
Abstract
Probable migraine (PM) is a prevalent migraine subtype fulfilling all but one criterion for migraine with or without aura. The aims of this study were: (i) to describe the epidemiology, medical recognition and patterns of treatment for PM in the USA; (ii) to compare the patterns of preventive PM treatment in the population with expert panel guidelines for preventive treatment. A validated self-administered headache questionnaire was mailed to a random sample of 120 000 US households. Subjects were classified as PM according to the second edition of the International Classification of Headache Disorders (ICHD-2). The questionnaire also assessed patterns of migraine treatment. Guidelines for preventive medication use were developed by a panel of headache experts, who used headache frequency and impairment to assess the need for preventive therapy and the gap between current and ideal use. Our sample consisted of 162 576 individuals aged ≥12 years. The 1-year period prevalence of PM was 4.5% (3.9% in men and 5.1% in women). In women and men, prevalence was higher in middle life, between the ages of 30 and 59 years. The prevalence of PM was significantly higher in African-Americans than in Whites (female 7.4% vs. 4.8%; male 4.8% vs. 3.7%) and inversely related to household income. During their headaches, most (48.2%) had at least some impairment, while 22.1% were severely disabled. The vast majority (97%) of PM sufferers used acute treatments, although 71% usually treated with over-the-counter medication. Most PM sufferers (52.8%) never used a migraine-preventive treatment and only 7.9% were currently using preventive medication. According to the expert panel guidelines, prevention should be offered (16.9%) or considered (11.5%) for 28.4% of the PM sufferers in the survey. We conclude that PM is a frequent, undertreated, sometimes disabling disorder. It has an epidemiological profile similar to migraine. In contrast to migraine, which is less prevalent in African-Americans than in Whites, PM is more prevalent in African-Americans than in Whites. In the USA, many with PM do not receive adequate treatment.
Introduction
Many headache sufferers with features of migraine fail to fully meet the International Classification of Headache Disorders (ICHD-2) criteria for migraine with aura or without aura (1–3). Most of these subjects meet criteria for probable migraine (PM), a migraine subtype fulfilling all criteria but one for migraine with or without aura (4). The term PM has replaced the previous term migrainous disorder (5).
PM is a frequent primary headache in the population, with estimates of 1-year prevalence ranging from 2.6% to 9.1% (1–3). A recent study using a validated telephone interview has shown that PM is as prevalent as migraine in participants of a health plan (6).
Like migraine, PM is associated with disability and reduced health-related quality of life (7). Furthermore, PM sufferers benefit from migraine-specific therapy (8). However, a study conducted in the USA has shown that PM is dramatically underdiagnosed and undertreated. Among 1262 PM participants in a health plan, just 2.7% received a prescription for an acute migraine-specific drug (triptans or ergotamine). Migraine preventives were used by a larger number of PM sufferers (13.1%), but also by a high proportion of non-migraine controls (10.5%), suggesting that they were probably used for medical reasons other than migraine. The patterns of medical treatment for PM in the general population are not known (7).
Here, we describe the epidemiology, medical recognition and patterns of treatment for PM in the USA. We also compare the actual patterns of preventive PM treatment in the population with prevention treatment guideline recommendations, in an attempt to identify barriers to optimal care for these subjects. Results are part of the American Migraine Prevalence and Prevention (AMPP) Study, which aims to assess the prevalence, patterns of treatment and unmet treatment needs of migraine and its subtypes.
Methods
Sample and survey
The AMPP was modelled on the methods of the American Migraine Studies 1 and 2, which are described in detail elsewhere (9–11). A validated, self-administered headache questionnaire was mailed in June 2004 to a stratified random sample of 120 000 US households, drawn from a 600 000-household nationwide panel maintained by the TNS/NFO (National Family Opinion). The panel comprises sampling blocks, each with 5000 households, which are constructed to be representative of the US population in terms of census region, population density, age of the head of the household, household income and number of household members.
Initial screening questions were completed by the head of the household, who reported the total number of household members and the number of household members suffering from at least occasional self-defined severe headache. Each household member with severe headaches was then asked to complete the remainder of the survey questions.
