
Abstract
Background
Epidemiological data on probable migraine (PM) in Asia have rarely been reported. This study aimed to assess the prevalence, clinical characteristics, and disability of PM in comparison with strict migraine (SM) in Korea.
Methods
The Korean Headache Survey (KHS) is a nationwide interview survey that investigates the status of headache disorders among adults aged 19–69. We used data from the KHS.
Results
In a representative sample of 1507 individuals, the one-year prevalence of SM was 6.0%, and that of PM was 11.5%. Most PM sufferers missed the criterion of typical headache duration (82.0%). Multivariable regression analyses revealed that PM sufferers had an increased odds ratio (OR) for mild headache intensity (OR = 2.08; 95% confidence interval (CI): 1.11–3.90) and decreased ORs for living in a small city (OR = 0.50; 95% CI: 0.26–0.94), living in a rural area (OR = 0.36; 95% CI: 0.14–0.92) and headache frequency five to nine days per month (OR = 0.29; 95% CI: 0.11–0.78) compared to SM sufferers. Some SM and PM sufferers experienced decreased activity (26.4% in SM vs. 18.0% in PM) and missed activity (12.1% in SM vs. 14.4% in PM) due to headache.
Conclusions
PM is a prevalent headache disorder in Korea. Some sociodemographic and clinical characteristics of PM are different from those of SM.
Introduction
Many headache sufferers with migrainous features fail to meet the second edition of the International Classification of Headache Disorders (ICHD-2) diagnostic criteria of migraine without aura (ICHD-2 code 1.1) or migraine with aura (ICHD-2 code 1.2.1), which we refer to herein as strict migraine (SM) (1,2). Most of these cases satisfy the criteria for probable migraine (PM; ICHD-2 codes 1.6.1 and 1.6.2), which is a migraine subtype fulfilling all but one criterion for SM (3).
PM has been reported to be a common primary headache disorder with a prevalence of 2.6%–11.3% in Western countries (4–10). Like the prevalence of SM, the prevalence of PM shows different patterns according to age, gender, geographical region, ethnicity, and socio-economic status. PM is more prevalent in women than in men, and the prevalence is highest among those aged between 20 and 49 years. The prevalence of PM is lower among those aged above 50 years. A population-based study in the United States (US) reported that PM prevalence was higher in African-Americans than in Caucasians (9). PM prevalence is higher among individuals whose highest educational attainment is graduation from high school or less than those who have graduated from college or more (4,5,9).
Studies that investigated diagnostic profiles of individuals with PM have reported controversial results. A population-based study in France reported that 61.1% of the individuals with PM did not meet the criterion of typical headache duration. The second most commonly unfulfilled criterion was that of typical associated symptoms, which was found in 22.8% of individuals with PM (5). A study in the US showed that in individuals with PM, the most common unfulfilled criterion was that of associated symptoms (7). In Singapore, approximately 72.9% of individuals with PM did not meet the criterion for typical headache duration (11).
Like SM, PM had been associated with disability and reduction in sufferers’ quality of life. In population-based studies, 12.7%–22.4% of the individuals with PM reported moderate-to-severe disability, which was similar to or slightly lower than that in individuals with SM (5,9). Further, individuals with PM benefit from migraine-specific treatment that could reduce their headache-related disability by prompt diagnosis and adequate treatment for PM (12).
Previous studies reported that the prevalence of migraine in Asian countries is lower than that reported in American and European countries (11,13–18). Some of these studies in Asian countries suggest that a significant proportion of individuals had PM (15,17). However, the prevalence of PM in Asian countries has only rarely been reported. A population-based study in Singapore reported that PM prevalence was 6.2% (7.5% in women and 4.7% in men). However, disability and impact on quality of life caused by PM have not yet been reported from Asian countries, including Korea.
The Korean Headache Survey (KHS), a population-based, face-to-face interview survey, provides an opportunity to assess the prevalence, clinical characteristics, and disability of individuals with SM and PM (19). The present study describes the above-mentioned features of PM in comparison with SM in the Korean population by using data from the KHS. Further, we assessed the diagnostic profiles of individuals with PM.
