
Abstract
The 2004 International Headache Society (IHS) classification of headache disorders introduced the new category of probable migraine defined by the existence of all but one of typical migraine criteria. FRAMIG 3, the first nationwide population-based survey performed in France using the 2004 IHS classification, assessed the prevalence of probable migraine and compared its features and management with those of strict migraine. Of a representative sample of 10 532 adult subjects interviewed, 1179 subjects (11.2%) were diagnosed as having strict migraine and 1066 (10.1%) as having probable migraine. The criterion most frequently missing was typical headache duration (4-72 h) and most subjects with probable headache had shorter average headache duration. Migraine severity and disability, although lower than those noted in subjects with strict migraine, were significant in subjects with probable migraine and quality of life impairment was identical among the two groups of migraine sufferers. Strict and probable migraine, which have similar prevalence and impact on migraine subjects, deserve similar medical and therapeutic management.
Introduction
The International Headache Society (IHS) recently published a second edition of the International Classification of Headache Disorders intended for research and clinical practice (1, 2). This new edition introduces several changes in the classification of headache disorders. As regards migraine, one of the major changes concerns the category termed ‘probable migraine’.
The first edition of the IHS classification (3) acknowledged the occurrence of headache attacks which were believed to be a form of migraine, but did not quite meet the operational diagnostic criteria for any of the forms of migraine. This syndrome, characterized by the presence of all but one of migraine diagnostic criteria (minimum number of attacks over lifetime, typical headache duration, typical headache characteristics, non-pain-associated symptoms) for one or more forms of migraine, was denied the appellation migraine and termed ‘migrainous disorder’. Indeed, it rapidly appeared that many patients likely to suffer migraine attacks fell into this category, although, in the opinion of many clinicians, these patients should be considered genuine migraine sufferers. Shortly after the release of the first edition of the IHS classification, several authors called into question the validity of the classification subcriteria. Rasmussen and Olesen (1991) determined the prevalence of the individual characteristics used as operational diagnostic criteria: studying a group of 112 migraine subjects, they found that unilateral headache was present in only 62% of cases and vomiting in only 50%, whereas other characteristics were present in 80% or more. These authors also noticed that reducing the lower limit of duration of headache attacks from 4 to 2 h would have bisected their group of patients given a migrainous disorder diagnosis (4). Some time later, Michel et al. (5) showed that, although the IHS criteria for migraine had excellent specificity, sensitivity was low (<50%). The diagnostic criteria for migraine seemed too restrictive, leading to a great number of erroneous diagnoses of non-migraine headaches: in fact, half of the IHS diagnostic criteria (typical headache duration, location, nausea or vomiting, aggravation by routine physical activity) were absent in more than 30% of migraine patients diagnosed by senior neurologists (5). Rains et al. found that 36% of migraine patients presenting to an out-patient headache clinic were given a migrainous disorder diagnosis (6). In a recent survey carried out in France, the prevalence of migrainous disorder according to the first edition of the IHS classification was found to be higher (9.1%) than that of migraine (7.9%) (7). It thus appeared clearly that exclusion from the diagnosis of migraine of so many patients presenting with a symptom pattern so close to migraine was questionable. A recently published survey carried out in Sweden deleted the typical headache duration of 4–72 h from the survey migraine criteria (8).
In fact, the second edition of the International Classification of Headache Disorders acknowledges probable migraine (defined as attacks fulfilling all but one of the criteria for migraine) as an integral part of migraine (IHS category 1.6.1). In addition, the new classification also introduces chronic migraine as a new diagnosis for those patients who fulfil the diagnostic criteria for migraine on 15 or more days per month for more than 3 months, differentiating chronic migraine (IHS category 1.5.1) and probable chronic migraine (IHS category 1.6.5) when there is or has been medication overuse within the last 2 months.
FRAMIG 3 is the first nationwide epidemiological survey carried out in France using the diagnostic criteria for migraine defined in the second edition of the IHS classification. It compared migraine impact (disability, quality of life and psychiatric comorbidity) and therapeutic management in different groups of subjects, either defined according to the new IHS classification (subjects with ‘strict’ or probable migraine, subjects with chronic or probable chronic migraine) or distinguished on the basis of patient personal knowledge of the migrainous status (subjects self-aware or unaware of their migraine).
The present article describes the overall methodology of the FRAMIG 3 survey and reports data on migraine prevalence in France according to the recent classification. It concentrates especially on the comparison of particulars of subjects classified as having probable migraine (IHS category 1.6) with those of subjects classified as having strict migraine (categories 1.1 and 1.2.1: migraine without aura and typical aura with migraine headache). In particular, it reports data on the IHS diagnostic criteria for migraine most frequently missing and leading to a shift from a diagnosis of strict migraine to a diagnosis of probable migraine in current practice. Other results will be presented in forthcoming articles.
Methods
FRAMIG 3 is a population-based survey conducted by the public poll institute TNS Sofres. The survey involved two consecutive phases: a screening phase which aimed to identify migraine sufferers among a large sample of subjects representative of the French general population, and a second in-depth analysis phase which aimed to analyse migraine features and management thoroughly in the identified migraine subjects.
The screening phase was carried out from 26 September to 7 November 2003 among the ACCESS SANTE permanent polling base. The ACCESS Panel polling base is updated monthly to maintain its size and representativeness. Individuals entered into the polling base are recruited in several ways (face-to-face interviews, mailings, phone calls) in order to reduce the risk of selection bias possibly associated with a particular methodology. Panellists participate in six to eight health surveys in a year and receive incentive services in return for their participation (no payment). The overall response rate is 70–75% for health surveys.
For the FRAMIG 3 survey, a self-administered questionnaire was mailed to a sample of 15 000 households selected to be representative of the French population. The assessable questionnaires returned by subjects aged ≥ 18 years were entered into the database (initial sample). A target sample size of 10 500 subjects participating was projected.
