
Abstract
The aim of the present study was to identify trigger factors in migraine with aura (MA). A total of 629 MA patients representative of the Danish population were sent a questionnaire listing 16 trigger factors thought to be relevant as well as space for free text. Distinction was made between attacks with or without aura within each patient. The questionnaire was returned by 522 patients of whom 347 had current MA attacks. In total 80% with current attacks (278/347) indicated that at least one factor triggered their migraine, and 67% (187/278) in this group indicated that they were aware of at least one factor often or always giving rise to an attack of MA. Forty-one per cent (113/278) had co-occurring attacks of migraine without aura (MO). Stress (following stress), bright light, intense emotional influences, stress (during stress) and sleeping too much or too little were the trigger factors mentioned by most. Attack frequency had little impact on the number of trigger factors. Women reported more trigger factors than men. Patients having attacks of both MA and MO reported more trigger factors for MO attacks than for MA attacks. In conclusion, 80% of patients with MA reported trigger factors and two-thirds of these reported at least one trigger factor often or always triggering an attack of MA. Patients should be educated to avoid these factors.
Introduction
‘Triggers are factors that, alone or in combination, induce headache in susceptible individuals’ (1). Many studies have identified a great number of different trigger factors in migraine. Most of these studies have focused mainly on migraine as a whole or migraine without aura (MO) (2–13). Few studies have analysed trigger factors separately for patients with migraine with aura (MA) and patients with MO (14–17). Recently a study by Kelman (14) reporting on a large material of patients showed significant differences between trigger factors in patients with MA and MO. Further investigation of the MA subgroup of patients in relation to trigger factors is relevant and might contribute to our knowledge about the aetiology and pathophysiology separating MA from MO. Such knowledge is also important for improved advice to patients.
The aim of the present study was to identify trigger factors in MA and to distinguish between trigger factors for MA and MO attacks in patients with both MA and MO. Further, the aim was to identify MA patients who were aware of triggers that often or always induced attacks. We drew upon a large representative series of patients diagnosed by a semi-structured validated interview. No other study has to our knowledge examined trigger factors in MA patients from the general population in an equally systematic way or in such a large material.
Material
Our material comprised 629 patients diagnosed with MA according to the International Classification of Headache Disorders 2nd Edition (18). All patients were identified in an earlier study (19,20). They were recruited from the entire Danish population and two search strategies were used: extraction of patients from the National Patient Register and screening of case records (Figure 1). From the National Patient Register of all hospitalized patients we extracted patients who had been admitted to hospital or seen as outpatients at a department of neurology or paediatrics in any Danish hospital in the years 1994–1997 and who were discharged with a diagnosis of MA or migraine with complication (ICD 10 diagnosis DG431 or DG433). Additionally, more than 27 000 case records were screened. About 6000 of these came from two headache clinics and a SPECT-scanning clinic, whereas 21 000 case records were from practising neurologists. A total of 1831 patients were recruited: 1101 from the National Patient Register and 730 from case records. Of the 1831 patients, 85 were non-contactable and 381 did not participate. A total of 1365 patients took part in an initial screening interview and it was found that 128 patients had hemiplegic migraine, 980 had non-hemiplegic MA and 257 did not have any kind of migraine. Among the 980 patients with non-hemiplegic MA and their relatives, 629 were diagnosed according to the International Classification of Headache Disorders 2nd Edition using a semi-structured validated extensive telephone interview (21) conducted by a physician or trained medical student and these patients were included in the present study (Figure 1). The interviews took place from 1999 to 2002 and from 2005 to 2006. The project was approved by the Danish Ethical Committee.
