
Abstract
Aims: Weather is mentioned as a trigger factor by migraine patients most frequently. We examined the impact of meteorological factors and the impact of their day-to-day change on the risk of occurrence and persistence of headache and migraine and the correlation of subjective weather perception with objective weather data.
Methods: We performed a prospective, diary-based cohort study in 238 patients suffering from migraine with or without aura. Patients had to live within 25 km of the Vienna meteorological station and were required to keep a diary for 90 days. We analysed 11 meteorological parameters and 17 synoptic weather situations. For evaluating the hazard of occurrence and persistence of migraine and headache, we performed a univariate and a stepwise multivariate Cox regression analysis. We calculated correlations between subjective weather perception and meteorological data.
Results: In the uni- and multivariate analysis, a ridge of high pressure increased the risk of headache occurrence, lower mean daily wind speed increased the risk of migraine occurrence and a day-to-day change of daily sunshine duration increased the risk of migraine occurrence. A day-to-day change of the daily minimum temperature decreased the risk of migraine persistence. After correction for multiple testing, none of these findings remained statistically significant. Subjective weather perceptions did not correlate with the occurrence or persistence of migraine or headache. Subjective perception of cold and too-cold weather and of too-warm weather correlated with daily minimum, mean and maximum temperature.
Conclusion: The influence of weather factors on migraine and headache is small and questionable.
Introduction
Weather is one of the trigger factors mentioned by patients most frequently (1–3). Sensitivity to meteorological changes is reported by 30–78% of headache patients (1,4). Patients relate headache most commonly to rapidly falling atmospheric pressure (2,5–7). Other weather characteristics suspected to precipitate headache include seasonal changes, bright sunshine, strong winds, hot weather, cold weather or thunderstorms (2,5–8). In contrast to the conviction of many patients that weather contributes to the occurrence of headaches, studies on the relationship between various meteorological variables and headaches or migraine have yielded inconsistent results. Most studies examined the effect of weather variables on migraine frequency and many of them failed to prove a statistically significant relationship (9–12). In some studies, air temperature, atmospheric pressure and wind speed were related to an increase and in others to a decrease in migraine frequency (6,11,13,14). In addition, the influence of certain weather characteristics varied in one and the same study (9,10,12,14–16).
The underlying mechanisms of possible associations between weather and headaches are not understood. It was speculated that sferics (very low frequency atmospherics, i.e. pulse-shaped, alternating electric and magnetic fields of very short duration which originate from atmospheric discharges) play a major causal role (17,18). The influence of atmospheric pressure or Saharan dust on trigeminal structures was examined in two animal models. One study found that the spinal trigeminal nucleus in rats responded to lowering atmospheric pressure and speculated that neuronal activation during atmospheric pressure changes may explain weather-related headaches (19). A recent study showed that Saharan dust containing naturally found microorganisms activates the trigeminovascular system in rats (20). Microorganisms such as bacteria, viruses, fungi and their spores attached to Saharan dust could multiply and initiate a series of reactions upon contact with cloud water and solar energy. This results in an increase in the number of microorganisms, basic amino acids, some metals, bioavailable iron and some unknown particles. The nociceptive effect of African dust is attributed to a nonoparticle (20). In addition, it was speculated that excretion of serotonin or histamine caused by positive ionisation of the ambient air may induce migraine (21). Still, no plausible pathophysiological model exists.
In the present study, we sought to analyse in detail weather-related data from a large prospective diary study including a wide range of factors related to migraine (22). Overall findings of this study, published previously, demonstrated that menstruation increased the risk for occurrence of a migraine attack by up to 96%, whereas other factors (muscle tension in the neck, psychic tension, tiredness, noise and odours increased the risk by no more than 35% (22). In addition, the study showed favourable as well as unfavourable effects of some meteorological factors. In this paper, we present detailed findings on the relation of headache in general and migraine in particular to (i) single weather values, (ii) day-to-day changes in these values, (iii) a synoptic weather classification and (iv) the patients’ subjective perception of weather conditions. Furthermore, we analysed the relation between objective meteorological data and the subjective perception of weather.