The questionnaire used in the screening phase for the identification of migraine sufferers involved 56 questions relating to the existence and features of attacks of headache and, for those having headaches, to the opinion whether headaches in reality were migraine attacks (this question explored the self-awareness of the possible migrainous status, i.e. personal knowledge that the headaches were indeed migraine attacks), and to headache-induced disability, health-related quality of life (HRQoL), anxiety and/or depression.
Migraine was diagnosed according to the A to D IHS migraine diagnostic criteria (A: number of attacks over life time ≥ 5; B: typical headache duration of 4–72 h without treatment; C: at least two of four typical headache characteristics; D: at least one of two types of non-pain-associated symptoms) (2). Diagnostic criteria respondents were identified as having strict migraine (categories 1.1 and 1.2.1 for migraine without aura and typical aura with migraine headache, respectively) if their attacks met all IHS diagnostic criteria for migraine, and as having probable migraine (categories 1.6.1 and 1.6.2 for probable migraine without and with aura, respectively) if they satisfied all criteria but one (2). A target sample size of 1800 migraine sufferers was projected.
Migraine impact on subject functioning was assessed by the French version (9) of the Migraine Disability Assessment (MIDAS) questionnaire (10), which focuses on lost days and days with reduced productivity over the last 3 months. The sum of the scores of the five questions of the questionnaire allowed assignment of one of the four MIDAS grades (0–5, grade I; 6–10, grade II; 11–20, grade III; ≥ 21, grade IV).
HRQoL was evaluated using the French version (11) of the Short-Form 12 questionnaire (12). The 12 items of the questionnaire explore eight health concepts: general health perception, limitation of physical activity (physical functioning), limitation of usual activities because of physical problems (role-physical), limitation of usual activities because of emotional problems (role-emotional), bodily pain, psychological distress and well-being (general mental health), energy and fatigue (vitality), and limitation of social activities because of physical or emotional problems (social functioning).
Anxiety and depression were assessed by the French version (13) of the widely used Hospital Anxiety and Depression Scale (HADS) (14). The HADS involves seven anxiety items alternating with seven depression items. Anxiety and depression are defined by anxiety (HAD-Anx) and depression (HAD-Dep) scores > 7, respectively.
The second (in-depth) phase of the survey was carried out from 20 November to 29 December 2003 in the sample of migraine sufferers previously identified who had reported at least one migraine attack during the last 3 months (subjects with ‘active migraine’). These subjects were mailed a second (73-item) questionnaire which explored medical follow-up for migraine, subject appraisal of his/her first medical consultation for migraine, trouble caused by migraine in family, professional, social, and daily life and for close relations (on scales of 0–10), therapeutic management of the last migraine attack (in order to avoid recollection difficulties), and lastly, subject's opinion about current migraine management and satisfaction about the treatment. As regards therapeutic management of migraine attacks, medications used were classified as recommended treatments of migraine attacks [triptans, ergotamine, aspirin, aspirin+ metoclopramide, non-steroidal anti-inflammatory drugs (NSAIDs)] and non-recommended treatments (opioids, paracetamol, fixed combination medications containing simple analgesics combined with opioids, barbiturates and/or caffeine). Efficacy of the treatment used for the last attack was evaluated by the set of four questions designed by the French medico-economic evaluation service (ANAES) and the French Headache Society (SFEMC), which aim to assess migraine relief 2 h after treatment intake, treatment tolerability, the number of drug intakes made to treat the attack, and rapid and normal resumption of social, family, and professional activities (15). A target sample size of 900 responding subjects with active migraine was projected.
Statistical analysis
Representativeness of the initial sample of subjects was assessed by the method of quotas (16) and computerized weighting according to the Raking Adjusted Statistics method (17). Five quotas (gender, two categories; age, five categories; profession, eight categories; regional distribution, nine categories; community size, five categories) were determined on the basis of the statistics published by the French Employment Survey for people aged ≥ 18 years in 2002 (18). Computerized weighting allowed for compensation of any over- or under-representation of some subject strata in the initial sample in terms of the predefined quotas and ensured that the socio-demographic profile of the surveyed subject sample tallied accurately with the profile of the French general population.
Categorical variables were summarized by the corresponding percentages in the relevant subject groups. Between-group differences were evaluated using the Z-test. Numerical variables were summarized by the usual descriptive statistics [mean, standard deviation (SD)]. Where appropriate, between-group differences were compared by Student's t-test (if the size of the groups to be compared was > 30). Statistical significance was considered at P < 0.05.
Results
Of the 15 000 subjects who were mailed the questionnaire for the screening phase of the survey, 10 870 (72.5%) returned it (Fig. 1). Among them, 10 532 (70.2%) subjects aged ≥ 18 years returned a completed and assessable questionnaire (initial sample), 106 (0.7%) returned a void questionnaire, 83 (0.6%) returned a questionnaire with the IHS criteria items incorrectly completed, and 149 (1.0%) were aged < 18 years. Of 1957 migraine subjects with active migraine identified in the screening phase, 1652 subjects participated in the second (in-depth analysis) phase of the survey.