Ascertainment of patients with MA.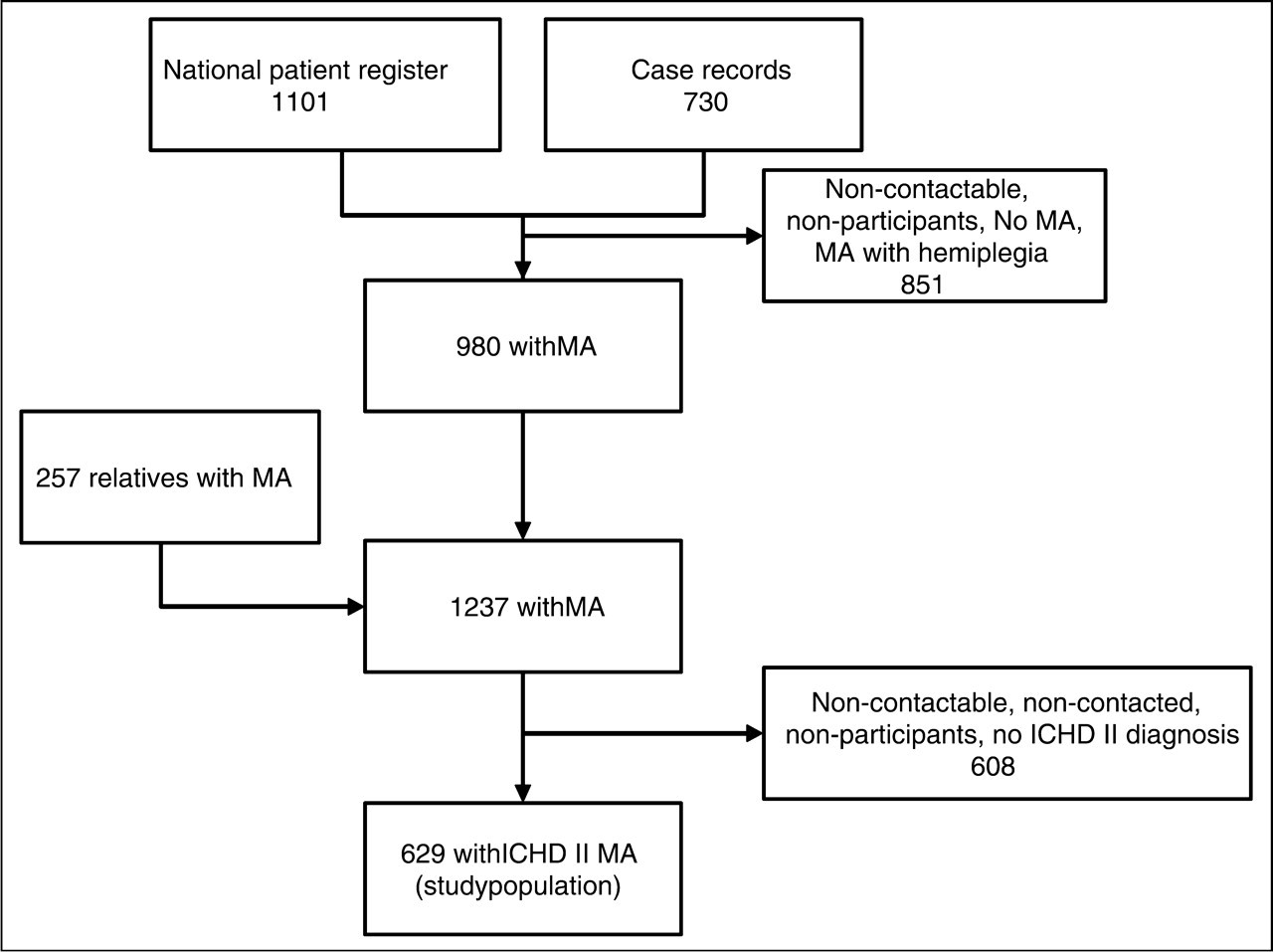
Methods
Data
Six hundred and twenty-nine patients were mailed a questionnaire regarding trigger factors (Figure 2). Those not responding within 1 month were mailed a reminding letter.
Questionnaire regarding trigger factors for migraine.