Methods
KHS is a nationwide, cross-sectional, descriptive survey on primary headache disorders, including SM and PM, in the Korean population. Structured interviews were conducted by trained interviewers using a questionnaire to determine the status of headache disorders in adults aged 19–69 years. The survey reported the symptoms and management of and disability related to headaches. Socio-economic, demographic, and geographic data were also evaluated. This study was performed in March 2009 in accordance with the ethical guidelines of the Council for International Organizations of Medical Sciences (20) and principles in the Declaration of Helsinki (21). The KHS was conducted with the technical support of Gallup Korea, a global social research company. Gallup Korea provided support in sampling, collecting data, and protecting personal information of participants.
Sample
On the basis of the population structure, our sample targeted 1500 individuals. This sample was used for determining the prevalence of SM and PM and for analyzing the demographic factors involved in SM and PM. We adopted a two-stage systematic random-sampling method. The estimated sampling error of our study was ±2.5% with a 95% confidence interval (22).
Sociodemographic distribution of all survey participants, of the total Korean population, and of cases identified as strict migraine and probable migraine.

Age- and gender-adjusted prevalence.
Compared gender, age group, size of residential area, and educational level distributions between the sample of the present study and total population of Korea.
Questionnaire
The questionnaire was designed to assess demographic and socioeconomic characteristics (nine questions), headache profiles according to the ICHD-2 (21 questions), and headache management (eight questions). We also included the Headache Impact Test-6 (HIT-6) questionnaire (24) to evaluate the impact of headache on the individual’s quality of life. The questionnaire was validated for SM diagnosis with 75.0% sensitivity and 88.2% specificity by comparing the doctors’ diagnosis and diagnosis in the survey. The detailed information for validation of headache diagnosis was described in the authors’ previous article (19).
Survey
The study objectives and methods were explained to our interviewers, who then interviewed a specific number of participants (aged 19–69 years) on the basis of age, gender, and profession. Before beginning face-to-face interviews, the interviewers were provided with the following information: (1) the aims of the study, (2) the meaning of each question, (3) the importance of checking participants’ responses, and (4) other details regarding how to properly conduct an interview.
Case definition of SM and PM
A diagnosis of SM or PM was based on the assigned A to D criteria for migraine without aura (ICHD-2 code 1.1) in the ICHD-2 (A: five or more attacks in a lifetime; B: attack duration of four to 72 hours; C: any two of the four typical headache characteristics (i.e., unilateral pain, pulsating quality, moderate-to-severe intensity, and aggravation by routine physical activity); D: attacks associated with at least one of the following conditions (nausea or vomiting, or both photophobia and phonophobia)). If a participant reported experiencing all of the aforementioned criteria, he or she was identified as having SM. If a participant’s response met all criteria except one, he or she was identified as having PM. In cases in which the headaches met the criteria for both PM and tension-type headache, a PM diagnosis was not assigned, in accordance with the ICHD-2. SM with aura (ICHD-2 code 1.2.1) and PM with aura (ICHD-2 code 1.6.2) were difficult to document using the questionnaire method (25), and we did not attempt to investigate the presence of aura in the present study. If the presence of aura was not investigated, SM with aura and PM with aura would be included in SM without aura and PM without aura, respectively (ICHD-2).
Analyses
Based on the definitions of SM and PM, one-year prevalence was presented as the number of cases per 100 persons. Age- and gender-specific prevalences were also calculated. The results were analyzed using statistical software for Windows, version R 2.14.0 and R commander 1.7-3 (The R foundation, GNU General Public License). For the continuous variables, the Kolmogorov-Smirnov test was applied to test for normality of the distribution. After normal distribution was confirmed, Student’s t test, chi square test and Mann-Whitney U test were used for comparison where appropriate. Values of p < 0.05 were considered to be statistically significant.
Univariable and multivariable odds ratios for probable migraine and strict migraine as function of sociodemographic variables and clinical characteristics in the population.

Proportion of all strict migraine sufferers after age and gender adjustment.
Proportion of all probable migraine sufferers after age and gender adjustment.
Adjusted for clinical characteristic covariates (headache frequency, headache intensity, unilateral pain, pulsating quality, headache, aggravation by movement, nausea, vomiting, photophobia, phonophobia, and osmophobia).
Adjusted for sociodemographic covariates (age, gender, size of residential area and educational level).
OR: odds ratio; CI: confidence interval.
As with most survey sampling designs, missing data resulting from non-response occurred in several variables. The data reported are based on the available data. Sample sizes of some variables diverge from the sample size of n = 1507 because of non-responses on that particular variable. Imputation techniques were not employed to minimize non-response effects (26).