The survey consisted of 21 questions assessing headache features. In addition, the survey included the Migraine Disability Assessment (MIDAS) questionnaire (12). Finally, the questionnaire assessed patterns of diagnosis and medical treatment (see below). The survey had been previously validated for the diagnosis of migraine, taking the First Edition of the International Classification of Headache Disorders (ICHD-1) as a gold standard (5), in a population sample of migraineurs and controls with other types of headache. The criteria remained essentially unchanged in the Second Edition of the ICHD (ICHD-2) (4).
Probable migraine case definition
A diagnosis of PM was assigned based on the ICHD-2 criteria. To be classified as PM, the following criteria must have been met:
Respondent reported at least one severe headache in the previous 12 months, but <15 severe headaches per month in the previous 3 months.
Subjects did not meet migraine criteria based on one of the following: (i) they had less than five attacks during their lifetime; (ii) duration of headache was <4 h or >72 h; (iii) headache did not fulfil two of four migraine pain characteristics; or (iv) subjects had no nausea or vomiting, and had no more than one of either photophobia or phonophobia.
The headache did not fulfil criteria for tension-type headache (TTH). In those cases where the headaches met criteria for both PM and TTH, a PM diagnosis was not assigned, in accordance with the ICHD-2.
Patterns of medical treatment
Subjects were asked a series of questions about acute and preventive treatment. The acute treatment options queried were no treatment, treatment with over-the-counter (OTC) medication only, treatment with prescription medications only, or treatment with both OTCs and prescription medications.
Subjects were then asked if they had ever taken prescription medication for a headache on a daily basis, to help prevent headache from happening in the first place. Those who responded positively were asked if they were currently taking such medications. If not, a subsequent question asked when they stopped preventive medication. Finally, subjects were asked about daily medications they were using for reasons other than to treat their headaches. Based on the answers obtained, headache sufferers were divided into four categories of preventive medication use: 1, ‘never users’ had never taken preventive medications; 2, ‘current’ users were taking preventive medications specifically prescribed for their headaches at the time of the survey; 3, ‘lapsed’ users had used preventive medications for headache in the past, but were not using them currently; 4, ‘coincident’ users were using medications that are accepted to be effective preventive migraine medications (β-blockers, tricyclics antidepressants, calcium-channel blockers, antiepileptic drugs) for medical reasons other than headache.
Candidates for preventive therapy
An expert panel comprised of headache specialists, epidemiologists and statisticians with experience in headache research convened several meetings in 2004 and developed recommendations, based on the US Headache Consortium Guidelines, for the use of migraine prevention. Decision rules for the classification of cases based on headache frequency and impairment were reviewed with the objective of identifying operational criteria consistent with consensus guidelines. Impairment during a headache attack was divided into categories of severe impairment (unable to function or requiring bed rest), some impairment (able to function, but with reduced performance) and no impairment (able to function normally). Based on expert consensus, three groups were identified:
Prevention should be offered: sufferers reporting either six or more headache days per month; or four or more headache days with at least some impairment; or three or more headache days with severe impairment or requiring bed rest.
Prevention should be considered: sufferers with four or five migraine days per month with normal functioning; or two or three migraine days with some impairment or two migraine days with severe impairment.
Prevention is not indicated: sufferers with less than four headache days per month and no impairment; subjects with no more than one headache day per month regardless of the impairment.
Data analysis
Sex-specific prevalence estimates of PM (1-year period prevalence) were derived by age, race, urban vs. rural residence, household income and region of the country. GLIM Poisson regression (log-linear models) was used to model sex- and age-specific prevalence by income and to derive adjusted prevalence ratios. Data were modelled separately by gender. Those aged 12–19 years and those ≥80 years were treated as separate categories, and all age groups were modelled as a continuous variable. Two race groups (Blacks, Whites), four population density groups, five income groups and nine US regions were defined.