The questionnaire consisted of 16 listed trigger factors (Figure 2), and participants were asked to grade these factors on a 5-point scale depending on their likelihood to precipitate an attack of MA or MO (0 = never, 1 = infrequent, 2 = approximately half of the time, 3 = often and 4 = always). It was possible to add up to three additional trigger factors and grade them as well. Participants were asked to state their current frequency of attacks of MA and MO per month.
Statistical analyses
The χ2 test, Spearman's correlation, Wilcoxon signed rank sum test, Mann Whitney U or McNemar were used as appropriate. All P-values are two-sided. P < 0.05 was considered significant. Statistical analyses were performed using
Results
The response rate was 83% (522/629). Overall 71% (369/522) of patients reported at least one trigger factor. A total of 347 patients had current attacks of MA (at least one attack within the last year) whereas 126 patients had had no attacks for a year or more (no attacks). A combination of attacks of MA and MO (and minimum 1 trigger factor for both types of attacks) was reported by 22% (113/522) (Figure 3). Table 1 shows age, frequency of MA and MO and number of years since onset of MA. No statistically significant difference was found in age between the groups with current attacks and no attacks (P = 0.86) nor in the duration of MA (P = 0.71).
Study population. Clinical characteristics of the patients MA, migraine with aura. MO, migraine without aura. Current attacks, one or more attacks within the last year. No attacks, no attacks within the last year.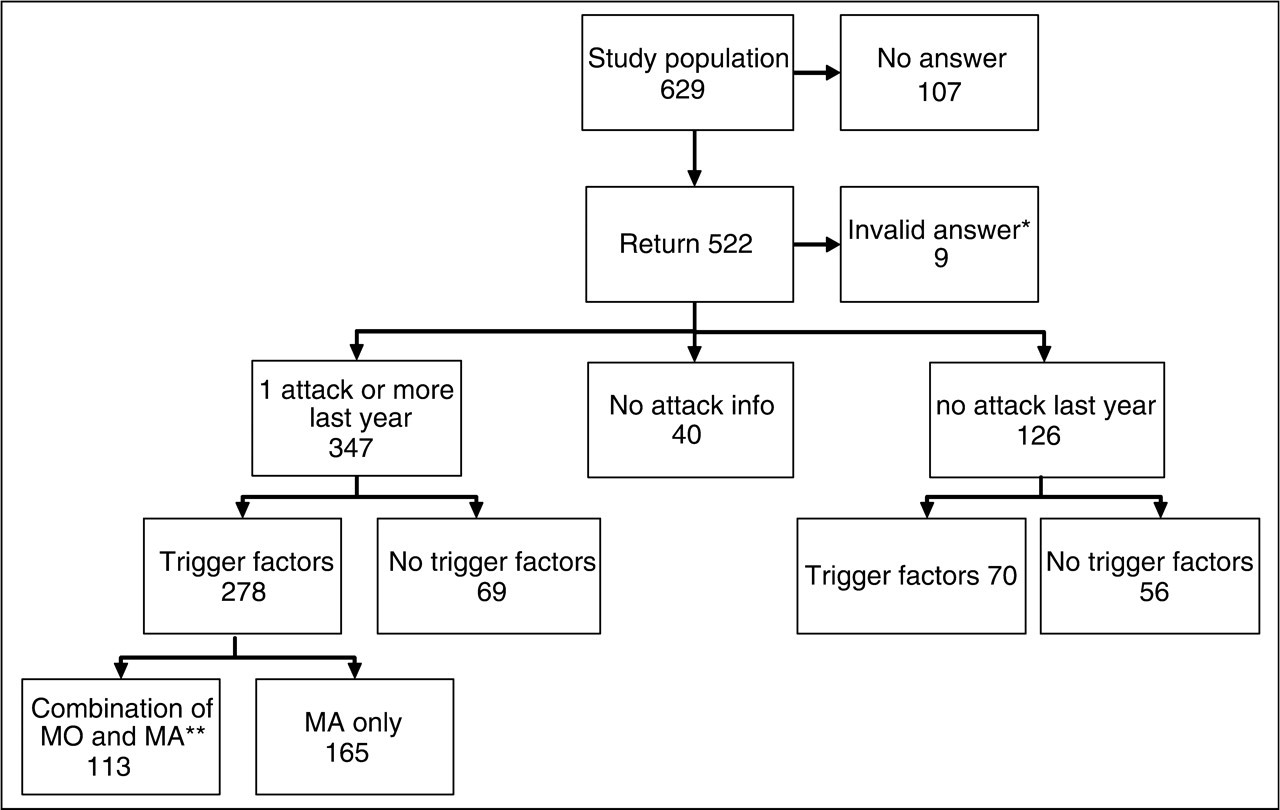

Of patients with current attacks, 80% (278/347) reported one or more trigger factors. Among participants with no attacks for the last year, only 56% (70/126) reported one or more trigger factors (P < 0.001). Because of this difference and the well-known tendency to forget about previous attacks, the rest of this paper focuses on the patients with current attacks.