Results
Sample
Our 76 interviewers approached 4054 individuals and 1699 of them accepted the survey (rejection rate of 58.1%). Ultimately, 191 individuals suspended the interview, leaving 1507 subjects who completed the survey (cooperation rate of 37.2%; Figure 1). The cooperation rates were not significantly different among interviewers. Age, gender, size of residential area, and educational level distributions of our samples did not show significant difference from those in the total population of Korea (Table 1).
Flowchart depicting the participation of subjects in the Korean Headache Survey.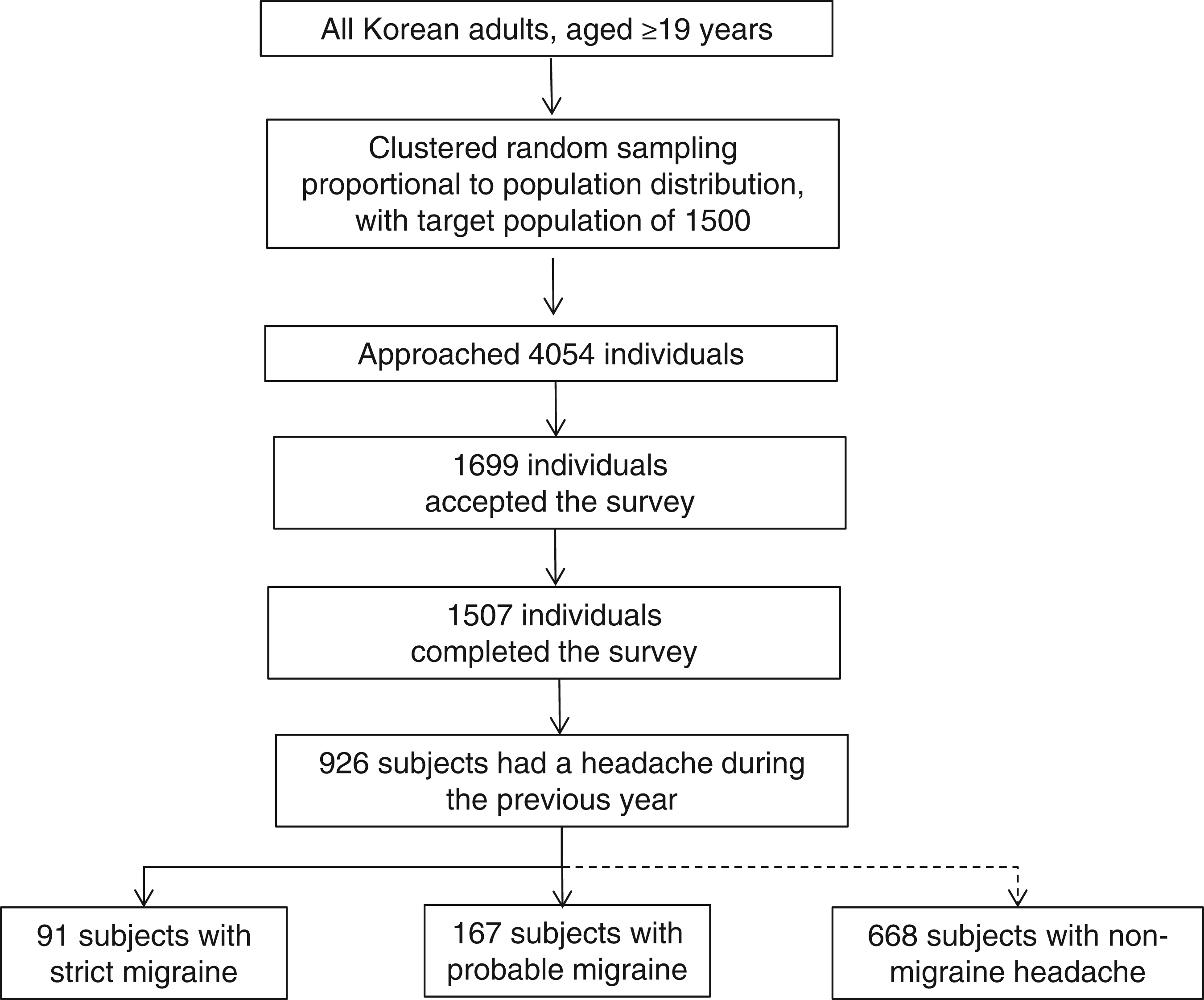
The prevalence of SM and PM
Of the 1507 participants, 926 (61.4%) reported having a headache at least once during the preceding year. Ninety-one participants (6.0%) were classified as having at least one SM attack during the previous year. The women-to-men ratio was 3.2:1 (women, 9.2% and men, 2.9%). After adjusting for age and gender, the highest prevalence of SM was found in the age group of 40–49 years for women and in the age group of 19–29 years in men (Figure 2). The prevalence of SM was inversely associated with the size of the residential area (p < 0.01). Difference in the prevalence of SM based on educational level was not significant (p = 0.57) (Table 1).