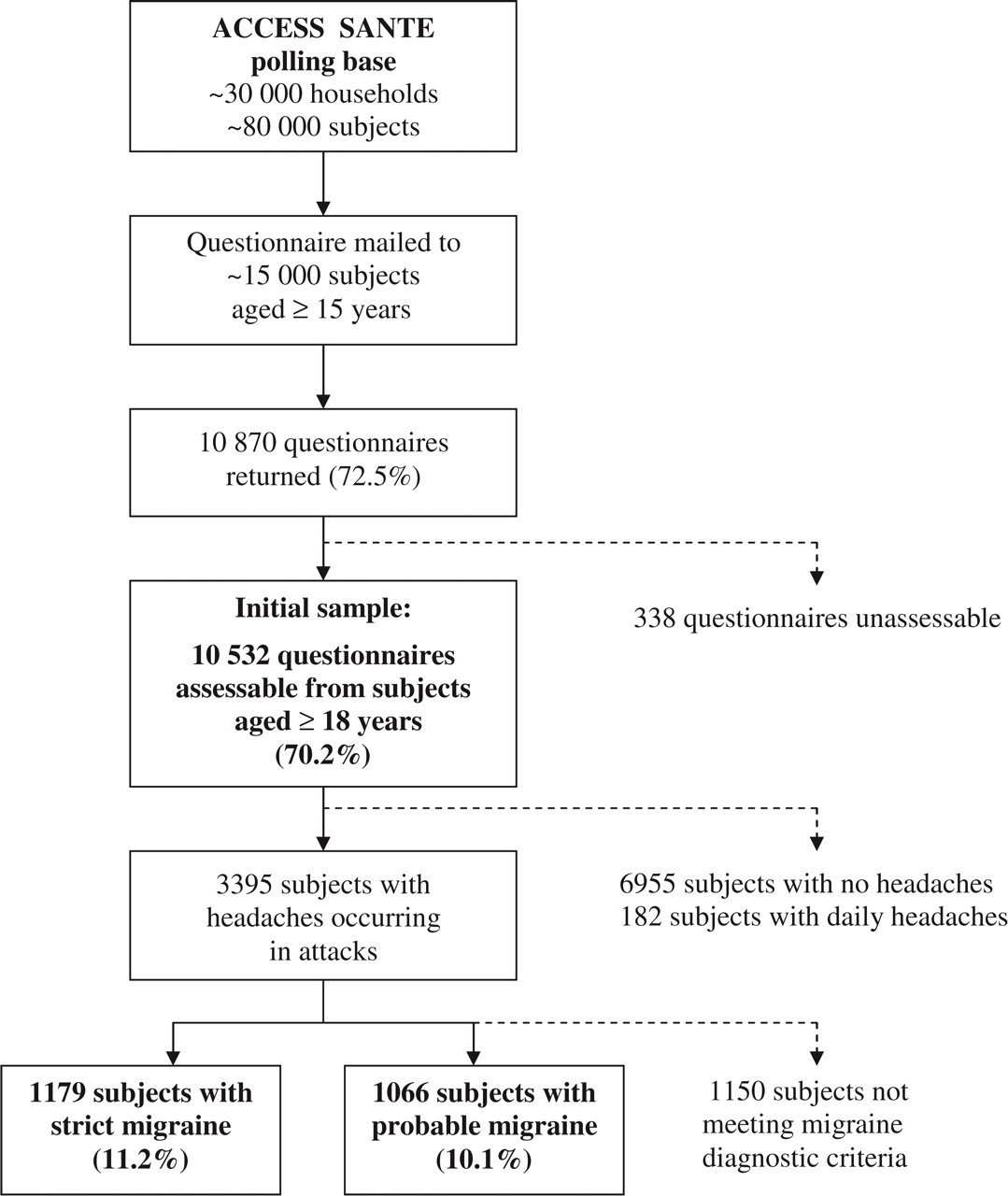
Flow chart depicting the progress of FRAMIG 3 survey (first phase).
In the first phase of the survey, non-responders were more frequently aged 18–34 years or 45–54 years, and farmers, craftsmen/shopkeepers or workers compared with responders. There was no difference in socio-demographic profile between responders and non-responders in the second phase of the survey. Socio-demographic attributes of all subjects in the initial survey sample and of the subset of all subjects identified as migraine sufferers are presented in Table 1. Compared with all subjects in the initial sample, migraine subjects were more frequently female, aged 35–54 years, and middle executives, employees or non-working and less frequently retired or living in the northern part of France.
Compared socio-demographic attributes of all subjects in the initial survey sample and of the subset of all subjects identified as migraine sufferers

,
Statistically different from all subjects aged ≥18 years (P < 0.05 and P < 0.01, respectively).
Mean subject age of the initial subject sample was 47.3 ± 17.4 years.
Prevalence of strict migraine and probable migraine in France
Of the 10 532 subjects in the initial sample, 3395 (32.2%) had had headaches occurring in attacks, of whom 189 (1.8%) had not sustained at least four attacks in their lifetime, 1505 (14.3%) had had attacks lasting < 4 h or > 72 h, 279 (2.6%) had had attacks meeting less than two of the four typical migraine pain criteria, and 243 (2.3%) had had attacks meeting none of the non-pain migraine-associated symptoms. In total, 1179 subjects (11.2%) fulfilled all IHS criteria for migraine, thus meeting the definition of strict migraine (categories 1.1 and 1.2.1 of the 2004 IHS classification), and 1066 (10.1%) fulfilled all IHS criteria except one, thus meeting the definition of probable migraine (categories 1.6.1 and 1.6.2 of the 2004 IHS classification). Thus, total current prevalence of migraine in France is estimated at 21.3%.
In both groups of subjects with strict or probable migraine, migraine prevalence was greater among women and employees, and lower among retired subjects (Table 2).
Prevalence of strict migraine and probable migraine, and overall prevalence of migraine, in terms of socio-demographic categories

,a′,a′′Significantly different from men (P < 0.01).
b′Significantly different from managers, middle executives, workers, retired, and other non-working (all P < 0.01, except for b′ P < 0.05 vs. middle executives).
,c′Significantly different from middle executives and other non-working (all P < 0.01, except for c′ P < 0.05 vs. other non-working); c′′significantly different from employees (P < 0.01).
,d′,d′′Significantly different from all other categories (P < 0.01), except for d′′(P < 0.01 vs. all other categories except farmers).
,e′Significantly different from East, South-West and South-East (all P< 0.01 except for e′ P < 0.05 vs. South-West); esignificantly different from Ile-de-France (P < 0.05).
,f′Significantly different from South-East and Mediterranean, respectively (both P < 0.05).