Analysis of variance (
Adjusted estimates–sex-specific regression models were used to adjust for possible confounding of demographic variables in estimating prevalence. Among males, age (χ2 = 957.95, d.f. = 5, P < 0.0001), income (χ2 = 311.65, d.f. = 4, P < 0.0001), race (χ2 = 19.65, d.f. = 1, P < 0.0001), geographical region (χ2 = 53.01, d.f. = 8, P < 0.0001) and population density (χ2 = 71.85, d.f. = 3, P < 0.0001) significantly improved the fit of the model to the data. Among females, age (χ2 = 4685.75, d.f. = 5, P < 0.0001), income (χ2 = 324.23, d.f. = 4, P < 0.0001), race (χ2 = 57.20, d.f. = 1, P < 0.0001, geographical region (χ2 = 149.70, d.f. = 8, P < 0.0001) and population density (χ2 = 259.51, d.f. = 3, P < 0.0001) each significantly improved the fit of the model to the data. All covariates were included in the final model to derive adjusted prevalence ratios by race, age, income, urban vs. rural residence, and region.
Results
Sample
The instrument was mailed to 120 000 households selected to be representative of the US population with respect to gender, age and census region. Surveys were returned from 77 879 households (65% response) yielding data for 162 576 household members age ≥12 years. A total of 132 674 women were contacted and 85 284 participated in the survey (response rate of 64%); for men, 124 655 were contacted and 77 292 (response rate of 62%) participated. Response rates did not differ by gender, region, regional population density or household income.
The prevalence of probable migraine
There were 7337 individuals age ≥12 years who met ICHD-2 criteria for PM, for a 1-year period prevalence of 4.5%. The prevalence in men was 3.9%; in women it was 5.1% (Table 1). Figure 1 provides prevalence curves adjusted for demographics. In men, the prevalence was highest in those aged 40–49 years and was lowest in those aged ≥60 years (5.1%) and in women, the peak of prevalence happened for age groups 30–39 (6.7%) and 40–49 years (6.5%). The prevalence was lowest in those <18 (2.2% in men and 2.8% in women) and in those >69 years (2.7% and 3.7%).
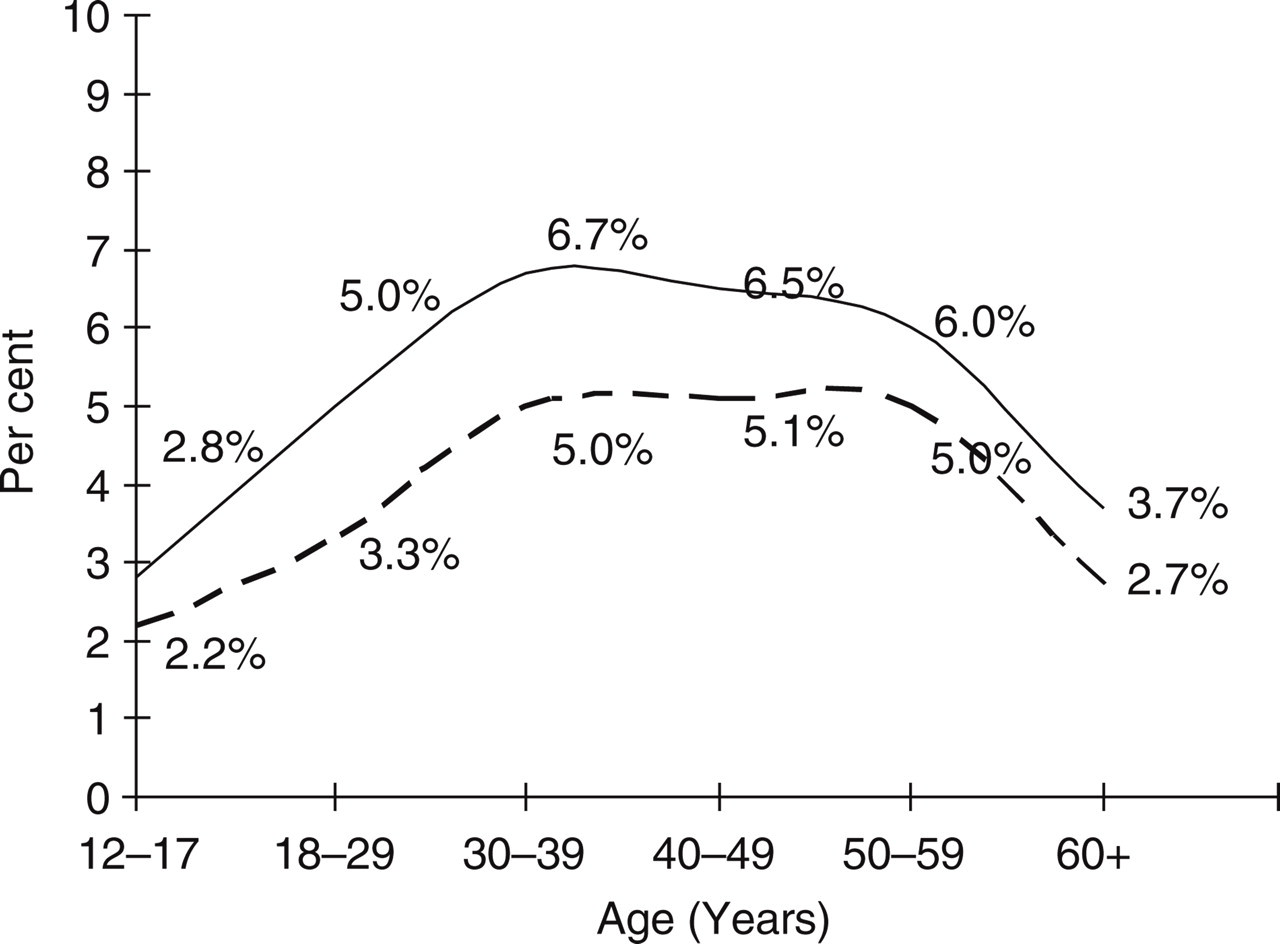
One-year period prevalence of probable migraine by age and gender, adjusted for demographics. – − – –, Males; –––––, females.
Gender-specific 1-year period crude and adjusted prevalence estimates for probable migraine
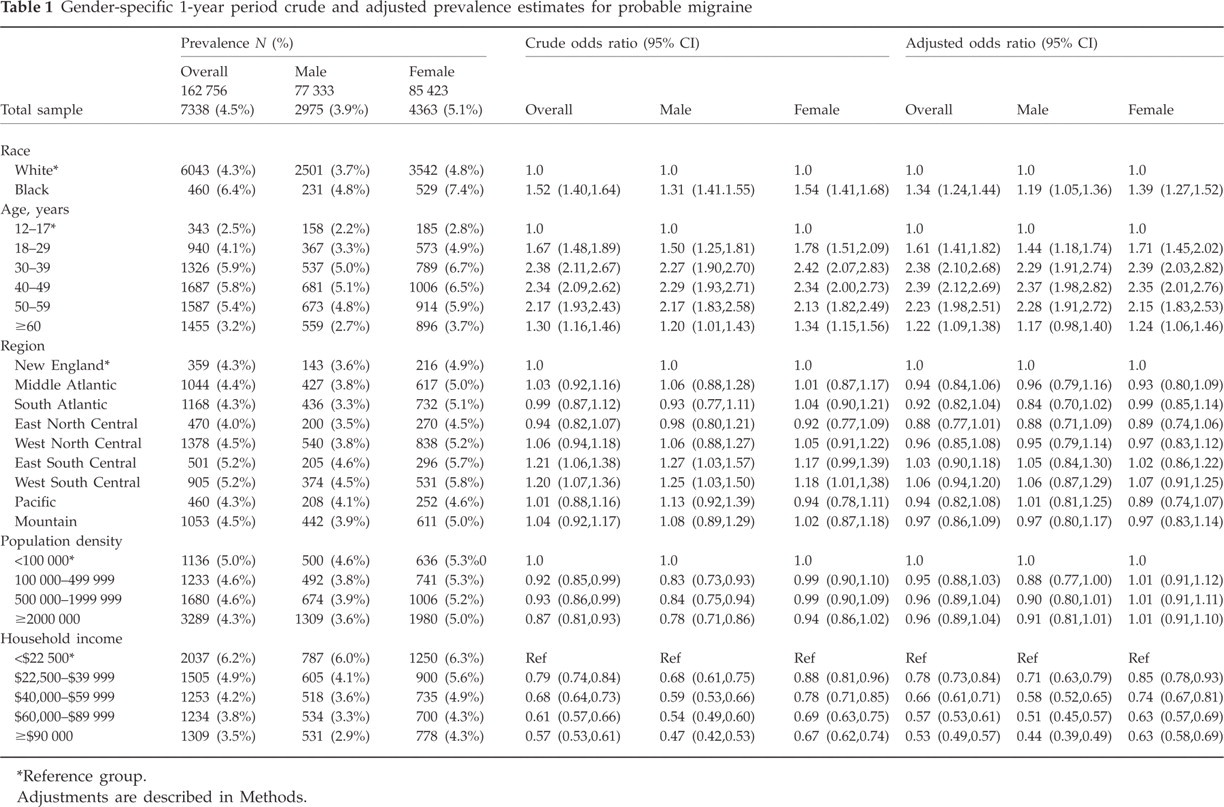
Reference group.