The one-year prevalence of strict migraine by age and gender.
One hundred and sixty-seven (11.5%) participants were classified as having experienced at least one PM attack during the previous year. The women-to-men ratio was 2.8:1 (women, 16.8% and men, 6.0%). The highest prevalence of PM was found in the age group of 19–29 years for women. The age group of 60–69 years had the second-highest PM prevalence. The highest prevalence in men was found in the age group of 40–49 years (Figure 3). Differences in the prevalence of PM based on educational level (p = 0.78) and size of residential area (p = 0.76) were not significant (Table 1).
The one-year prevalence of probable migraine by age and gender.
Diagnostic profiles of individuals with PM
Among the 167 individuals diagnosed as having PM, 137 (82.0%) did not meet the criterion of typical headache duration, 28 (16.8%) did not meet the criterion of typical headache characteristics, and two (1.2%) did not meet the criterion of associated symptoms. All individuals with PM met the criterion of the lifetime attack number (Figure 4). All individuals with PM who did not satisfy the typical headache duration criterion had headache durations of < four hours, 57 of them had headache durations of two to four hours, and the remaining 80 individuals had headache durations of < two hours. Of the PM individuals not satisfying the criterion of typical headache characteristics, 28 (100.0%) had pulsating quality, 12 (42.9%) had moderate-to-severe pain intensity, six (21.4%) had aggravation by movement, and three (10.7%) had unilateral pain.
Diagnostic profiles of individuals with probable migraine.
Univariable analyses for sociodemographic variables and clinical characteristics
The sociodemographic and clinical characteristics of individuals with SM and PM are displayed in Table 2. In univariable analyses (see Table 2), using living in a large city as the reference, living in a small city (OR = 0.52; 95% CI: 0.30–0.91) and rural area (OR = 0.33, 95% CI: 0.14–0.74) showed decreased ORs for individuals with PM compared to those with SM. Other sociodemographic variables such as age, gender, and educational level were not significantly different between individuals with PM and individuals with SM. Using those with moderate headache intensity as the reference, mild headache intensity was more common in individuals with PM than individuals with SM (OR = 2.25, 95% CI: 1.25–4.07). Severe headache intensity was not significant. Using those with zero to four headache days per month as the reference, headache frequency of five to nine days per month was less in PM comparing to SM (OR = 0.30, 95% CI: 0.12–0.75). However, headache frequency ≥10 days per month was not significantly different between PM and SM. Unilateral pain, pulsating quality, aggravation by movement, nausea, vomiting, photophobia, phonophobia, and osmophobia were not significantly different between individuals with SM and individuals with PM.
Multivariable analyses for sociodemographic variables and clinical characteristics
As described in Methods, we conducted multivariable-adjusted logistic regression analyses including covariates (Table 2). For sociodemographic variables, PM sufferers displayed decreased ORs for living in a small city (OR = 0.50, 95% CI: 0.26–0.94) and living in a rural area (OR = 0.36, 95% CI: 0.14–0.92) compared to SM sufferers. Other sociodemographic variables such as age, gender, and educational level did not show a significant difference between SM and PM. For clinical characteristics, mild headache intensity (OR = 2.08, 95% CI: 1.11–3.90) showed an increased OR, and headache frequency of five to nine days per month (OR = 0.29, 95% CI: 0.11–0.78) showed a decreased OR for PM from SM. Unilateral pain, pulsating quality, aggravation by movement, nausea, vomiting, photophobia, phonophobia, and osmophobia were not significant.
Disability by SM and PM
Headache frequency and headache-related disability of individuals with strict migraine and individuals with probable migraine.

