in migraineurs as well as factors which decrease this risk. In addition, we wanted to identify factors increasing and decreasing the risk of headache persistence.
Patients and methods
Patients were recruited via articles about trigger factors of migraine in the two most popular newspapers in eastern Austria. In the articles, it was indicated that all patients completing the study would profit from participation by being provided with a detailed analysis of their individual data.
Inclusion criteria comprised written informed consent, age ≥18 years, a migraine frequency of at least one attack per month during the previous 6 months and a diagnosis of migraine without aura, migraine with aura or probable migraine (with or without coexisting tension-type headache) according to the criteria of the International Headache Society (IHS) (16).
Exclusion criteria were medication overuse, medication overuse headache, any other primary or secondary headache and clinically relevant other diseases.
Out of 446 persons who made an appointment, 31 subjects did not come for the first visit and 415 patients were screened for the fulfilment of the inclusion and exclusion criteria.
Biographical data, lifestyle, general medical history (Table 1) and headache characteristics were recorded in a semistructured interview. Eighteen subjects were excluded because of medication overuse (n = 12), pure tension-type headache (n = 3), cluster headache (n = 1) and refusal to participate in the study (n = 2); 397 patients were included. These patients were provided with a paper-pencil diary for 90 days.
Variables included in the analysis

Variables lagged, i.e. taken from the day before onset of headache.
The diary covered 52 items potentially related to migraine (Table 1). All items, except the specification of each day and hormonal factors, had to be assessed on a four-point scale or a quantity had to be given. In addition, the diary included questions regarding the presence of headache as well as all headache characteristics required for a diagnosis according to the IHS criteria. Apart from the patient-based variables, 29 meteorological factors were included, which were collected at the Central Institute of Meteorology and Geodynamics (Vienna, Austria). Beside single values such as air temperature, a synoptic weather classification was used (Table 1).
During the first visit every patient filled in a questionnaire identical to that in the diary. This questionnaire was checked by a member of the study group and discussed with the patient, if necessary. After the completion of the diary the patients were seen for the final visit to check the diary and clarify any unclear information.
Every single headache was classified according to the IHS criteria of migraine without aura (16). Headaches fulfilling none of the criteria B, C, and D, i.e. headache duration, headache characteristics and associated symptoms, were excluded from further analysis.
Statistical analysis
Data from 28 325 patient days were available for statistical analysis. The analysis was based on the interval between two successive headache attacks and on the interval between two successive migraine attacks. These had to fulfil the criteria of migraine without aura (IHS 1.1), typical aura with migraine headache (IHS 1.2.1) or probable migraine without aura (IHS 1.6.1) treated or untreated. The analysis of headache attacks was based on 20 831 patient days and that restricted to migraine attacks on 22 942 patient days. Each interval started on the second day after a headache attack and ended on the day of the following attack. Days 2+ of a headache attack were not included in the analysis and the number of days was larger in the migraine analysis, as the interval from one migraine attack to the next comprised days without headache as well as days with non-migrainous headache. The first day without headache was excluded from statistical analyses, since on this day the risk of headache and migraine was per definition 0 and covariates could have been influenced by the headache the day before (17). For evaluating the hazard of occurrence of headache and migraine we performed univariate Cox regression analyses and a stepwise multivariate Cox regression analysis including those covariables which showed a P-value of 0.05 in the univariate procedure. The stepwise model selection was based on the Akaike Information Criterion, which can include factors that have a multivariate P-value slightly larger than 0.05. P-values from the univariate and multivariate analysis were according to the robust Wald test, which accounts for correlations between event times within subjects by jack-knife estimation of the standard errors of the hazard ratios. There was a design-specific negative correlation between the length and the number of headache-free intervals. This could lead to an overestimation of hazard ratios in the analyses. Hence, a confirmatory stepwise multivariate Cox regression analysis with patients stratified by the number of headache-free intervals (classified into five approximately equally large strata) was performed.
To increase further the robustness of the analyses and to exclude an interaction with headache, 45 variables were lagged, i.e. they were taken from the day before onset of headache (Table 1).
All continuous covariables were categorized in either two or three approximately equally large classes (leading to either a single or two dichotomous covariables). In total, 116 dichotomous covariables were investigated.
A similar statistical analysis was performed for the persistence of headache and migraine attacks. Persistence was defined as presence of headache or migraine on at least two subsequent days. The analysis including headache attacks was based on 6927 patient days, that restricted to migraine attacks comprised 4466 patient days. All analyses were performed with the statistical software package R.