,g′Significantly different from East and South-East (P< 0.05, except for g P < 0.01 vs. South-East); gsignificantly different from South-West (P< 0.05).
h′Significantly different from East and South-East (both P< 0.05).
Diagnostic profile of subjects with probable migraine
Among the 1066 subjects diagnosed with probable migraine, the prevalence of each individual diagnostic criterion for migraine was 98.1% for criterion A (number of attacks over life time), 38.9% for criterion B (typical headache duration), 85.8% for criterion C (typical headache characteristics), and 77.2% for criterion D (non-pain-associated symptoms). It appears that the migraine criterion most often not satisfied in subjects with probable migraine was criterion B (typical headache duration), which was not verified in nearly two-thirds of subjects diagnosed with probable migraine (651 subjects, 61.1%). Criterion D was not satisfied in 22.8% of subjects, criterion C in 14.2%, and criterion A in only 1.9%.
Thorough analysis of the distribution of subjects with probable migraine as a function of average duration of migraine headaches indicates that, of the 61.1% of subjects with probable migraine not satisfying criterion B, 52.7% (561 subjects) had headaches whose average duration was < 4 h, while only 8.4% (89 subjects) had headaches which usually lasted > 72 h (Fig. 2).

Proportions of subjects with probable migraine (N = 1066) whose average duration of migraine headaches satisfied the International Headache Society criterion B for migraine (typical migraine headache duration), or was shorter (<4 h) or longer (>72 h) than the typical migraine headache duration (4–72 h).
One hundred and thirty subjects (12.2% of subjects with probable migraine) did not fulfil at least two of the four typical headache characteristics of criterion C (unilateral location, pulsating quality, moderate to severe intensity, aggravation by routine physical activity). Pain intensity characteristic was not verified in nearly three-quarters of these subjects (73.1%), while pulsating quality was not verified in 12.3%, unilateral location in 8.5%, and aggravation by routine physical activity in 6.2%.
The migraine criterion most often satisfied was criterion A (number of attacks over life time), which was not verified in only 1.9% of subjects with probable migraine.
Main characteristics of subjects with strict migraine or probable migraine
The main characteristics of subjects with strict migraine or probable migraine are displayed in Table 3. The proportion of women was higher (P< 0.01) among subjects with strict migraine compared with those with probable migraine. Mean age did not differ significantly between the two groups of migraine subjects. In contrast, duration of migraine history was significantly longer in subjects with strict migraine compared with those with probable migraine: significantly more subjects with probable migraine had a migraine history duration of < 1 year or between 1 and 5 years, whereas more subjects with strict migraine had a migraine history duration of > 15 years (Fig. 3).
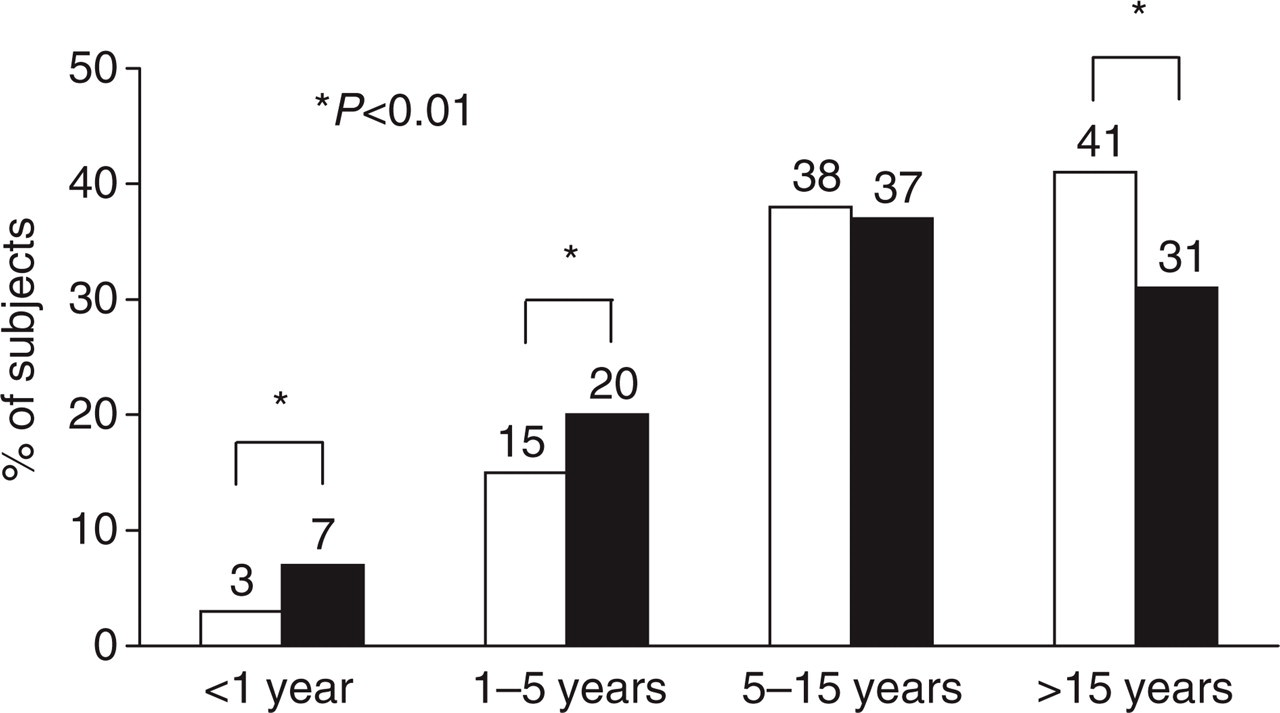
Migraine history duration in subjects with strict (□) or probable migraine (▪) (N = 1179 and N = 1066 subjects, respectively).
Characteristics of subjects with strict migraine and probable migraine, and of the whole group of migraine subjects

Several responses possible.
