
Abstract
Objective: The aim of the present study was to characterize perceived consistent triggers of migraine with aura (MA).
Method: Questionnaires specifically designed to characterize various trigger factors were sent to 181 participants identified in an earlier study. All participants had formerly identified at least one factor that often or always triggered an MA attack. They only answered questions regarding this or these factor(s).
Results: The response rate to the questionnaire was 70% (126/179). A number of subtype triggers were mentioned by a high proportion of patients: too much work (under the stress category 54/64), reflected sunlight (under the light category 35/44), too little sleep (under the sleep category 19/24), red wine (under the alcohol category 20/22), passive smoking (under the smoke category 11/11), menstruation (under the menstruation or break from the pill category 12/14) and perfume (under the fumes/heavy scents category 12/15). Hormones, light and stress were reported to cause at least 50 % of MA attacks in 62%, 47% and 42% of participants, respectively. No participants reported alcohol to be the trigger of 50% or more of their attacks. In the groups of participants with “light”, “fumes/heavy scents”, “smoke” or “physical effort” as triggers, nearly all patients reported that an exposure time to the trigger of less than 3 hours (90–100% of patients) was necessary to trigger an attack and a latency to onset of attack of less than 3 hours (90–100% of patients).
Conclusion: Our study has provided new knowledge about factors that in particular patients consistently trigger MA. In daily routine practice this information should be helpful in identifying factors to avoid. Patients with trigger factors that always or usually trigger attacks of MA will be highly useful for imaging and other experimental studies.
Introduction
Genetics play an important role in migraine with aura (MA). First-degree relatives to probands with MA have a four times greater risk of MA compared to the general population (1), and monozygotic twins have a higher probandwise concordance rate than dizygotic twins (2). Spouses to probands with MA do not have an increased risk (1) despite sharing environment with the probands. Environmental factors do, however, play an important role; inheritance in twin studies was only around 50 % (2). Furthermore, individual patients have a great variation in attack frequency during their lifetimes (3), which also points to the importance of an interplay between genetics (risk factors) and environment (trigger factors) as essential. Unfortunately, little has been done to understand the influence of the environment in detail. If trigger factors were better known, it would be possible to change factors in the environment and thus reduce the frequency of migraine. Some environmental factors can probably cause a long-lasting worsening of migraine; however, here we examine only factors that trigger individual attacks. In a previous study we identified a number of trigger factors that often or always trigger an attack of MA in many patients (4). Here, we take one step further by characterizing these factors in detail using a questionnaire developed specifically for this purpose. The aim of the present study was to better understand perceived trigger factors in MA and how patients can avoid them, and also to identify patients who reliably can trigger attacks in experimental studies of migraine mechanisms
Study population
Our study population was identified in earlier studies (5,6). The patients were diagnosed with MA according to the International Classification of Headache Disorders, second edition (ICHD-II) (7). They were recruited from the entire Danish population using two search strategies: extraction of patients from the National Patient Register (NPR) and screening of case records as previously described (5,6).
In brief, patients were extracted from the NPR of all hospitalized patients if they had been admitted to a hospital or seen as outpatients at a department of neurology or paediatrics in any Danish hospital in the years 1994–1997 and discharged with a diagnosis of MA or migraine with complication (ICD 10 diagnosis DG431 or DG433). Additionally, more than 27,000 case records were screened. About 6000 of these came from two headache clinics and a single-photon emission computed tomography (SPECT)-scanning clinic, whereas 21,000 case records were from practising neurologists. A total of 1831 patients were recruited: 1101 from the NPR and 730 from case records. Of 1831 patients, 85 were non-contactable and 381 did not participate. A total of 1365 patients took part in an initial screening interview, and it was found that 128 patients had hemiplegic migraine, 980 had non-hemiplegic MA and 257 did not have any kind of migraine. Among the 980 patients with non-hemiplegic MA and their relatives, 629 were diagnosed with MA according to the ICHD-II using a semi-structured validated extensive telephone interview conducted by a physician or trained medical student. Based on a questionnaire survey regarding trigger factors in this particular group of patients, 181 patients were included in the present study. Inclusion criteria were a minimum of one trigger factor where exposure often or always triggered an attack of MA and at least one attack of MA within the last year; (Figure 1). A regional Danish Ethical Committee approved the project.