Results
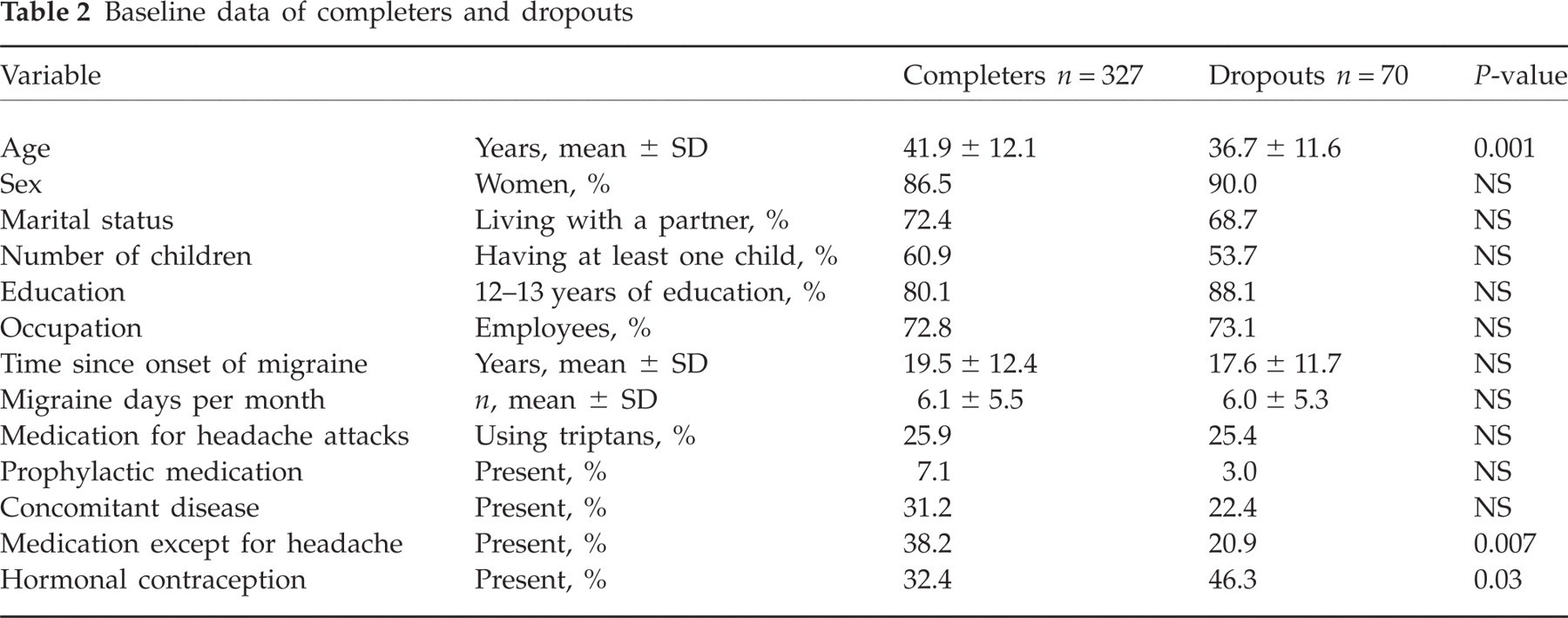
Three hundred and twenty-seven patients (82.4%) returned the diary. On average, the diary was kept for 86.6 ± 12.1 days. A comparison between completers and dropouts is given in Table 2.
Baseline data of completers and dropouts
Of 28 325 patient days, there were 8648 days with headache. Headaches fulfilling none of the criteria B, C and D of the IHS criteria of migraine without aura occurred on 1620 days and were not included in the statistical analyses. Migraine without aura was present on 2096 days, probable migraine on 2459 days and non-migrainous headache (fulfilling only one of the IHS criteria B, C and D) on 2473 days. Aura symptoms occurred on 839 days.
Acute headache medication was used on 57.6% of the 7028 analysed headache days, i.e. on 4047 days. Analgesics were taken on 2684 days, triptans on 1035 days, ergotamines on 542 days and antiemetics on 117 days. On 323 days the patients took more than one type of medication.
Details regarding the frequency and (semi)quantitative assessment of factors potentially related to migraine attacks are given in Tables 3 and 4. During the study period 47 of 52 factors (90%) were present in >75% of the patients and 28 factors (54%) were present on >25% of the days.