Adjustments are described in Methods.
Table 1 also displays the crude and adjusted prevalence ratios for several demographic features, stratifying by gender. The prevalence of PM was significantly higher in African-Americans than in Whites (female 7.4% vs. 4.8%; male 4.8% vs. 3.7%). There were no significant differences in PM prevalence based on census region or population density. Finally, for both genders, there was an inverse relation between income level and the prevalence of PM. In those with a household income >$90 000, the prevalence of migraine was 4.3% in women and 2.9% in men. In those with an income <$22 500, the prevalence of PM was 6.3% and 6.0%.
Self-awareness of diagnosis
Just 21% of those with an ICHD-2 diagnosis of PM, according to our survey, reported that they ever received a medical diagnosis of migraine. Sinus headache (34.9%), TTH (25.2%) and stress headache (22%) were more common medical diagnoses than PM.
Disability of PM
The majority (58.2%) of the individuals with PM had from 1 to 4 days of severe headache per month (Table 2). During their headaches, most (48.2%) had at least some impairment, while 22.1% were severely disabled. Although over a 3-month period the impact of PM was low for most, 13.1% had missed one or more days of activity due to their PM.
Headache frequency and disability among cases with probable migraine (PM)

Data available from 7299 participants.
Data available from 7202 participants.
Data available from 7040 participants.
Patterns of use of acute treatment
Most PM sufferers in this survey (71.4%) treated their attacks with OTCs only, while 10.8% used prescription medication most of the time (Table 3). A total of 15% sometimes use OTCs and sometimes use prescription medication for their acute treatment. Table 3 displays the patterns of acute medication use stratified by sociodemographic characteristics of the population. Use of a prescription medication was more common in women than in men [odds ratio (OR) 1.46, 95% confidence interval (CI) 1.31, 1.63] and African-Americans than Whites (OR 1.48, 95% CI 1.26, 1.74), and increased with age.
Patterns of acute treatment for probable migraine by sociodemographic characteristics

Odds ratio: none ± over-the-counter (OTC) vs. prescription (Rx) ± both. Adjustments are described in Methods.
Patterns and needs of use of preventive treatment
The majority of the PM sufferers in our survey (52.8%) never used a migraine-preventive treatment and just 7.9% were current users. There were 19.7% reporting coincident use, whereas 19.9% reported preventive medication use in the past. Overall, just 27.6% of PM cases were currently or coincidentally using a preventive medication (Table 4).
Patterns of preventive treatment for probable migraine by sociodemographic characteristics

Odds ratio: ever vs. never. Adjustments are described in Methods.
Subjects using daily medications to prevent migraine.
Subjects using daily medications potentially effective for migraine (see Methods) for other medical reasons.
Compared with those who never used a preventive, and excluding coincident use, ever using prevention (current + lapsed) was more common in women than men (OR 1.24, 95% CI 1.11, 1.39), African-Americans than Whites (OR 2.06, 95% CI 1.74, 2.43), consistently increased with age and decreased with household income (Table 4).