Significantly different from subjects with probable migraine (P < 0.01).
Two-thirds (67%) of all migraine subjects experienced migraine attacks of moderate intensity and one-third (32%) also reported attacks of severe intensity (Table 3). More subjects with strict migraine had attacks of severe intensity compared with subjects with probable migraine (P< 0.01). Migraine impact on daily living was reported by nearly two-thirds of subjects (60%), and more frequently by subjects with strict migraine compared with their probable migraine counterparts (P< 0.01).
Sixty per cent of all migraine subjects were not self-aware that they had migraine (denied having migraine or did not know). Self-awareness of migraine was more frequent among those with strict migraine than those with probable migraine (P< 0.01), and denial of migraine was more frequent among those with probable migraine than those with strict migraine (P< 0.01) (Table 3).
Migraine-related disability
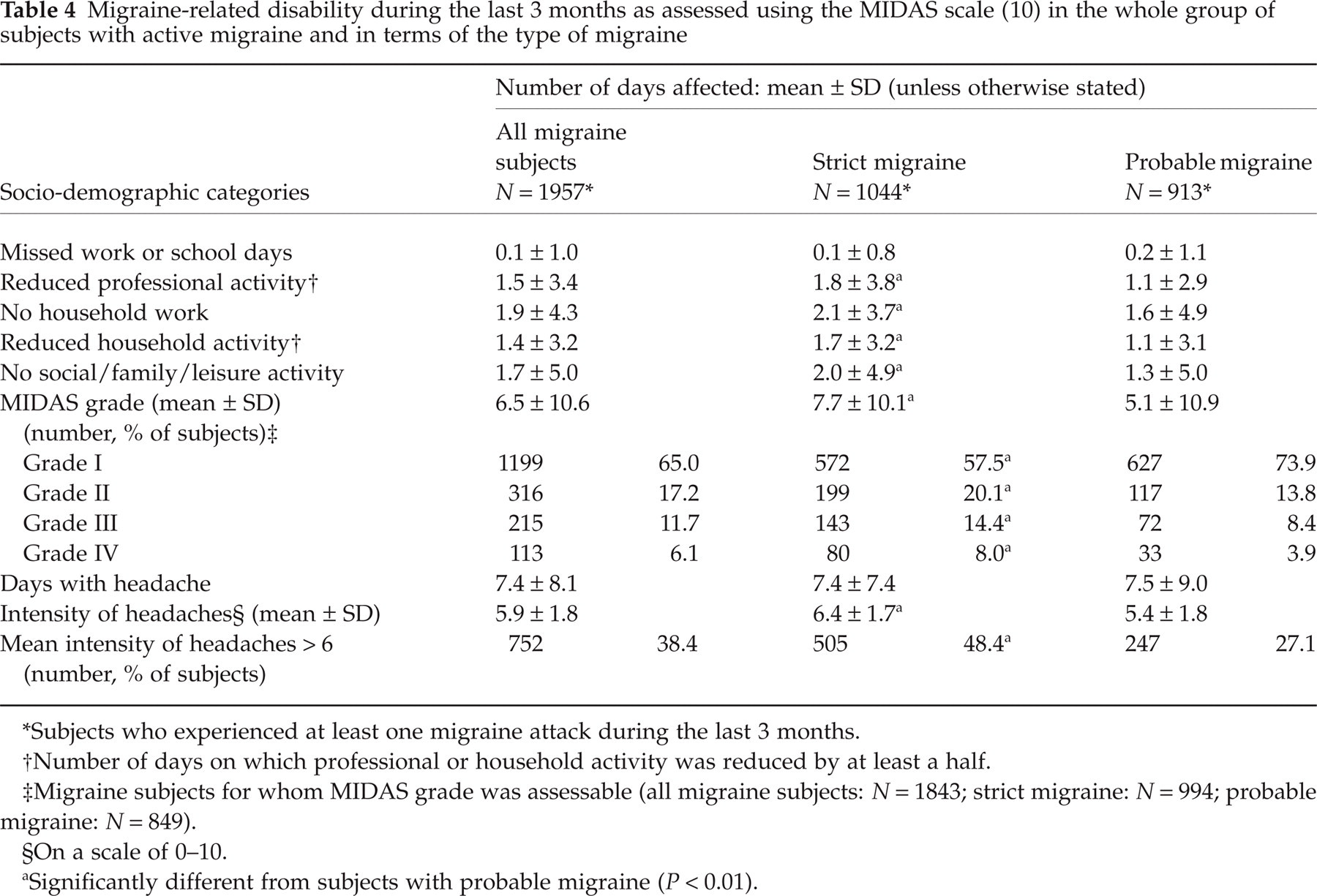
Migraine-related disability was assessed using the MIDAS questionnaire, in subjects who had experienced at least one migraine attack during the last 3 months (subjects with active migraine). Results are displayed in Table 4.
Migraine-related disability during the last 3 months as assessed using the MIDAS scale (10) in the whole group of subjects with active migraine and in terms of the type of migraine
Subjects who experienced at least one migraine attack during the last 3 months.
Number of days on which professional or household activity was reduced by at least a half.
Migraine subjects for whom MIDAS grade was assessable (all migraine subjects: N = 1843; strict migraine: N = 994; probable migraine: N = 849).
On a scale of 0–10.
Significantly different from subjects with probable migraine (P< 0.01).
Of the 1957 subjects with active migraine identified, 1044 (53.3%) were diagnosed with strict migraine and 913 (46.7%) with probable migraine. Over the last 3 months, these subjects had sustained a mean number of 7.4 ± 8.1 days with headache, with no significant difference between subjects with strict migraine and probable migraine. Mean numbers of days affected by migraine (days with reduced professional activity, no or reduced household work, and/or no social/family/leisure activity, because of migraine) were greater (P< 0.01) for subjects with strict migraine than for those with probable migraine, but the number of days on which subjects missed work or school because of the headaches did not differ between the two groups of migraine subjects (Table 4). The mean MIDAS score was 6.5 ± 10.6 for the whole group of migraine subjects with MIDAS grade assessable (1843 subjects), and 17.8% of these subjects were in MIDAS grades III or IV (moderate or severe disability) (22.4% of subjects with strict migraine and 12.3% of those with probable migraine; P < 0.01) (Table 4).