Patients and methods
Patients were recruited via newspaper advertisements about trigger factors of migraine. Inclusion criteria comprised written informed consent, age ≥ 18years, a migraine frequency of at least one attack per month during the past six months and a diagnosis of migraine without aura, migraine with aura or probable migraine (with or without co-existing tension-type headache) according to the International Classification of Headache Disorders, second edition (ICHD-II) (23). All patients were seen personally at the clinic and diagnosis was made by one of the authors (CW). Patients with medication overuse headache, other primary or secondary headaches and other clinically relevant diseases (stroke, unstable or acute coronary heart disease, other vascular disorders, marked hypertension, neurological, pulmonary, hepatic, renal or endocrine disease and active malignant diseases) were excluded. The study was approved by the ethics committee of the Medical University of Vienna and Vienna General Hospital.
Patients included underwent a semi-structured interview, filled in paper-and-pencil questionnaires and were required to keep a detailed headache diary. Methodological details have been published elsewhere (22). In summary, biographic data, lifestyle, general medical history and headache characteristics were recorded and patients were provided with a paper-and-pencil diary for 90 days. The diary was filled in every day before bedtime, irrespective of the presence or absence of headache, and covered 59 items potentially related to migraine. All items had to be assessed on a four-point scale or a quantity had to be given. Seven questions referred to the subjective perception of the weather. In addition, the diary covered questions regarding the presence of headache as well as all headache characteristics required for diagnosis according to ICHD-II. Each single headache was classified according to the ICHD-II criteria for migraine without aura (23). Headaches fulfilling none of the criteria B, C and D, (headache duration, headache characteristics and associated symptoms) were excluded from further analysis. Headaches fulfilling one criterion were classified as non-migrainous and those fulfilling two or three criteria as probable migraine and migraine, respectively.
Meteorological data were collected on a daily basis at the Central Institute of Meteorology and Geodynamics, Vienna, Austria, between 1 October 2002 and 31 March 2003. Due to the geographical and meteorological situation, these data are reliable for an area of 25 km around the institute (linear distance). Eleven single values, such as air temperature or atmospheric pressure, were measured every 10 minutes. Based on all these single values, minimum and maximum values, means with standard deviations and sums were calculated for further analysis as appropriate. In addition, we used a synoptic weather classification differentiating 17 different weather situations. This synoptic classification represents macro weather situations in the eastern Alps characterised by typical constellations of pressure gradient between ground level and heights, horizontal and vertical air convection, low pressure areas and air advection. The macro weather situations of the eastern Alps are in fact those weather situations which regulate the local weather in and around Vienna. The weather situations occur irregularly during the year and determine the local weather for shorter or longer periods (24). The classification was done once a day, at 7
Statistical analysis