The median number of trigger factors was five (range 1–17) (Figure 4) A total of 67% (187/278) of patients reporting trigger factors reported at least one trigger factor that often or always precipitated an attack of MA. Thirty-two per cent (90/278) reported a trigger factor that always could precipitate an attack.
Percentage of patients according to the number of factors triggering an attack of migraine with aura (n = 278). Patients not indicating a trigger are not included.
Individual trigger factors
Relaxation after stress was a trigger factor in 70% (194/278) of participants, followed by sunlight or other bright light in 61% (169/278), intense emotional influences in 59% (164/278), acute stress (during stress) in 58% (161/278), and sleeping too much or to little in 57% (158/278) (Figure 5). ‘Other factors’ mentioned by more than five patients were hunger/missing a meal (n = 11), dehydration (n = 10), tension in neck muscles (n = 9), noise (n = 7), and wind/draught (n = 7).
Number of patients reporting each individual trigger factor (n = 278). Grey bars indicate the total number of patients who have reported the individual trigger. Black bars indicate the number of patients who have indicated that the specific trigger factor often or always triggers an attack.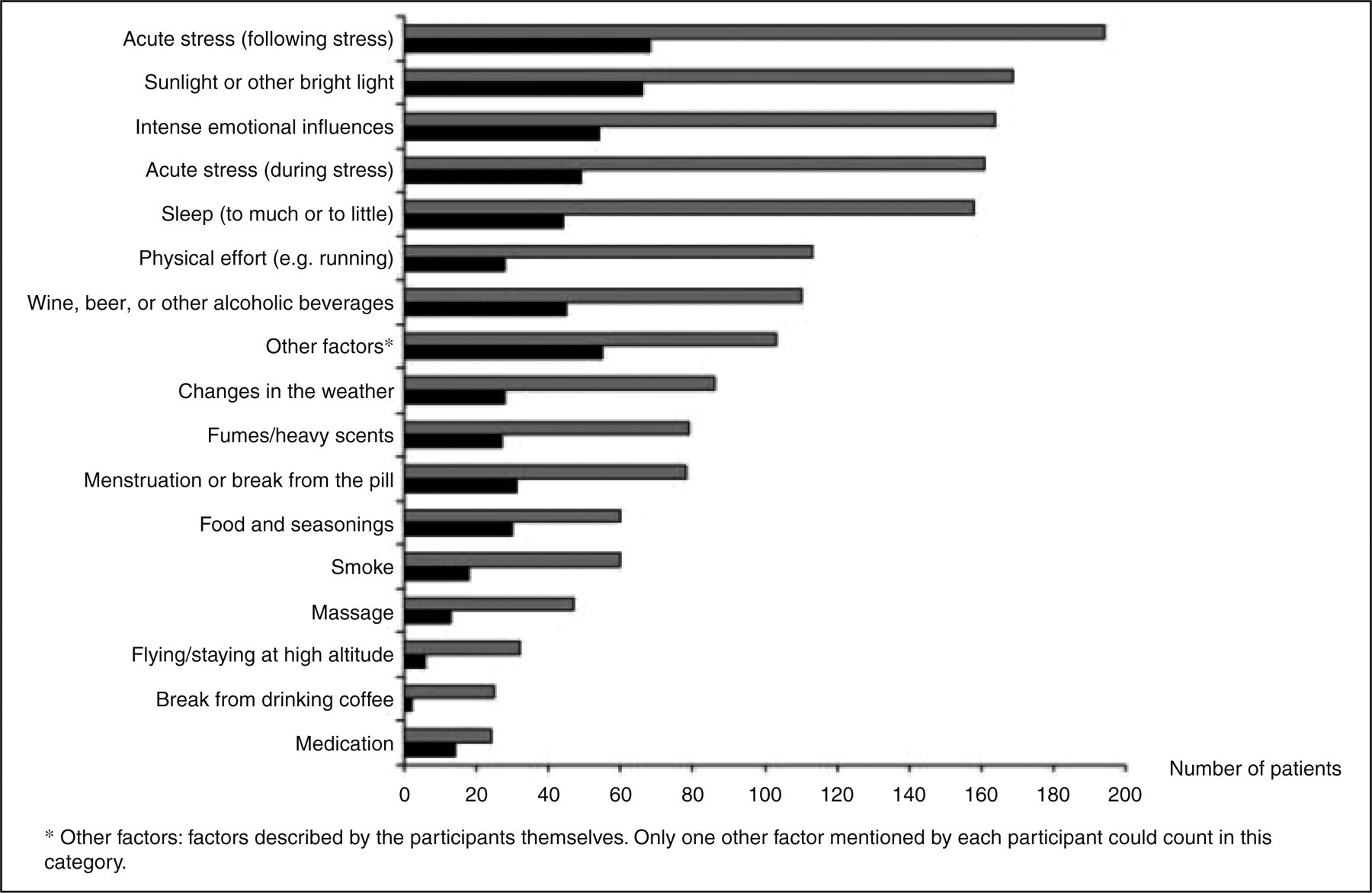
Correlations and group comparisons
Number of trigger factors was positively correlated with frequency of MA attacks (P < 0.01), but the correlation accounted for only 6% of the variability of the data. There was no correlation between age and number of trigger factors (P < 0.10) or between MA duration and number of trigger factors (P < 0.48). We found no statistically significant difference in number of attacks of MA between men and women (P < 0.39). If all trigger factors were included, the median number of trigger factors was greater in women than in men (P < 0.03) (Figure 6). If ‘menstruation or break from the pill’ were excluded no statistically significant difference was found. For patients having both MA and MO attacks, the number of MO trigger factors was positively correlated with frequency of MO attacks (P < 0.01). The correlation accounted for 12% of the variability of the data. Patients having MA attacks only reported the same number of trigger factors for MA attacks as patients having MA and MO attacks in combination (P < 0.63).