The mean intensity of headaches was 5.9 ± 1.8 on the scale of 0–10, and greater in subjects with strict migraine than in those with probable migraine (P< 0.01). One-third of all migraine subjects (38%) had sustained attacks of intensity > 6 on the scale of 0–10 (48% of subjects with strict migraine and 27% of those with probable migraine, P < 0.01) (Table 4).
Influence of migraine on health-related quality of life (HRQoL)
Of the 8287 non-migraine subjects and 2245 migraine subjects contacted, 7863 (95%) and 2164 (96%), respectively, entirely completed the SF-12 questionnaire, thus allowing the calculation of the eight SF-12 health concept scores.
Mean scores of the eight health concepts were quite similar for the whole group of migraine subjects and subjects with strict or probable migraine. On the other hand, all groups of migraine subjects (subjects with strict or probable migraine, and all migraine subjects) showed significantly lower mean scores than non-migraine subjects at all eight HRQoL concepts (P< 0.01) except physical functioning (Fig. 4).

Influence of migraine on health-related quality of life as assessed by migraine subjects (all migraine subjects: N = 2164; subjects with strict migraine: N = 1136; subjects with probable migraine: N = 1028) and non-migraine subjects (N = 7863) using the SF-12 questionnaire (mean scores on a scale of 0 to 100 at each of the eight concepts of the SF-12 scale, higher scores corresponding to greater quality of life) (12). ×, Non-migraine subjects; ▵, subjects with probable migraine; ▪, subjects with strict migraine; ○, all migraine subjects. ∗P < 0.01 vs. non-migraine subjects for all three groups of migraine subjects.
Assessment of anxiety and depression in migraine subjects
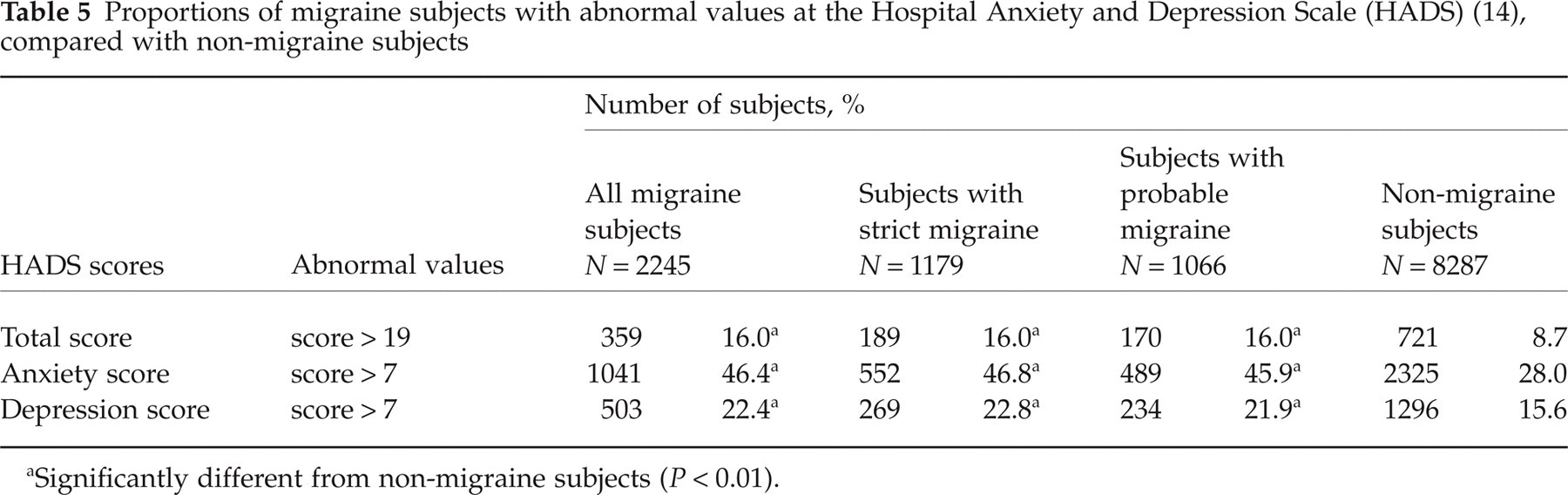
Results of anxiety and depression assessment by the HADS in migraine subjects (all migraine subjects and subjects with strict migraine or probable migraine) and all survey non-migraine subjects are displayed in Table 5.
Proportions of migraine subjects with abnormal values at the Hospital Anxiety and Depression Scale (HADS) (14), compared with non-migraine subjects
Significantly different from non-migraine subjects (P < 0.01).
Compared with non-migraine subjects, significantly more subjects with migraine (strict or probable) had abnormal values (score > 7) at the anxiety subscale (P< 0.01) and the depression subscale (P< 0.01). On the other hand, similar proportions of subjects with abnormal values were found among subjects with strict or probable migraine, both at the anxiety subscale (47% and 46%, respectively) and at the depression subscale (23% and 22%, respectively).
Medical consultation
Of the 1652 subjects with active migraine who participated in the second (in-depth analysis) phase of the survey, 890 (54%) received a diagnosis of strict migraine and 762 (46%) a diagnosis of probable migraine according to the IHS criteria. Of these subjects with active migraine, 59.5% had consulted a physician for the headaches. The corresponding proportions were 65.3% of subjects diagnosed with strict migraine and 52.7% of those diagnosed with probable migraine, the difference between the two subject groups being statistically significant (P< 0.01). Of the subjects who had consulted, only 34.1% (i.e. 20% of the whole group of subjects with active migraine) were still medically followed up (37.0% of subjects with strict migraine, 30.0% of subjects with probable migraine; P < 0.05) and 64.9% had lapsed consulting. On the whole, 79.7% of all subjects with active migraine had no medical follow-up at the time of the survey (75.9% of subjects with strict migraine, 84.1% of subjects with probable migraine; P < 0.01).