The statistical analysis was based on the interval between two headache attacks and on the interval between two migraine attacks. The analysis of headache and migraine attacks was based on 20,553 patient days. For analysing the occurrence of headache and migraine, each interval started on the second day after a headache or migraine and ended on the day of the following attack. The first day without headache was excluded from statistical analysis, as on this day the risk of headache and migraine was per definition 0 and covariates could have been influenced by the headache the day before. To evaluate the hazard of occurrence of headache and migraine, we performed univariate Cox regression analyses and a stepwise multivariate Cox regression analysis including those covariables which showed statistically significant results in the univariate procedure. Details of the statistical model have been published previously (22). All continuous covariables were categorised in either two or three approximately equally large classes (leading to either a single or two dichotomous covariables). In total, 116 dichotomous covariables were investigated. For analysis of the persistence of headache and migraine attacks, we performed similar calculations based on the interval between the day after headache or migraine onset and the first headache (migraine) free day, defining persistence as presence of headache or migraine on at least two subsequent days. The hazard ratio for an increase in persistence is <1, because the “hazard” of ending the attack is decreased. Considering that many patients believe that they get headache or migraine immediately before or after a change of weather, we calculated the day-to-day changes in the mean values of the 11 single weather values and included these mean values of change in the multivariate analysis. Correlations between subjective weather perception and single weather values, correlations between subjective weather perception and the mean day-to-day changes of the weather values and correlations between subjective weather perception and the occurrence of migraine or headache were calculated using Spearman’s correlation coefficient. The statistical analysis was based on patient days and on all separately diagnosed headache and migraine attacks, and not on individual patients. For all tests, significance levels were set at p < .05. After performing correction for multiple testing by means of Bonferroni correction, only p values <.0018 were considered significant. All analyses were performed with the statistical software package R. (A language and environment for statistical computing. Development core team organisation. Foundation for statistical computing. Vienna, Austria)
Results
Of 446 patients screened, 397 were included in the original study and 327 completed that study (22). For the present study, we selected those 287 patients living within 25 km of the Central Institute of Meteorology and Geodynamics. Diaries were available from 238 patients (209 women, 29 men) aged 42.2 ± 12.1 years and suffering from migraine for 20.0 ± 12.3 years. Demographic characteristics of the patients are shown in Table 1. The patients kept the diary for 86.4 ± 12.8 days (range 12–104 days). The number of patient days on each day of the study period is shown in Figure 1. Headache was present on 5281 days of 20,553 patient days; of these, migraine (including migraine without aura, migraine with aura and probable migraine according to ICHD-II) was diagnosed on 3404 patient days. Migraine with aura was present on 513 patient days. The mean duration of all headache attacks was 7.1 ± 5.3 hours, and the mean duration of migraine attacks was 8.1 ± 5.5 hours. The intensity of all headache attacks was severe in 30.0%, moderate in 43.4% and mild in 26.6%. Looking at migraine attacks in detail, the intensity was severe in 40.0%, moderate in 47.5% and mild in 12.5%.
Number of patient days on each day of the study period. Patients’ baseline data SD = standard deviation.

Weather characteristics during the study period*
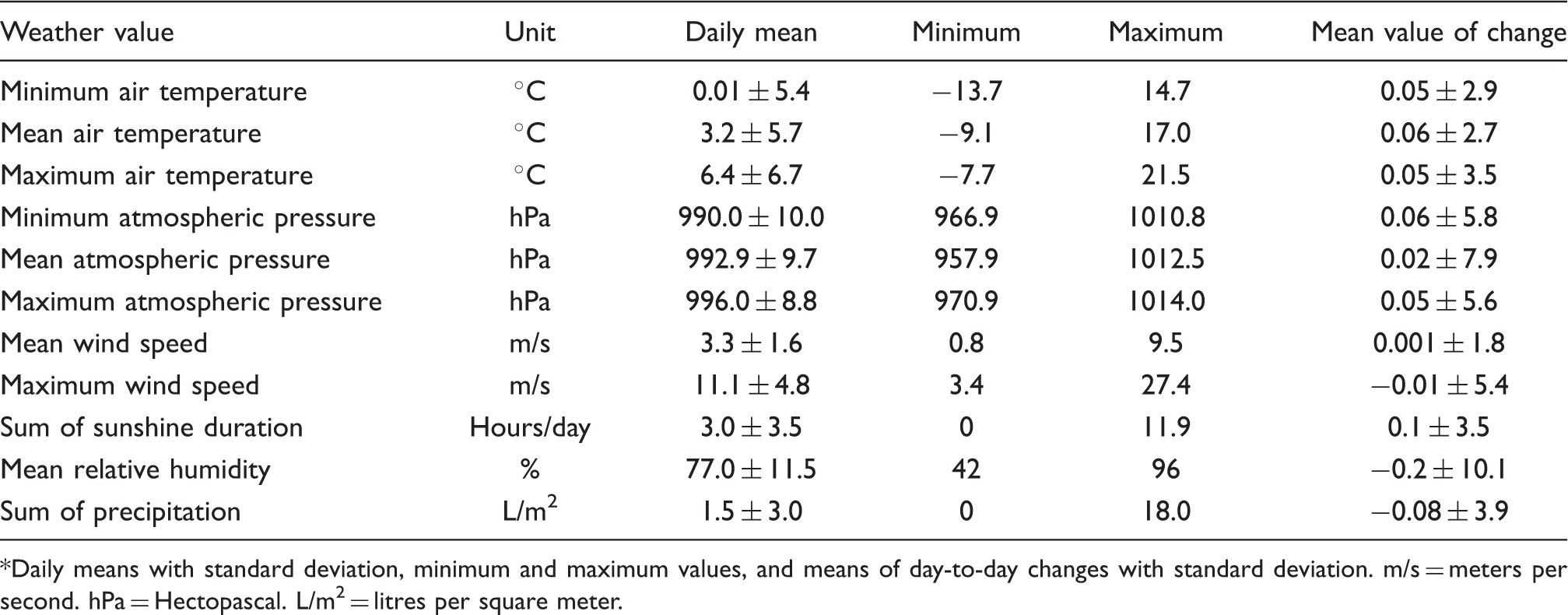
Daily means with standard deviation, minimum and maximum values, and means of day-to-day changes with standard deviation. m/s = meters per second. hPa = Hectopascal. L/m2 = litres per square meter.