Correlation between number of attacks of migraine with aura and the number of trigger factors per participant according to sex.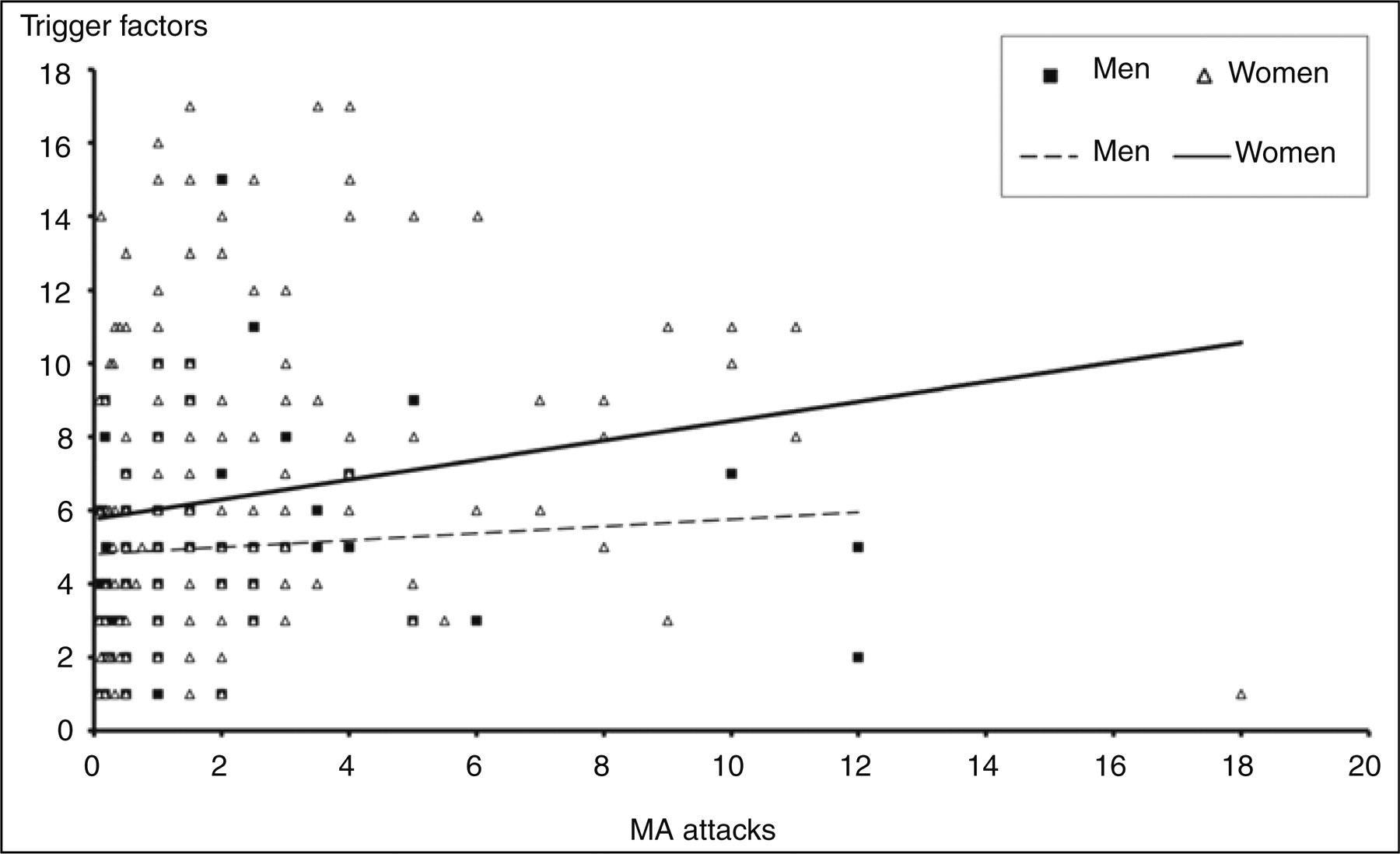
Within-subject analysis
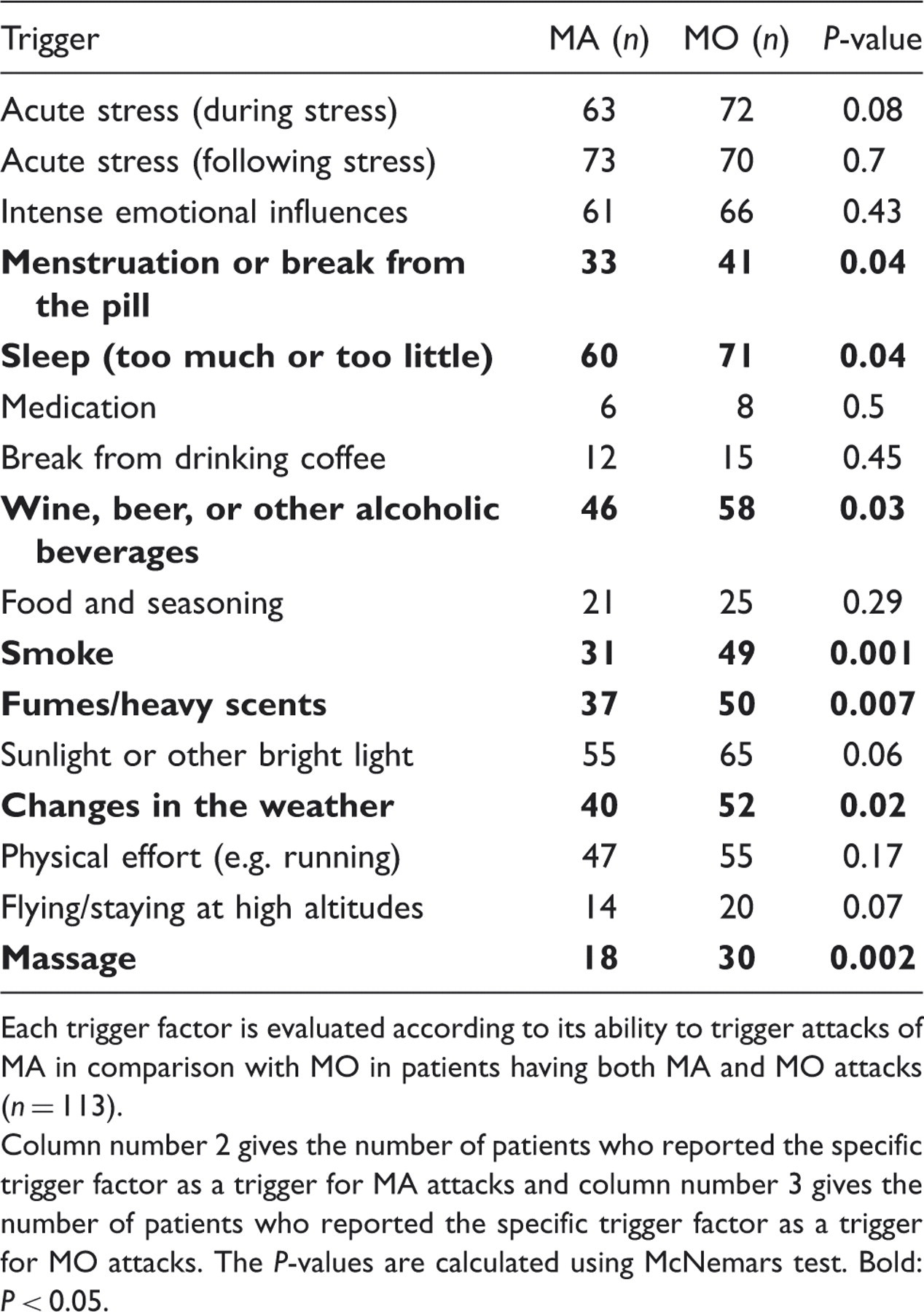
Patients reporting trigger factors for both MA and MO and with a status of current attacks of both types of migraine had a significantly higher number of trigger factors for MO (median 7, range 1–17) than for MA (median 6, range 1–17) (P < 0.001) (Figure 7). Comparisons of the individual trigger factors for attacks of MA and MO are shown in Table 2.
Correlation between number of attacks of migraine with aura (MA) or migraine without aura (MO) and the number of trigger factors per participant. Comparison of individual trigger factors in attacks of migraine with aura (MA) and migraine without aura (MO) Each trigger factor is evaluated according to its ability to trigger attacks of MA in comparison with MO in patients having both MA and MO attacks (n = 113). Column number 2 gives the number of patients who reported the specific trigger factor as a trigger for MA attacks and column number 3 gives the number of patients who reported the specific trigger factor as a trigger for MO attacks. The P-values are calculated using McNemars test. Bold: P < 0.05.