Primary reasons for not consulting included the availability of an effective treatment for headaches (71.1% of all migraine subjects; 72.3% of subjects with strict migraine vs. 70.2% of those with probable migraine), and headaches of mild intensity (45.2% of all migraine subjects; 36.7% of subjects with strict migraine vs. 52.4% of those with probable migraine, P < 0.01). Primary reasons for medical consultation included severe and frequent attacks (84.3% of all migraine subjects; 89.2% of subjects with strict migraine vs. 77.2% of those with probable migraine, P < 0.01), impact on daily (professional or family) life (31.2% of all migraine subjects; 35.7% of subjects with strict migraine vs. 24.7% of those with probable migraine, P < 0.01), and advice from close relations (20.7% of all migraine subjects; 19.5% of subjects with strict migraine vs. 22.4% of those with probable migraine). Main reasons for lapsed consulting included the availability of an efficacious treatment (32.5% of all migraine subjects), disappearance of attacks (27.5% of all migraine subjects; 22.0% of subjects with strict migraine vs. 34.8% of those with probable migraine, P < 0.01), and frustration about physicians and/or treatments (37.8% of all migraine subjects).
Severity of attacks and impact on daily living as reasons for consulting were cited more frequently by current consulters (93.0% and 41.4% of subjects, respectively) than by lapsed consulters (80.5% and 26.1%, respectively, both P < 0.01 vs. current consulters).
Therapeutic management of the last attack of migraine
Of the 1652 subjects with active migraine in the second phase of the survey, 1299 (78.6%) had treated the last attack with either a prescription treatment (52.1% of subjects; 55.1% of subjects with strict migraine vs. 48.2% of those with probable migraine, P < 0.05), self-treatment (41.5%; no significant difference between groups), or a medication recommended by the dispensing chemist (5.8%, no significant difference between groups). Slightly more subjects with strict than probable migraine had first used a recommended treatment for migraine attacks (triptan, ergotamine, NSAID, aspirin, aspirin + metoclopramide) (40.8% vs. 35.8%, difference not statistically significant). In particular, triptans had been used by 8.8% of subjects with strict migraine vs. 4.0% of those with probable migraine (P< 0.01). As regards non-recommended treatments, paracetamol had been used by a greater proportion of subjects with probable migraine (42.8% vs. 33.0% of subjects with strict migraine, P < 0.01), whereas opioids had been used by a greater proportion of subjects with strict migraine (16.2% vs. 9.0% of those with probable migraine, P < 0.01). A prophylactic treatment of migraine had been used by a greater proportion of subjects with probable migraine (1.4% vs. 0.3%, P < 0.05).
Most migraine subjects (84.9%) had taken a first acute treatment within 2 h of attack outbreak, and one-third (35.3%) had taken it very soon after symptom onset. However, more subjects with probable migraine than with strict migraine had taken the treatment within the first hour (41.4% vs. 32.1%, P < 0.01), whereas slightly more subjects with strict migraine had waited more than 2 h (15.2% vs. 11.1%, P < 0.05). At the time of treatment intake, the intensity of the last attack was moderate for nearly two-thirds of subjects (61.8%) and severe for nearly one-third (29.7% of all migraine subjects; 32.6% of subjects with strict migraine, 25.9% of those with probable migraine, P < 0.05).
Migraine relief 2 h after intake of the first acute treatment was achieved in more subjects with probable than strict migraine (76.4% vs. 66.2%, P < 0.01), as well as complete resolution of migraine headache (32.2% vs. 20.7%, P < 0.01). A single intake of a single drug unit was made by 41.2% of all migraine subjects (39.0% of those with strict migraine, 44.1% of those with probable migraine), but more subjects with strict migraine had made multiple intakes of several drug units (32.8% vs. 25.5% for subjects with probable migraine, P < 0.01). The treatment taken had been well tolerated by most migraine subjects (96.8%). Rapid resumption of normal daily activities had been achieved by most subjects (77.9% of all migraine subjects; 74.2% of subjects with strict migraine vs. 82.8% of those with probable migraine, P < 0.01).
Additional acute treatments had been taken by a small minority of migraine subjects (12.2% of all migraine subjects; 14.7% of subjects with strict migraine vs. 8.8% of those with probable migraine, P < 0.01). These additional treatments were either recommended treatments (5.5% of subjects) or non-recommended treatments (6.8% of subjects). Overall, total mean number of drug units taken for the acute treatment of the last migraine attack had been 2.9 ± 3.0 for subjects with strict migraine and 2.5 ± 2.4 for those with probable migraine (P< 0.05). The majority of migraine subjects (61.8%) declared that they were entirely satisfied about their treatment (58.5% of those with strict migraine, 66.2% of those with probable migraine, P < 0.01). Reasons for subject dissatisfaction about the acute treatment used concerned principally insufficient (54.6% of subjects dissatisfied) and slow (60.0%) efficacy, with no significant difference between subjects with strict and probable migraine.
Discussion
FRAMIG 3 is the first nationwide survey carried out in France according to the new International Classification of Headache Disorders recently released by the IHS (1, 2). The results presented is this article concentrate specifically on particulars of the new category of migraine acknowledged by the recent classification, namely probable migraine (IHS categories 1.6.1 and 1.6.2), especially the prevalence of probable migraine, and comparison of the clinical profiles of migraine subjects with probable migraine or strict migraine (IHS categories 1.1 and 1.2.1).