Prevalence of various weather situations during the study period, based on all patient days

A day before headache onset is the last headache-free day before the day of headache onset. Low pressure on route Vb = low pressure typically spreading from south Italy to north Italy, Austria and Hungary.
Factors showing a significant influence on the occurrence of headache or migraine in uni- and multivariate Cox regression analysis

stderr = standard error.
p values in bold indicate statistically significant results after Bonferroni correction.
Factors showing a significant influence on the persistence of headache or migraine in uni- and multivariate Cox regression analysis

aThe hazard ratio for an increase in persistence is <1, as the “hazard” of ending the attack is decreased.
p values in bold indicate significant results after Bonferroni correction.
In the uni- and multivariate analyses, only one weather situation had a statistically significant influence on the occurrence of headache: a ridge of high pressure increased the risk of getting headache (Table 4A). Among the single weather values, only a lower daily mean wind speed increased the risk of getting migraine (Table 4A). A day-to-day change of daily sunshine duration slightly increased the risk of getting migraine (Table 4A). There was only a minimal decrease in the risk of migraine persistence due to an increase in day-to-day minimum air temperature (Table 4B). However, after correction for multiple testing, the influence of these weather factors was no longer statistically significant.
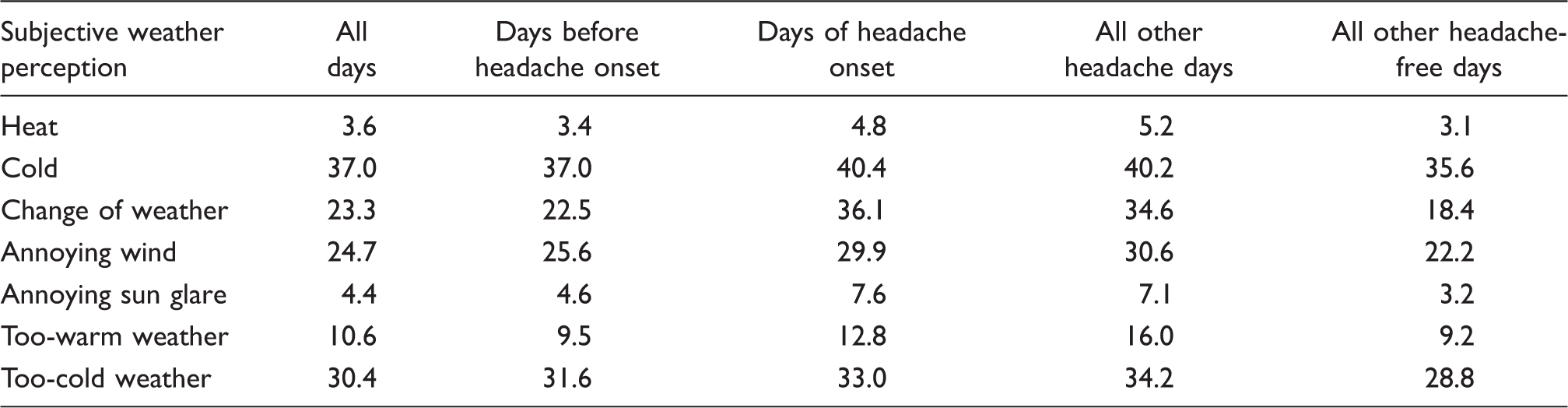
Percentage of patients who have the subjective perception of the presence of certain weather aspects (based on all patient days)
Discussion
In this comprehensive prospective diary study, we analysed 20,553 patient days recorded by 238 patients with migraine. We classified each single headache attack according to ICHD-II (23), and we found very limited influence of meteorological factors on the occurrence and persistence of headache and migraine in migraineurs. We found some influence of a lower daily mean wind speed and the change of sunshine duration on the risk of migraine, occurrence and of the change of daily minimum air temperature on the risk of migraine persistence. Of 17 synoptic weather situations, only a ridge of high pressure increased the risk of headache occurrence. However, after correction for multiple testing, none of these findings remained statistically significant. The patients’ subjective perception of weather did not correlate with the occurrence or persistence of headache or migraine. The relation between the patients’ perception and objective meteorological data was limited to a few correlations. The findings on non-meteorological factors were in agreement with those of the overall analysis published previously (22), although a smaller number of subjects was analysed, because patients who lived in a distance of more than 25 km from the meteorological institute were excluded. In relation to these trigger factors, the influence of meteorological factors is a minor one.