Ascertainment of patients reporting a trigger factor that often or always trigger an attack of migraine with aura. MA = migraine with aura. MO = migraine without aura. ICHD-II = International Classification of Headache Disorders, 2nd ed. Category 3 trigger = a trigger that often causes an attack of MA. Category 4 trigger = a trigger that always causes an attack of MA.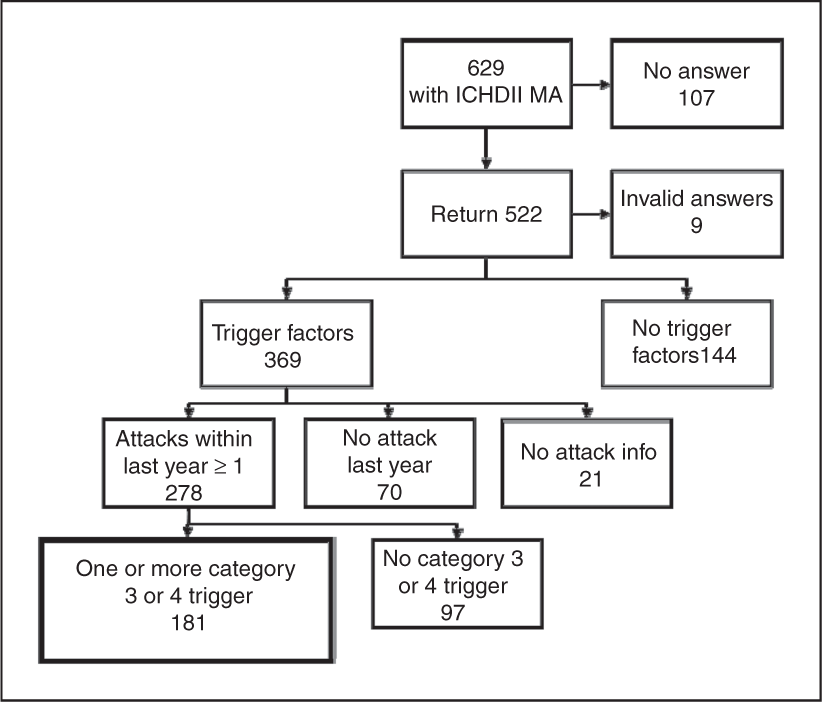
Methods
Part of questionnaire regarding stress as a trigger

One hundred and eighty-one patients were sent a questionnaire. Patients not responding within one month were mailed a reminder letter.
Results
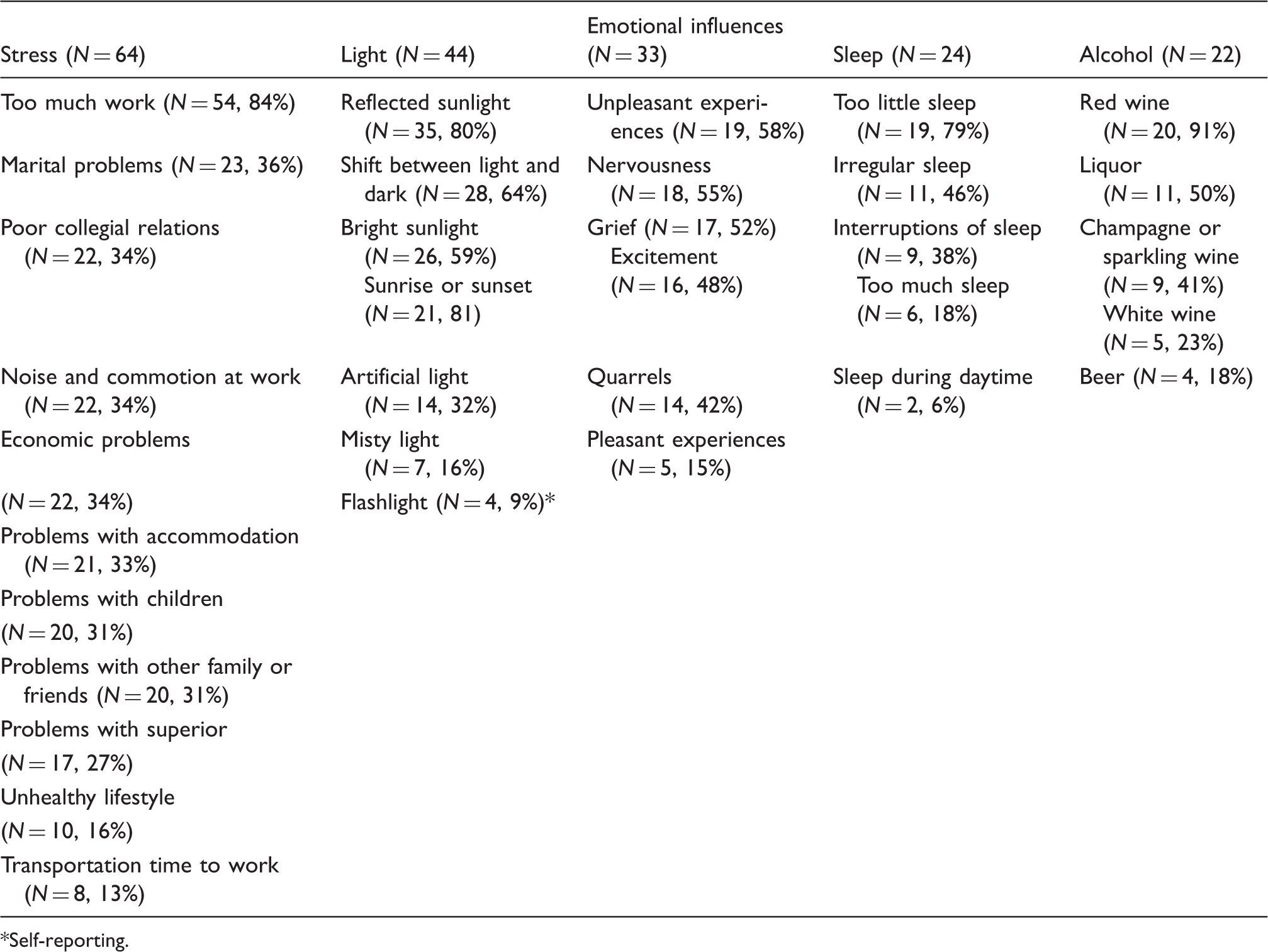
The total response rate was 70% (126/179) (Figure 2). Table 2 shows age and sex distribution as well as the number of attacks of MA and migraine without aura (MO) in participants. The group of non-participants did not differ statistically significant from the group of participants with regard to age, sex, number of attacks of MA and MO (all p ≥ 0.16). Table 3 shows general characteristics of the triggers. Seven subtypes of trigger factors are worth noticing because they were mentioned by a very high proportion of the patients: too much work (“stress” 54/64), reflected sunlight (“light” 35/44), too little sleep (“sleep” 19/24), red wine (“alcohol” 20/22), menstruation (“menstruation or break from the pill” 12/14), perfume (“fumes/heavy scents” 12/15) and passive smoking (“smoke” 11/11). “Food and seasoning” (not included in Table 3) was a trigger for 17 persons. All subtypes of food were self-reported; none were listed in advance. Four kinds of subtypes were reported by more than one person: chocolate (6/17), various seasonings (4/17), sugar (3/17) and cheese (2/17). Reporting of exposure time to specific trigger factors necessary to trigger an attack of MA is shown in Table 4. A brief exposure time (minutes or less) was reported for “light” and “fumes/heavy scents” by at least two quarters of the patients. Table 5 shows latency from exposure to the trigger to onset of the aura. Percentage of attacks of MA considered as being triggered by a specific trigger is shown in Table 6 and modulation of behaviour in order to avoid attacks due to specific triggers appears in Table 7.