Recommendations for preventive medication were based on headache frequency and attack-related impairment. Table 5 provides the distribution of headache frequency and attack-related impairment experienced by those with PM and correlates it with the headache expert guidelines for prevention use. Based on these recommendations, preventive migraine therapy should be offered (16.9%) or considered (11.5%) in a total of 28.4% of the PM sufferers in the population. Among those who never used preventive migraine therapy, 25.4% were candidates (14.1% met criteria for offering and 11.3% met criteria for considering prevention). No differences in prevention needs were observed between males and females with PM.
The distribution of headache frequency and attack-related impairment, and the corresponding prevention need based on headache expert recommendations
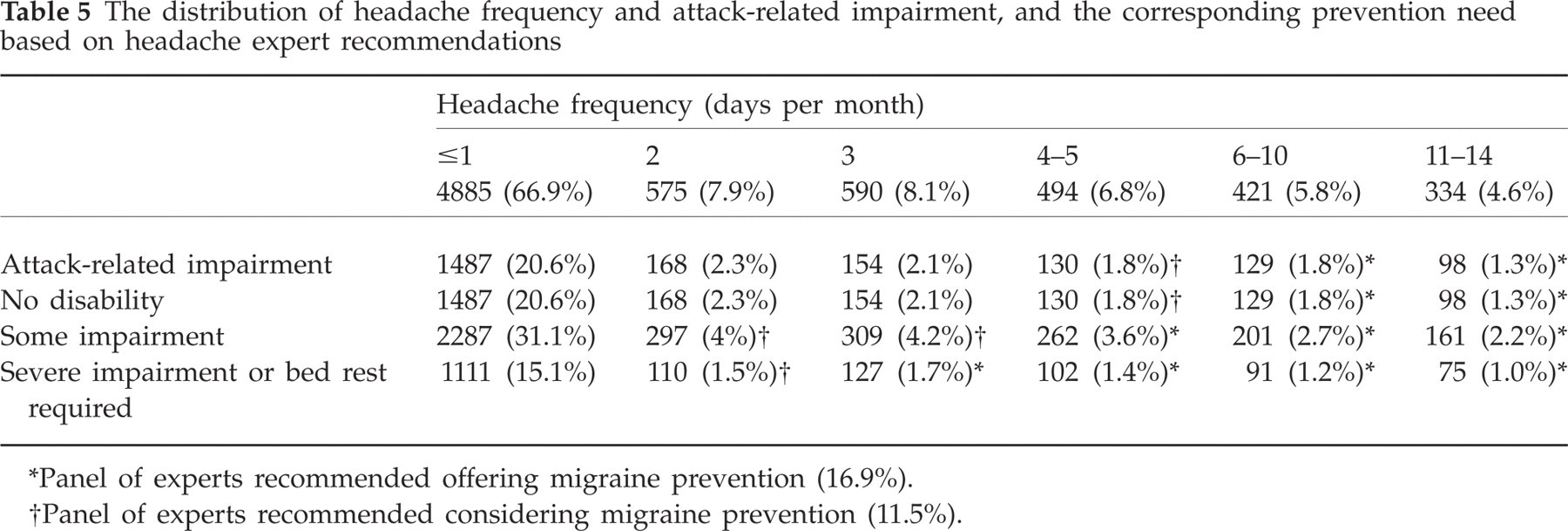
Panel of experts recommended offering migraine prevention (16.9%).
Panel of experts recommended considering migraine prevention (11.5%).
Discussion
As a part of the AMPP Study, we assessed the features of PM in a large representative sample of the US population. Although less prevalent and severe than migraine, PM occurred in about 4.5% of the general population and was disabling to a substantial subgroup of sufferers. Most PM sufferers were unaware of their diagnosis, and a sizeable proportion of those who could benefit did not receive acute migraine-specific treatment or preventive medications.
The prevalence of PM in the general population is still not fully understood (1–3). A population-based study assessing 4000 4-year-old males and females using the ICHD-1 criteria found that the lifetime prevalence of PM was 2.5% with a male:female ratio of 1 : 1.2 (2). Similar prevalence estimates emerged in the AMS II (overall 2.6%, 63% female) (3). In France (13), the prevalence of PM was 9.1%. Finally, a recent study found that, within participants in a health plan that had made at least one medical consultation (for any reason) in the past 24 months, the prevalence of PM was 14.5% (19.6% in women, 13.1% in men) (6).