Migraine and weather: methodology of previous studies

HA = headache. M = migraine. TTH = tension-type headache. Ad hoc = Ad hoc committee on classification of headache of the National Institute of Health. ICD-I = International Classification of Diseases, first edition. ICHD-9 = International Classification of Headache Disorders, ninth revision.
Only one hospital visit. bStatistical analysis was done for 53 migraineurs only.
Influence of various single weather values or combined weather factors on migraine frequency: findings of previous studies (figures given are numbers of studies)
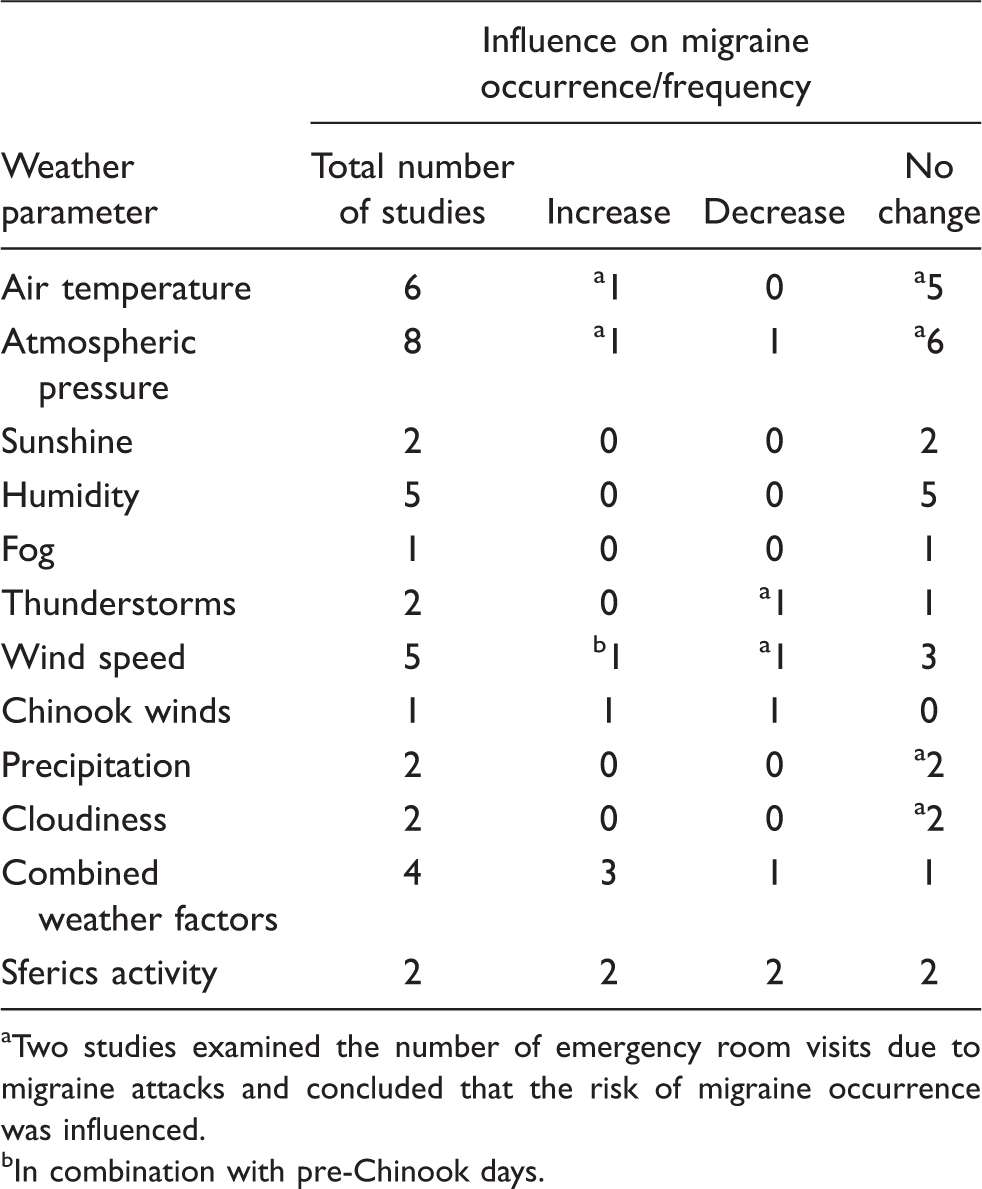
Two studies examined the number of emergency room visits due to migraine attacks and concluded that the risk of migraine occurrence was influenced.