Study population. Age, sex distribution and attack frequency (N = 126) MA = migraine with aura. MO = migraine without aura. N indicates the number of valid answers in each category. Number of patients reporting a specific subtype trigger factor Self-reporting. Self reporting. Self reporting Duration of exposure for triggering an attack of migraine with aura NA = not applicable. Time between trigger exposure and attack NA = not applicable. Percentage of patients´ overall attacks caused by the specific trigger factor Modulation of behaviour in order to reduce number of triggered attacks Included are only trigger factors reported by at least 10 patients and behaviour modulation reported by a minimum of one-third of patients.







Discussion
The present study has, for the first time, provided detailed information about perceived consistent trigger factors in MA. Stress, for example, is a well-known trigger factor (4,8–15), but nothing was known about which types of stress are most likely to trigger attack, how severe the stress needs to be, how long the exposure, how long time after the onset of stress attacks occur or what individuals do to avoid stress. The same unknowns pertain to the other frequent trigger factors. Most previous studies concerning triggers have been carried out in a mixed population of headache patients or a mixed population of patients with either MA or MO or both, and only a few of these have paid special attention to the MA subgroup. In a previous study we showed that MA patients report a high number of trigger factors (4), and in the present study we included those patients who had reported at least one trigger factor that often or always triggered an attack.