Discussion
The present study in patients with MA showed a high number of factors that triggered attacks. More importantly, the number of trigger factors that were reported to often or always precipitate an attack of MA was very high.
Our study has a number of advantages over previous studies. It deals with a relatively representative sample of patients. The aura was diagnosed using a validated semi-structured interview conducted by physicians and trained medical students. The sample size was large, allowing analysis of subgroups and of correlations to a number of variables. We used a specially designed questionnaire to record the trigger factors for MA and MO separately, making it possible to compare trigger factors within migraine patients having both types of attacks.
Stress has almost consistently been reported as the most frequent trigger factor for MA (15–17,22), MO (17,22), and migraine overall (8,10,12,14,23). Our study was no exception but we distinguished between occurrence during stress (triggered migraine in 59% of patients) and occurrence after stress (triggered migraine in 70%). Apart from the consistency of this one factor, other trigger factors have been more variably reported. In the present study sunlight and other strong light was the second most reported trigger factor. Two studies discriminating between MA and MO patients but not between MA and MO attacks (15,16) also found stress and bright light as the most frequent trigger factors although their percentages were somewhat lower than ours (34.2%, 28%). This difference might at least in part be explained by the fact that our study only used patients who currently (during the last year) had attacks, because these patients reported a statistically significantly higher number of trigger factors than patients who did not have attacks. A study by Zivadinov et al. (17) also discriminating between MA and MO patients is not suitable for comparison in this respect because flickering light was reported together with noise in a group called afferent stimulation.
Hormonal changes are often mentioned as very frequent triggers but were only reported by 36% of the women in our study. This is in agreement with previous population-based epidemiological studies showing that hormonal relations are much more common in MO than in MA patients (13,14,17). Our material also showed a much lower frequency of weather changes as a trigger factor for MA attacks compared with other studies looking at migraine patients and not MA and MO attacks separately (8,10,13,14).
Patients having attacks of both MA and MO reported more trigger factors for MO attacks than for MA attacks. Patients with many MA attacks had only slightly more prevalent trigger factors than patients with fewer attacks. The correlation showed statistical significance but could only explain 6% of the variability of data. Neither age nor time since onset of MA had any correlation with number of trigger factors. Women reported significantly more triggers than men but when hormonal triggers were left out there was no statistically significant difference.
Although our study recorded trigger factors in patients with currently active migraine in a systematic fashion even better data might have been obtained if patients had kept a diary of trigger factors. That, on the other hand, would have led to less representation because of many drop-outs. Trying to minimize recall-bias we have excluded those patients who did not have current attacks, because we found a big difference in number of reported trigger factors between patients having current attacks and those who had not. Prospective studies, where the patients, who have indicated factors that often or always could cause an attack of MA, keep a diary of trigger factors could supplement the present study. A diary could also include information regarding the time span from the exposure of the trigger factor to the onset of the migraine attack as well as specific information regarding the trigger factor. This information is essential when planning future pathophysiological studies examining migraine patients during triggered attacks and will be included in a future study.
Our study did not record how many attacks are precipitated by exposition to a trigger factor, but another study has shown that this may be as high as 76% (14). In the present study 67% of patients reporting trigger factors indicated at least one trigger factor that often or always precipitated an attack of MA, suggesting that avoidance of these specific factors could lead to a substantial reduction of attacks.
Another aspect of trigger factors is to identify patients whose attacks can be precipitated in research studies. Studies of such patients have already proven extremely useful (24). If a number of patients can be identified, who reliably can precipitate their aura, then the study of such patients may lead to increased understanding of the mechanisms of MA.
In conclusion, 80% of MA patients reported one or more trigger factors and two-thirds of these reported at least one trigger factor that often or always precipitates an attack of MA. Because we have no acute treatment for the aura-phase of an attack of MA, educating patients to pay attention to and avoid these factors is a particularly important part of their treatment.