Our prevalence estimates are broadly consistent with prior reports, particularly the AMS II, which used similar methods (3). However, both the AMPP and AMS II studies identified PM only in individuals with at least one self-defined severe headache in the past year. As PM attacks do not have to be severe, we may have missed individuals with less severe PM and consistently we probably underestimated the prevalence of PM in the USA. That may explain the higher prevalence in the health plan study referenced above (6). That study used a telephone interview instead of a mailed questionnaire and did not screen for severe headache. This may also explain the higher prevalence found in a recent population study conducted in France, where 10 532 subjects were assessed using validated questionnaires that followed the ICHD-2 criteria (Framig 3 study). In the Framig 3 study, more than one type of headache was assessed and the prevalence of PM was 10.1%. In that study, 12.3% of PM sufferers had moderate or severe disability, which is comparable to our own data (13).
Like other reports on PM, we found a higher prevalence in females than in males, a peak of prevalence in middle-life and an inverse relationship with income (1–3, 14). Surprisingly, PM was more common in African-Americans than in Whites. Population studies in occidental countries consistently find that migraine is less common in African-Americans than in Whites (9, 10, 15, 16). Our findings may reflect an important demographic feature of PM. It is possible that African-Americans have less severe headache attacks than Whites, and that attacks therefore would more frequently fulfil criteria for PM than for migraine. The results in African-Americans may reflect race-related differences in symptom reporting, which would be more accurately characterized as reporting bias rather than as a specific feature of PM.
A previous report showed that PM is underdiagnosed and suboptimally treated even in those with access to medical care and prescription drugs (7). In a health-plan study in the USA, among those who had a medical consultation in the previous 24 months, just 1.7% of the PM sufferers diagnosed, based on telephone interviews, received an in-patient or out-patient primary migraine claim. Any headache diagnosis was assigned to just 20.8% of these sufferers. Migraine prescriptions were filled by just 2.7% of the PM sufferers. Non-specific analgesics were filled by 48.8% PM sufferers, as well as by 46.5% of the controls. Preventives were filled by 13.1% of the PM sufferers, but also by controls (10.5%), indicating that they might be used for other medical reasons (7).
The US Headache Consortium provides guidelines for the use of acute and preventive medications (16). These guidelines recommend that migraine sufferers with moderate or severe attacks should be treated with specific acute antimigraine medications. Migraine prevention is recommended in individuals with frequent headaches, as well as attacks that remain disabling despite optimal acute treatment. The goals of prevention are to reduce migraine attack frequency, prevent migraine-related disability and improve health-related quality of life (17, 18). Since PM is a migraine subtype which responds to specific migraine therapy, the same principles for the treatment of migraine may be suggested for PM. We have shown here that just a minority of PM sufferers use prescription medications for their acute treatment, and that a sizeable proportion of them may benefit from preventive treatments.
This study has limitations. First, as mentioned above, the validated questionnaire was applied in just those with a self-defined severe headache, possibly leading to under-ascerainment of probable migraine. Second, selection bias, whereby individuals with a physician diagnosis of migraine may have been more likely than undiagnosed migraineurs to respond to the survey, might have led to an overestimation of the values for some study parameters. Third, the questionnaire was not specifically validated for PM. However, since PM is diagnosed based on the migraine criteria and is a migraine subtype, specific validation was not considered to be necessary. Strengths of this study include the robust sample size (it is the largest migraine epidemiological study conducted to date) and the use of validated symptom screening and other questionnaires that allow comparisons with prior studies.
PM is frequent and under-recognized in the USA. Barriers for optimal care of PM are evident and many disabled individuals with this migraine subtype do not receive adequate treatment. Education initiatives should focus on the medical diagnosis and clinical recognition of PM as a migraine subtype and the benefits of adequate treatment for these individuals.
Acknowledgements
This study was sponsored by the National Headache Foundation through a grant from Ortho-McNeil Neurologics, Inc. The authors thank Kristina M. Fanning PhD and Kathy Ward for help in data management.