Based on our results, it is possible to characterize some trigger factors much more specifically by subtype than has been done previously. Stress as a result of too much work was reported to be a trigger by 84% of participants and thus to be significantly more prevalent than the second-most reported subtype of stress trigger (marital problems), which was reported by only 36% of the patients (Table 3). In many previous studies stress has been reported as a prevalent trigger (4,8–15), but to our knowledge it has not been characterized further with regard to subtype. In the category of “emotional influences” only 15% of respondents reported pleasant experiences as triggers, whereas negative feelings and excitement were mentioned as triggers by up to 58%. In a French study, various emotional subtypes were rated (anxiety, irritation, worrying, distress, feeling depressed and strong emotions) (16). Anxiety was the most prevalent of all triggers, but previous the study did not discriminate between MO and MA. Within the category sleep, undersleeping (lack of sleep) was reported significantly more often than other sleep disturbances. Two other studies have also found undersleeping to be a more prevalent trigger than oversleeping (11,17). Fatigue/tiredness were triggers in other studies (12,15,18) but here patients were not specifically asked about the reason for this. In the group of participants with alcohol as a trigger, no less than 91% specified red wine as the trigger. Most previous studies have not looked at subtypes of alcohol (8–10,13,15,16,19) but one study discriminating also found red wine to be the dominating alcoholic trigger (20). Another study, carried out in Japan, found that wine never precipitated MA and only 1.4% of MO patients reported wine as a trigger (17), a difference that could be explained by low alcohol intake and different types of alcohol consumed. In the category “smoke”, all participants reported passive smoking as a trigger (100%), whereas smoke from other sources was reported rarely. Smoke unspecified or smoking inclusive of passive smoking have been reported in other studies (8–10,13,16,17). Within the “smells” category, perfume was reported by a high percentage (80%) of participants. In many previous studies the distinction between perfume and other odours has not been made (8,13,16,21,22), although one other study also found perfume alone as a highly rated trigger factor (11). In the group of women perceiving hormone as a trigger, there was a marked relation to menstruation (no details of contraceptives or hormone replacement therapy were obtained). This result is somewhat in contrast to prospective studies, where only attacks of MO have been related to menstruation (23,24).
Our participants were asked to estimate the percentage of all their attacks caused by each of the trigger factors. In the group of participants with hormones as a trigger, 62% estimated hormones to trigger more than 50% of their attacks. Light and stress were also estimated to cause a high percentage of attacks. Certain forms of light caused more than 50% of attacks in 47% of those sensitive to light. In the group of participants with stress as a trigger, 42% reported stress to be the cause of at least 50% of their attacks. Given the high number of patients with MA reporting light and stress as triggers, it is particularly important to instruct patients to avoid these factors as part of their management. No participants reported alcohol to be the cause of 50% or more of their attacks; maybe because alcohol is an easy factor to avoid. Weather was estimated to cause only 50% of attacks by 8% of participants reporting this factor as a trigger even though this factor cannot be avoided. In two prospective studies where recordings of patients’ headache were related to weather changes, it was shown that patients overestimate weather changes as a trigger factor (25,26).
In order to prevent attacks, 91% of the patients in the group with alcohol as at trigger reported not drinking any alcohol or avoiding certain types of alcohol. This trigger factor may be considered an easy identifiable trigger factor as well as a factor easy to avoid, and patients’ response demonstrates patients’ readiness to change their behaviour in order to prevent attacks. Even though a high percentage of the patients with light or stress as a trigger had also acted to prevent the trigger (e.g. wearing sunglasses, working part-time), these triggers were still estimated by the patients to be the cause of many attacks (Table 6) and other strategies could be useful for these patients. Sleep and smoke are also modifiable triggers. Getting enough sleep is a feasible modification of lifestyle and societal measures are now reducing passive smoking, considerably to the benefit of migraine patients.
We also obtained information about the necessary exposure time of triggers as well as the time lag between exposure and attack in an effort to identify patients who could trigger attacks of MA in association with neuroimaging and other experimental studies of migraine mechanisms. Based on our results we believe that experimental triggering of attacks of MA would be most feasible using light, fumes/heavy scents, smoke or physical effort. For these factors, nearly all patients reported an exposure time to the trigger of less than 3 hours (90–100% of patients) and a latency to onset of attack of less than 3 hours (90–100% of patients). One previous study that produced extremely interesting results experimentally used physical effort as the trigger for MA (27).
The limitation of this study is first and foremost due to recall bias of the participants, and further examination using prospective diaries must be carried out. Our population resembles the general population more than a specialized clinic population, and in future studies it may be considered to pay special attention to patients with a higher attack frequency. In future studies it would also be interesting to look into the aspect of summing of combined trigger factors (e.g. lack of sleep when stressed).
Migraine triggers may act at the cortical level by inducing cortical spreading depression (CSD) (28) or other kinds of cortical activation (29), which then project to the brainstem and disinhibit incoming sensory information; or they may activate multiple brain areas (hypothalamic, limbic and cortical), all of which project to the superior salivatory nucleus, which then causes headache by releasing various peptides that can activate nociceptive meningeal afferents (30). Evidence to support the mechanisms of action of migraine triggers are unfortunately sparse and we will make no further attempt to speculate on the mechanisms here.
In conclusion, our study has provided new detailed knowledge about trigger factors in MA. This should be helpful in the management of patients with MA in daily routine practice. It may also facilitate experimental studies of the migraine aura with imaging and other laboratory tests.