Frequency and semiquantitative assessment of factors potentially related to migraine attacks, data from 28 325 patient-days

Factor rated >0 on at least 1 day.
Frequency and quantitative assessment of factors potentially related to migraine attacks, data from 28 325 patient-days

Present on at least 1 day.
HA, Headache.
The hazard of headache occurrence was increased by all days of menstruation and by the 2 days before menstruation, as well as by muscle tension in the neck and tiredness on the day before headache onset, whereas the hazard was decreased by a small pressure gradient, holidays or days off and a maximum atmospheric pressure of >1000.1 hPa. The detailed findings and the findings of the analysis restricted to migraine attacks are summarized in Table 5. The hazard ratios give the ratio by which the hazard for occurrence of headache is increased (hazard ratio >1) or decreased (hazard ratio <1). All factors given in Table 5 reached statistical significance in both multivariate analyses. Hence there is strong evidence for an influence of these factors.
Factors influencing the occurrence of headache and migraine attacks

All variables were statistically significant in both multivariate analyses.
Variable lagged, i.e. taken from the day before onset of headache.
Max. AP, Maximum atmospheric pressure.
Table 6 gives the factors which showed statistical significance in the first multivariate analysis but not in the second confirmatory analysis. Most of these factors had P-values >0.01. An exception was the group of 110 patients with <3 h of sport per month, which had a significantly increased risk for a headache attack in the first analysis. The lack of statistical significance in the stratified analysis was due to a correlation between hours of sport per month and the stratification factor, in which case the stratified analysis is less powerful.
Further factors influencing the occurrence of headache and migraine attacks
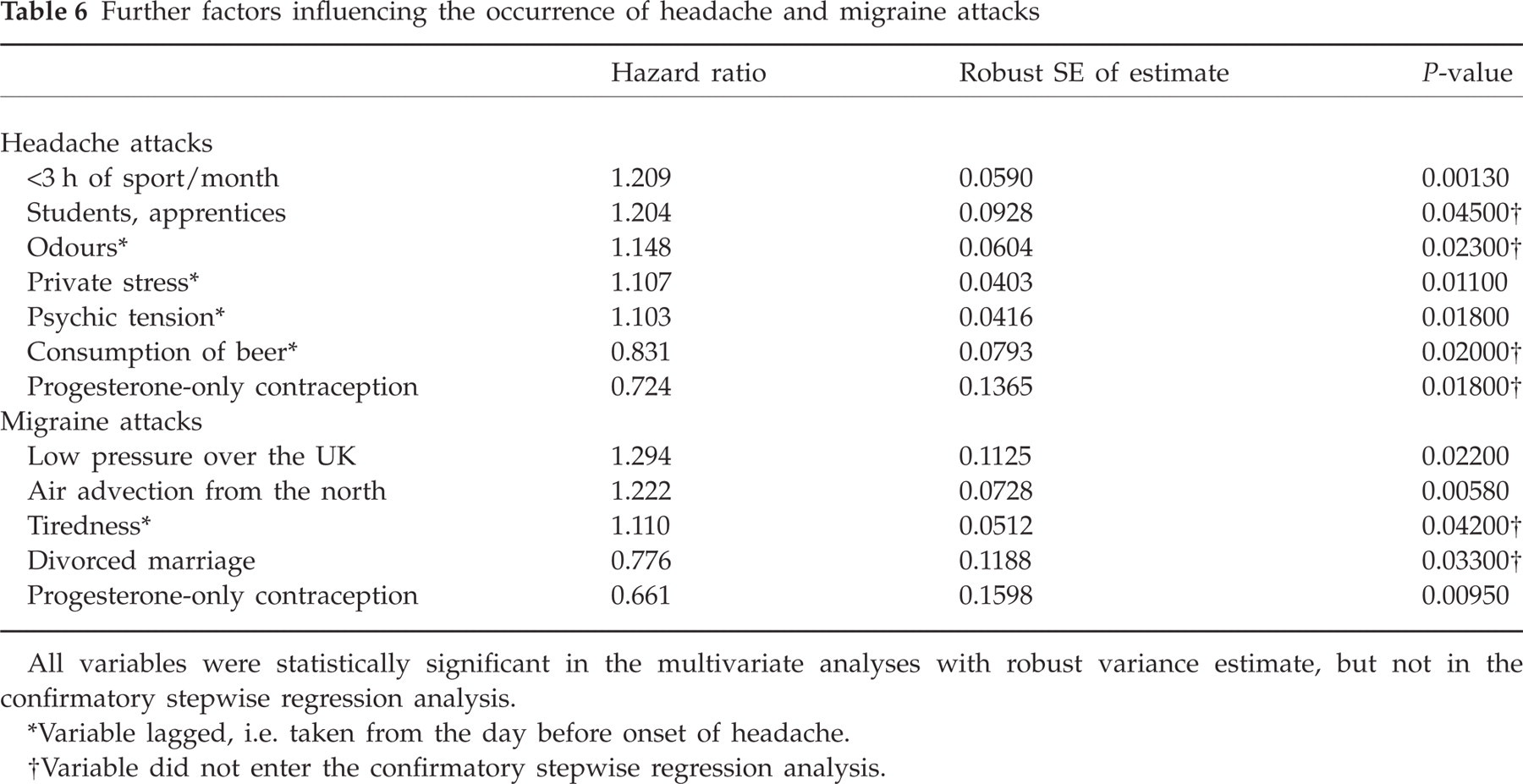
All variables were statistically significant in the multivariate analyses with robust variance estimate, but not in the confirmatory stepwise regression analysis.