Of the initial sample of 10 532 subjects recruited for the survey, 1179 (11.2%) fulfilled all diagnostic criteria for strict migraine, and 1066 (10.1%) fulfilled all criteria but one, thus satisfying the definition of probable migraine. The current overall prevalence of migraine in France is therefore estimated at 21.3% according to the new IHS classification. As expected, the proportion of female subjects was greater among migraine subjects than in the whole group of responders, as was the proportion of subjects aged < 55 years. The relative proportions of subjects with strict and probable migraine are quite similar to those observed in a previous survey recently performed in France (GRIM 2000) for strict migraine (7.9%) and what was named migrainous disorder at that time (9.1%) (although the overall frequency of migraine was somewhat lower in the latter survey since it was carried out on the whole French general population aged ≥ 15 years, and therefore involved subject age groups with lower migraine prevalence) (7). The prevalences of strict and probable migraine found in FRAMIG 3 are also comparable to the respective frequencies noted recently among a group of patients presenting to a primary care clinic in the South of France, namely 11.2% for strict migraine and 14.1% for probable migraine (19).
Analysis of the prevalence of individual migraine diagnostic criteria among subjects diagnosed with probable migraine indicates that the criterion most frequently not verified was typical headache duration. Among the 3395 headache sufferers who participated in the study, the proportion of subjects with average headache duration < 4 h (561 subjects, i.e. 16.5%) is quite similar to the proportion (15.8%) reported in the recently published Swedish survey in a sample of self-considered migraine sufferers (8), whereas the proportion of subjects with headache duration > 72 h is somewhat lower (2.6% vs. 6.4% in the Swedish survey). As regards the group of subjects with probable migraine in the present survey, the typical headache duration criterion was missing in 61% of subjects, while non-pain-associated symptoms (nausea/vomiting, photo- and phonophobia) were absent in 23%, typical headache characteristics in 14%, and minimum number of attacks over life time in 2%. This is in keeping with other observations that failure to meet the typical headache duration criterion was the most common reason for subjects with headaches occurring in attacks to receive what was previously termed a ‘migrainous disorder’ diagnosis: Rains et al. found that this was the case in 58 (70%) of 83 subjects classified as having migrainous disorder (6). However, in this study, most migraine subjects who were denied the diagnosis of strict migraine, because their headaches failed to meet the typical duration criterion, had headaches that lasted > 72 h. By contrast, in the present survey, average headache duration was found shorter than 4 h in nearly half of subjects with probable migraine (53%) and > 72 h in only 8%. This is in good accord with results of other studies which found that most subjects who received a diagnosis of migrainous disorder did so because average headache duration was less than the lower limit of the IHS criteria (4 h) (4, 20). The opposite results obtained by Rains et al. (2001) may be related to the study population, since the headache sufferers were recruited among patients presenting for treatment in a specialty clinic setting (thus being likely to have more severe attacks), while the other studies were performed in the general population or in primary care. Migraine attacks of average duration < 4 h may reasonably be expected to be more frequent in the general population than in the population of subjects attending specialty clinics.
As regards the respective characteristics of subjects diagnosed with strict migraine or probable migraine, the main differences concern the proportion of female subjects, duration of migraine history, severity of attacks, migraine-related disability, and migraine impact on daily living and for close relations, all significantly lower among subjects with probable migraine. As could be expected from these data, fewer subjects with probable migraine are self-aware that they have migraine (27%) compared with subjects with strict migraine (52%).
The differences between the two groups of migraine sufferers are, however, relatively small. Migraine attacks of moderate intensity are reported by two-thirds of subjects in each group, and nearly half of subjects with strict migraine and a quarter of those with probable migraine also report attacks of severe intensity. Activities of daily living are affected by migraine for nearly three-quarters of subjects with strict migraine and also nearly half of those with probable migraine. Twenty-two per cent of subjects with strict migraine are in MIDAS grades III or IV, as well as 12% of those with probable migraine. The number of days with headache over 3 months is similar in the two groups of migraine subjects. The migraine-related deterioration of HRQoL is quite comparable between subjects with strict and probable migraine. Abnormal values of the HADS-Anx and HADS-Dep scores are found in similar proportions of subjects with strict and probable migraine. The therapeutic behaviour of subjects with strict and probable migraine is comparable, although those with probable migraine use somewhat fewer recommended treatments. Thus, although some obvious differences exist between the two categories of migraine, the similarities are also evident and aggregating both categories under the term ‘migraine’ in the new IHS classification seems entirely justified.
Furthermore, it is noteworthy that migraine history duration is significantly shorter for subjects with probable migraine compared with those with strict migraine (11.9 vs. 14.3 years, P < 0.01), while mean subject age does not differ significantly between the two groups. This observation may be paralleled by the fact that the majority (53%) of subjects with probable migraine have attacks which last less than the lower limit of 4 h retained for strict migraine. It has been suggested that migraine associated with brief duration of headaches may reflect a developmental phenomenon and that the headaches of these subjects may increase in length with advancing age (6). It may thus be postulated that probable and strict migraine are two evolutionary stages of the same clinical entity and that, with the passage of time, subjects with probable migraine may develop genuine migraine with the entirety of classical attributes. Further investigations are warranted to confirm this hypothesis.
Average headache duration data collected from interviewed migraine subjects must be taken with caution, however. In fact, only few migraine subjects do not treat their headaches. Amongst others, some may mistakenly take the usual duration of the treated attacks for that of untreated attacks, as suggested by Linde & Dahlöf (8), or erroneously remember the length of remote untreated attacks.
What are the possible consequences of these study data for the management of migraine headaches? If probable and strict migraine are two phenotypic forms of the same entity, and the burdens inflicted on patients is comparable, similar treatments must be proposed for the two medical conditions. The same recommendations as for strict migraine may apply for probable migraine, including medical follow-up, prescription of specific treatments and drug intake as soon as possible after the beginning of an attack (15).