Compared proportion for reporting activity restriction or missed activity by headache between individuals with strict migraine and individuals with probable migraine.
Compared between individuals with strict migraine and individuals with probable migraine.
HIT-6: Headache Impact Test-6.
Further, we assessed the impact of headache using the HIT-6. The HIT-6 scores of SM and PM sufferers are shown as median and 25%–75% interquartile range values in Table 3. The HIT-6 score of SM sufferers was higher than that of PM sufferers (p = 0.04).
Discussion
Although the prevalence of PM has been reported in several studies, most of these studies were from American and European countries (1,4–10,27). Other than a study from Brazil reporting a remarkably high PM prevalence (18.2%) (6), most studies have reported a one-year prevalence of 4.3%–14.6% for PM (1,4,5,7,9,10). The PM prevalence observed in the present study was broadly similar to those observed in previous studies. Concerning Asian countries, a population-based study had been reported from Singapore. This study reported that the estimated one-year prevalence of PM was 6.2% (11), which was lower than that observed in the present study. The SM prevalence in that Singaporean study (3.1%) was also lower than that reported in studies from other Asian countries including Hong Kong, Japan, Malaysia, and Taiwan (4.7%–9.1%) (11,13,15,16,18). The discrepancy in SM and PM prevalences between the study from Singapore and the present study may be explained by differences in ethnical and cultural background, survey method, and socioeconomic status.
A population-based study in France showed that 67.1% and 21.4% of PM sufferers had moderate and severe headaches, respectively (5). In the present study, 49.1% had moderate intensity while severe headache was reported in 10.2% of PM sufferers (5). Compared to other studies, a study from the US reported lower PM prevalence (4.5%) (9). This study included only those PM individuals who had experienced at least one attack of severe headache. Screening only for severe headache may partially explain the low PM prevalence in the study from the US.
The PM-to-SM prevalence ratios in the previous studies ranged widely between 0.33 and 2.00. In reports from the US and Brazil, where SM prevalences were reported to be higher at 11.7% and 20.4%, the PM-to-SM prevalence ratios were lower at 0.47 and 0.33, respectively (6,9,28). In Singapore, where SM prevalence was reported to be lower at 3.1%, the PM-to-SM ratio was higher at 2.00 (11). These findings may suggest that PM-to-SM prevalence ratio is inversely related with SM prevalence. However, the PM-to-SM ratio in France was an intermediate value as 0.89, where the SM prevalence showed a higher value at 11.2% (5). Another possible explanation for the discrepancy in PM-to-SM prevalence ratios was the differences in case definition, survey method, and ethnic background. The PM-to-SM prevalence ratio in the present study was 1.92, which was similar to that in Singapore.
Previous studies have reported that 61.0% and 72.9% of PM sufferers in France and in Singapore, respectively, did not meet the criterion for typical headache duration (5,11). Our findings are in accordance with these two reports in that missing typical headache duration was the most common cause for PM diagnosis. However, two studies in the US showed that the most commonly unfulfilled criterion resulting in a diagnosis of PM was that of associated symptoms (4,7). Possible explanations for discrepancy in PM diagnostic profile between these two studies and our study are the differences in survey method, cultural background, and biological differences in body mass index. Further studies are needed in order to better understand the diagnostic profile of PM.
In accordance with other studies, the present study showed that PM was more prevalent in women than in men, with a women-to-men ratio of 2.80. The previously reported women-to-men ratios for PM prevalence mostly ranged between 1.16 and 1.56, which was lower than the ratio for SM prevalence (4–7,9,29). The women-to-men ratio in the present study was slightly higher than those reported by the aforementioned studies and was similar to that in a study from Croatia (10). The women-to-men ratio of 1.60 reported by a Singaporean study was lower than that estimated in the present study (11). The high PM prevalence among women in our study might reflect the importance of hormonal influence in the development of PM, as found in SM.
The SM and PM prevalence showed a different pattern according to socioeconomic status in the previous studies (1,4,9). Difference in prevalence according to socioeconomic variables may be explained in part by differences in environmental influences (30). Notably, the prevalence according to sociodemographic variables showed different patterns between SM and PM. In univariable analyses, individuals with PM displayed decreased ORs for living in a small city and a rural area compared to individuals with SM. The decreased ORs for living in a small city and a rural area with PM persisted in multivariable-adjusted analyses. The association pattern according to educational level did not show a significant difference between SM and PM. The discrepancy in the association between the prevalence and sociodemographic factors suggests different environmental influences between SM and PM.