In combination with pre-Chinook days.
The trend towards headache risk being increased by a ridge of high pressure is in accordance with the study of Walach et al. (14), who reported an increased migraine frequency during warm high pressure, exaggerated high pressure and warm air advection at the rim of high pressure. However, in contrast to our study, which was done in autumn and winter, Walach et al. (14) found these correlations during summer months only. Furthermore, in our study, this trend was found for all headache days and not specifically for migraine days. Considering that many patients relate headache and migraine to weather changes (3,4), we included day-to-day changes of single weather values in our analyses, something which was done in only one study previously (15). The previous as well as the present study suggest that these day-to-day changes play a very limited (if any) role.
The considerable discrepancy between subjective weather perception and objective weather values in our study confirms previous studies. Prince et al. (6) reported that about 50% of their patients were sensitive to any weather factor (mostly to a function of absolute temperature and humidity), and 62.3% thought they were sensitive to weather conditions. However, the weather conditions subjectively reported as headache triggers did not correlate with the ones found in the analysis of the objective parameters. Similar discrepancies were reported by Cooke et al. (13). Once more, this underlines that we cannot rely only on patients’ reports of possible triggers and that objective measurements are warranted, collected independently of the patients’ perception (31). We think that the discrepancy between subjective perception and objective weather data could be explained by the patients’ search for causal explanation and selective memory. It may be more likely to recall the co-occurrence of bad weather and headache than bad weather without headache or good weather with or without headache. This hypothesis may be supported by a study on stressful events in patients with tension-type headache. It suggested that patients as well as headache-free persons have a tendency to overestimate stress on retrospective measures (34).
The examination of pathophysiological mechanisms which could link headache and weather was not the goal of the present study. Neither does our study allow any pathophysiological conclusions, nor does it show a consistent factor which could be the goal of experimental or pathophysiological studies on the association of weather and headache.
Regarding the interpretation of previous studies, one has to consider various methodological issues. As shown in Table 6, most studies did not establish diagnoses according to the classification of the International Headache Society but according to ICHD-I or the Ad hoc criteria (32,33). Diaries were used in the majority of studies, but information was usually limited to the absence or presence of headache. Detailed headache characteristics and classification of each single headache attack as suggested by Lipton (33) were used in two studies only (9,13) and in one study partially (12). Observation periods varied from four weeks to six months and covered different seasons. Only two studies (13,15) had longer observation periods and covered all seasons. Correction for multiple testing was explicitly done in only one study (17). The geographical area around the weather station was defined unequivocally in seven studies only. Such definition is necessary, however, since the reliability of weather values is limited to a certain area around the weather station. In addition, special methodological aspects must be considered: two studies examined the association between weather and emergency room visits due to migraine or headache attacks (25,26). Both studies used a case-crossover design which assumes that an event does not occur on a pre-specified control day. Patients were not interviewed about whether they had headache on this control day. Accordingly, the information in both studies is limited to the risk of an emergency room visit because of headache or migraine, and does not allow any conclusions regarding the relation of certain meteorological factors to the presence or absence of headache or migraine. In addition, emergency room visits depend on various factors, such as patient selection, emergency department availability, subjective perception of pain, co-morbid depression or disease severity (35), which might have caused additional bias. Weather is only one co-factor which may influence the decision to visit an emergency department. Accordingly Villeneuve et al. (25) asserted that their study was more an investigation on “visits to a hospital for migraine” and weather than on migraine and weather. In addition, in these studies, the actual onset of headache attacks could not be recorded (25,26).