Variable lagged, i.e. taken from the day before onset of headache.
Variable did not enter the confirmatory stepwise regression analysis.
Table 7 gives details of the multivariate analyses of factors affecting the persistence of headache and migraine. Factors which increased the risk of persistence had hazard ratios <1 (as they decreased the ‘hazard’ of ending the attack). In addition to the factors given in Table 7, the risk of persistence of a headache attack was decreased in patients with a university degree (hazard ratio 1.14, P = 0.045), but this factor missed the level of statistical significance in the confirmatory regression analysis.
Factors influencing the persistence of headache and migraine attacks

All variables were statistically significant in both multivariate analyses.
HA, Headache.
Variable lagged, i.e. taken from the day before onset of headache.
Discussion
This prospective study provides the first comprehensive and systematic information about the importance of a wide spectrum of factors related to the occurrence and persistence of headache in migraineurs. Based on the data of 28 325 patient days, we applied a sophisticated statistical analysis considering the classification of each single headache attack.
We found strong evidence that in migraineurs the risk of occurrence of a headache attack was increased by all days of menstruation, the 2 days preceding menstruation as well as by <3 h of sport per month and by muscle tension in the neck and tiredness on days before headache onset. The analysis restricted to migraine attacks showed that menstruation, muscle tension and tiredness remained statistically significant and that psychic tension on days before headache onset as well as a daily sunshine duration of >3 h gained significance.
The evidence for decreasing the risk of a headache attack was best for holidays and days off, an atmospheric pressure of >1000.1 hPa, and a small pressure gradient. Similarly, the risk of a migraine attack was reduced on holidays and days off. In addition, this risk was reduced on Tuesdays and, surprisingly, on days following the consumption of beer.
Several other factors tended to influence the risk of a headache or migraine attack, but missed statistical significance in the confirmatory multivariate analysis. These factors comprised private stress and odours on days before headache onset, low pressure over the UK and air advection from the north. In addition, the risk of headache occurrence tended to be increased in students and apprentices. Factors which tended to decrease the risk of headache or migraine were progesterone-only contraception and a divorced marriage.
The risk of persistence of headache or migraine was increased by menstruation, sick days not due to headache, concomitant diseases, and noise, odours, muscle tension in the neck and physical exhaustion on days before headache onset. In contrast, a divorced marriage, relaxation after stress, holidays and days off and consumption of beer had a favourable effect. A reduction in the risk of headache persistence was also seen in patients with a university degree.
Statistical analysis
Statistical analysis of the type of data in this study, i.e. recurrent event data, is in general not an easy task and is still under statistical scientific investigation (18, 19). No off-the-shelf solution is available yet. The models chosen in this paper have the following advantages. First, they allow analysing all recurrent headache data of the patients. (A less complicated but also less efficient approach would consider the time until the first headache attack and the duration of the first headache interval. This would ignore a large amount of data.) Second, they allow accounting for time-varying covariates. Third, they account for censoring due to the 90-day study window and other independent dropout. (No other model class than the survival models could account for such censoring.) Fourth, using the robust variance estimate accounts for the correlation of event times of the same subject when estimating the standard errors. The confirmatory analysis with strata based on the number of headache intervals per patient was done to see whether the significant factors found in the main model are mainly driven by few patients with a large number of intervals. Factors that do not rely on few patients with a large number of intervals should be significant also in the stratified model.