Some clinical characteristics of PM were different from those of SM. In univariable analyses, individuals with PM showed an increased OR for mild headache intensity and decreased ORs for headache frequency of five to nine days per month compared to those with SM. The association with mild headache intensity and headache frequency five to nine days per month remained significant in multivariable analyses. Differences in clinical characteristics between SM and PM in multivariable analyses have not yet been reported. Further work is needed to fully explain the difference in clinical characteristics between SM and PM.
In the present study, we assessed the disability and impact of SM and PM. Disability of PM was comparable to that of SM. The number of decreased-activity days and missed activity days was similar between SM and PM. The impact of headache on PM sufferers, assessed by the HIT-6, was lower than that on SM sufferers. However, approximately one-fifth of PM sufferers reported a substantial or severe impact of their headaches on their quality of life.
Data regarding SM prevalence are available for six countries in Asia: Hong Kong, Malaysia, Japan, Korea, Singapore, and Taiwan (11,13–18,31). Barring the first report in Korea (31) and the report in Singapore (11), the one-year prevalence of SM was fairly consistent and ranged from 4.7% to 9.1%, which is lower than that observed in the European (10%–25%) and North American countries (9%–16%). The SM prevalence estimated in the present study was comparable to that reported in previous studies from Asian countries (13–17).
The first nationwide population-based study on migraine was conducted in Korea in 1995 (31). The one-year prevalence of migraine reported in that study was 22.3%; this is much higher than the prevalence observed in the present study. This discrepancy in prevalence values between the first and present study could be due to several factors. First, the first study included both SM and PM under the diagnosis of migraine (ICHD-1 codes 1.1, 1.2, and 1.7). If the SM and PM prevalences estimated in the present study are combined, the prevalence of migraine is 17.5%, which is comparable to that reported in the first study. Second, low response rates for both mailing and telephone surveys can introduce interest bias and lead to artificially high estimates of migraine prevalences. Third, socio-cultural status changes may affect migraine prevalence where industrialization and development have been greatly promoted since the first study.
This study had some limitations. First, although the questionnaire in the present study was validated for SM, it was not specifically validated for PM. The diagnosis of PM was based on SM diagnosis according to the ICHD-2, and PM is a subtype of migraine. We used a questionnaire based on the ICHD-2 for SM and PM diagnosis since specific validation of PM was not considered necessary. Second, although the present study is a population-based study with low sampling error, its statistical power was limited for examining subgroups. Thus, some conditions that did not reach statistical significance could merely be a reflection of the limited sample number. A significant strength of our study was the use of clustered random sampling proportional to the Korean population. Combined with low sampling error in this study, this approach allowed us to successfully assess and compare the prevalence, clinical characteristics, and disability of PM and SM.
The one-year prevalences of SM and PM in Korea were 6.0% and 11.5%, respectively. Upon combination of the SM and PM prevalences, all migraine had a prevalence of 17.2%. The prevalence of PM was highest among women aged 19–29 years and in men aged 40–49 years. Missing the criterion of typical duration was the most common reason for PM diagnosis; this criterion was missing in 82.0% of PM sufferers. The next most common reason for PM diagnosis was missing typical headache characteristics, which was the case for 16.8% of PM sufferers. Compared to individuals with SM, those with PM more frequently showed mild headache intensity and, less frequently, headache frequency five to nine days per month. Disabilities of PM, such as missed activity days and decreased activity days, were similar to those seen in SM.
Clinical implications
Many headache sufferers with migrainous features fail to meet the second edition of International Classification of Headache Disorders (ICHD-2) diagnostic criteria of migraine without aura or migraine with aura (strict migraine, SM). If an individual’s headache meets all but one criterion for SM, he or she was diagnosed as having probable migraine (PM). Epidemiological data regarding PM in Asia have rarely been reported. This study aimed to assess the prevalence, clinical characteristics, and disability of PM in comparison with SM in Korea.
Footnotes
Acknowledgments
The authors would like to thank Gallup Korea for providing technical support for the Korean Headache Survey.
Funding
Korean Headache Survey is funded through a research grant to the Korean Headache Society from Boryung Pharmaceutical Inc.
Conflict of interest
The authors declare that they have no conflicting interest.