An important issue in studying the influence of weather on headaches is the dynamic nature of weather. Single weather values can change significantly during one day; synoptic weather classifications are not always stable during one day and can change within hours or over days. Furthermore, each classification means to arbitrarily assign hundreds of weather values and types to only few weather classes. So far, neither our study nor previous studies could manage this challenge sufficiently.
Strengths and limitations
Our study has several strengths and limitations. Strengths are the large number of patients and patient days, the prospective collection of data using a diary which allowed classification of each single headache attack according to ICHD-II (23), the fact that the patients were blinded regarding the collection of objective weather values and the analysis of weather-related variables in the context of other possible trigger factors. In addition, the sophisticated statistical analysis is an important strength of this paper. Analysis of this type of data is not an easy task and is still under statistical scientific discussion (36,37). To our knowledge, for the examination of associations between migraine and weather, such complex models have been used for the first time. The models chosen in this paper have the following advantages. First, they allow analysing recurrent data. Second, they allow accounting for time-varying covariates. Third, they account for censoring due to the 90-day study window and other independent dropout. Fourth, using the robust variance estimate accounts for the correlation of event times of the same subject when estimating the standard errors. The confirmatory analysis with strata based on the number of headache intervals per patient was done to see whether the significant factors found in the main model are mainly driven by few patients with a large number of intervals. Factors that do not rely on few patients with a large number of intervals should be significant also in the stratified model.
Our study is limited, most importantly, by the observation period restricted to the half-year between October and March. In addition, weather classification was done only once a day and the weather class may have changed during the day. Comparing the meteorological findings during the study period with long-term findings, however, did not indicate that weather conditions were unusually stable or unstable during the study. Furthermore, regional geographical variety may have influenced specific weather characteristics, and we did not analyse local weather differences caused by the topographical relief. However, local weather and its local differences are regulated by the macro weather situation and that regulates the local weather within 25 km around the Central Institute of Meteorology and Geodynamics. Accordingly, we selected all patients living within this distance. In addition, one has to consider that many patients work in districts other than the area they live in. Therefore, the procedure chosen was the best possible for studying the influence of weather on headache and migraine guaranteeing an optimum in geographical and meteorological homogeneity. The findings regarding the weather situations are limited to the studied specific area, but the findings on single weather values such as temperature or atmospheric pressure and day-to-day changes of these values probably can be generalised. Finally, the paper-and-pencil headache diary for 90 days involved the possibility that patients reviewed previous answers. However, the patients had to answer 67 questions every day (excluding specific headache questions). Considering this large number of questions, it seems very unlikely that the patients reviewed prior answers when filling in the diary.
Conclusion
The present study as well as previous studies show that the influence of weather on headache and migraine is small if not negligible. This questionable influence can be unfavourable as well as favourable. Our results underline the importance of studying the relation between migraine and weather independently of patients’ subjective perception. They also underline that other factors such as menstruation or lifestyle trigger headache or migraine more frequently, and that these factors should be main targets of therapeutic approach.
Footnotes
Acknowledgements
We thank Drs. Kadriye Aydinkoc, Andrea Böttcher, Evelyne Geuder, Kathi Hanslik, Natalie Hattinger, Julia Holzhammer, Ludmila Zahlbruckner and Robert Zingerle for their help in data acquisition and data processing.
Conflict of interest
CW has received honoraria and travel funding from AstraZeneca, Linde Gas, Menarini and Pfizer. KZ has received honraria and travel funding from Biogen-Idec, Sanofi-Aventis and Serono. CWB has received honoraria from AstraZeneca. All other authors declare that they have no actual or potential competing financial interest.