Classification of headache attacks
A detailed headache diary allowed to classify each single headache attack and to differentiate headaches with and without features of a migraine attack. Considering the overlap between migraine and tension-type headache (20, 21), we excluded headaches fulfilling not one IHS criterion of migraine without aura and we performed two separate analyses for all other headaches. The first analysis included headaches fulfilling at least one IHS criterion of migraine without aura, i.e. definite migraine attacks, migraine attacks fulfilling all but one IHS criterion of migraine without aura and tension-type headache with migrainous features. The second analysis included only headaches classified as migraine without aura (IHS 1.1, 1.2.1, 1.6.1) treated or untreated. This strategy provided an optimum of information and prevented restrictive, highly selective inclusion criteria not reflecting the conditions of everyday life.
Menstruation and other hormonal factors
Menstruation was the most important risk factor for the occurrence and persistence of headache and migraine. The 2 days before menstruation increased only the risk of headache in general, but not that of migraine attacks, and had no impact on the persistence of headache and migraine.
The importance of menstruation has been frequently described (11, 12, 22), but the present study confirmed this prominent role for the first time prospectively within the context of multiple other factors.
In contrast to menstruation, progesterone-only contraception used by 11 women only had a favourable influence, reducing the risk of occurrence of headache and migraine. The favourable effect might be explained by the absence of menstruation in these women. Colson et al. (23) have reported that variants of steroid hormone receptor genes increase the risk of migraine, but evidence for the use of hormonal treatments in migraine is still poor (24).
Muscle tension in the neck
Virtually all patients experienced muscle tension in the neck and at least mild tension was present on >50% of the patient days. Muscle tension on a day before headache onset decreased the interval between the impending attack and the following one and increased the risk of headache persistence. In a paper on premonitory symptoms of migraine by Giffin et al. (25), a stiff neck was present before, during and after the headache phase, suggesting that neck complaints are a symptom and not a trigger of migraine attacks. Neurophysiological studies indicate a dynamic trigemino-cervical interaction with neuroplastic changes based on convergence of trigemino-cervical afferents and central sensitization of trigemino-cervical neurons and have prompted therapeutic studies using neurostimulation of afferent nerves (26). The question whether neck complaints are exclusively a symptom of migraine attacks or whether they may also act as a trigger cannot be answered definitely. The clinical evidence from the present investigation and from the paper by Giffin et al. (25), however, calls for further studies on therapies targeting the cervical portion of the trigemino-cervical pathways.
Tiredness, mental exhaustion, and sleep-related factors
The proportion of days with tiredness reached almost 60%. Restless sleep and sleeping for too short a time were present on approximately 35% of the patient days, whereas mental exhaustion and sleeping too long occurred less often. The effect of these factors on the occurrence and persistence of headache and migraine was limited. Only tiredness increased the risk of headache and migraine. No other factor had an influence. In the study on premonitory symptoms (25), tiredness was by far the most common symptom before, during and after the headache phase. Similar to muscle tension, the role of tiredness as a trigger factor of an attack may be questioned, but the occurrence of tiredness before headache may offer a chance for the prevention of attacks.
The relation between sleep and migraine is reciprocal. On the one hand, sleep problems are frequently cited as a trigger factor, on the other hand, migraine attacks starting during night and interfering with sleep were reported by >70% of patients in a large clinical sample of migraineurs (11, 15, 27, 28). Polysomnographic recordings showed differences between nights preceding a migraine attack and nights without a following attack (29). The lack of a statistically significant role of sleep problems in the present study can be explained by the study design. The variables were lagged, i.e. taken from the day before headache onset to exclude an interaction with headache. Accordingly, our analysis did not include nights immediately preceding an attack.
Psychological factors
Psychic tension, irritation, private stress, stress at work and relaxation after stress occurred on 27–45% of the days, joy was present on almost 2 of 3 days. For statistical analysis, all variables were lagged. Psychic tension and private stress increased the risk of headache or migraine, whereas relaxation after stress decreased the risk of persistence of headache and migraine, but did not influence their occurrence. Accordingly, our study does not suggest that relaxation after stress is a relevant trigger factor (11).
Indirect evidence for the impact of stress is the favourable influence of holidays and days off on the occurrence as well as persistence of headache and migraine. Other indirect evidence for the impact of stress may be the favourable effect of a divorced marriage.
Meteorological factors
The detailed meteorological data are not presented in this paper. Statistical analysis provided strong evidence that certain meteorological factors have an effect on the occurrence, but not on the persistence of headache and migraine. The majority of previous studies have focused on the unfavourable consequences of the ‘weather’ on health in general and headache or migraine in particular (11, 30, 31). Beneficial effects have been widely ignored. The present study indicates unfavourable as well as favourable effects on headache and migraine. A daily sunshine duration of ≥3 h, low pressure over the UK and air advection from the north increased the risk of migraine, whereas a small pressure gradient and a maximum atmospheric pressure of >1000.1 hPa decreased the risk of headache.
External sensory stimuli
Surprisingly, external stimuli were cited rather infrequently by the patients in this study. Noise was given most often (on 18% of the days), followed by odours, bright light and a disturbing air condition. Odours and noise (on days before headache onset) increased the risk of occurrence and persistence of headache or migraine, whereas bright lights and air condition did not change the risk. Studies comparing migraine with and without aura suggest that sensory stimuli are more important in aura patients (11, 32). In the present study, a separate analysis of migraine aura was not performed.
Nutritional factors
Alcoholic beverages were consumed on 7–10% of days by 60–80% of patients. Red wine was the most popular alcoholic beverage. Cheese and chocolate were consumed by virtually all patients, every other day on average. In contrast to previous reports (10), not one nutritional factor had an unfavourable impact. Surprisingly, the consumption of beer on days before headache onset even reduced the risk of headache and migraine as well as the risk of headache persistence. To elucidate this unexpected finding, further studies are necessary.
Our study provides evidence for the limited importance of nutrition in the precipitation of migraine. However, we did not record whether patients had stopped consuming alcoholic beverages or certain foods considering they could trigger migraine attacks. In addition, factors triggering attacks inconsistently in a small number of patients might have been missed by our analysis.
Further factors
Among biographical factors, marital status had the most prominent influence regarding the favourable effect of a divorced marriage discussed above. Apart from that, education and occupation tended to change the risk. The finding that lack of physical activity increased the risk of headache correlates indirectly with a study showing that aerobic exercise is effective in preventing migraine without aura (33). The negative impact of concomitant diseases is supported by studies on the comorbidity of migraine (34). Regarding the favourable effect of Tuesdays, we can offer no explanation. The absence of any other relation between weekdays and headache or migraine suggests that ‘weekend migraine’ (11) does not play a prominent role.
Limitations of the study
The findings of this study may be limited by the fact that we recruited patients via articles in newspapers. However, we believe that this was the most useful way of patient recruitment, avoiding on the one hand the selected group of patients of a tertiary care centre and promising, on the other hand, sufficient compliance in completing a comprehensive diary over a period of 3 months. We cannot exclude that patients in our study had certain beliefs in trigger factors, but considering the large number of trigger factors, the large number of patients and the fact that the vast majority of variables analysed were objective or quantitative (and not subjective), we see no relevant bias. On the contrary, the patients were motivated to gain reliable information about the actual, individual importance of trigger factors (and all patients were provided with an evaluation of their personal data).
Conclusion
This comprehensive, prospective study on the importance of a wide spectrum of factors possibly related to the occurrence and persistence of headache in migraineurs indicates that menstruation has a prominent unfavourable role, increasing the risk of occurrence and persistence of headache or migraine by up to 96%. Other factors change the risk of occurrence or persistence of headache or migraine by <35%. The statistical evidence for an unfavourable effect is strong for muscle tension in the neck, psychic tension, tiredness, noise, odours and physical exhaustion on days before headache onset as well as for the 2 days before menstruation, sick days not due to headache, concomitant diseases and lack of physical activity. The statistical evidence for a favourable effect is strong for holidays and days off, a divorced marriage, consumption of beer, relaxation after stress, and Tuesdays. Finally, our study clearly indicates that the risk of getting headache and migraine can be increased as well as decreased by certain meteorological factors. Our findings improve markedly the knowledge about trigger factors of migraine, provide additional information regarding headache persistence and will have consequences for the management of migraine, including patient education.
Acknowledgements
This study was supported by a grant from Pfizer Corporation Austria. Additional support was provided by AstraZeneca, GlaxoSmithKline and Sanofi-Synthelabo.