
Abstract
The objectives of this study were to assess the proportion of subjects with strict migraine (SM, migraine with and without aura), probable migraine (PM), and all migraine (AM, SM and PM pooled together), who receive a medical diagnosis or a specific treatment within a health plan. Eligible participants were 18-55-year participants of a non-profit health maintenance organization (HMO) who had received out-patient, emergency department, or in-patient care from a physician within the past year. We used a validated computer-assisted telephone interview (CATI) survey to identify SM, PM and controls (received out-patient, emergency department, or in-patient care from a physician for any reason within the past year, but did not have SM or PM). Medical and prescription drug claims for the 24-month period were linked to participant files. Among 8579 respondents, we identified 1265 SM sufferers and 1252 PM sufferers, which were compared with 960 randomly selected controls. Just 194 (15.3%) SM, 21 (1.7%) PM, and 215 (8.5%) AM sufferers received an in-patient or out-patient primary migraine claim in the previous 24 months, compared with six (0.5%) controls; 240 (18.9%) SM, 39 (3.1%) PM, 279 (11.1%) AM sufferers, and eight controls (0.6%) received any migraine claim. There were claims for migraine drugs (ICD-9 code for triptans or ergot compounds) for just 140 (11.1%) SM and 34 (2.7%) PM sufferers, and migraine analgesics (butalbital and isomethepthene compounds), for 6.3% SM and 2.2% PM sufferers (0.7% of the controls). Migraine preventives were used for a larger number of SM and PM sufferers (19.6% and 13.1%), but also for controls (10.5%), indicating that they were probably used for other medical reasons. Both SM and PM are underdiagnosed and undertreated within a health plan. Educational strategies should focus on physician education addressing diagnosing the full spectrum of migraine and physician management of migraine with specific migraine therapy in appropriate patients.
Introduction
Clinic and some population-based studies (1–3) show that a sizeable group of patients with many features of migraine fail to meet fully the International Classification of Headache Disorders (ICHD) criteria for migraine with aura (ICHD 1.2), or migraine without aura (ICHD 1.1) (4). Herein we refer to subjects who fully meet those criteria as strict migraine (SM). Many of these patients meet criteria for probable migraine (PM, ICHD 1.6), a group defined in the ICHD by headaches that fulfil all criteria but one for migraine with or without aura (4). The term PM replaced the term migrainous disorder (5). Population estimates for the prevalence of PM range from 2.6% to 9.1%(1–3).
The ICHD criteria classify PM as a subtype of migraine (4, 5). Using a validated telephone interview we recently showed that PM and SM are equally prevalent within a health plan (6). Like SM, PM produces substantial disability and reduced health-related quality of life (6). PM sufferers also benefit from migraine-specific therapy (7). Given the pain, disability and treatment response of PM, population studies that focus on SM miss an important part of the migraine problem. Though diagnosis and treatment patterns for SM have been carefully studied, these patterns are less well characterized for PM.
SM is a prevalent, disabling, underdiagnosed and suboptimally treated disorder (8–11). Although severely affected SM sufferers tend to receive more medical care than those who are less affected (12), about half of all migraineurs deny having ever received a migraine diagnosis from a physician (9, 10, 13). Most SM sufferers are treated with over-the-counter (OTC) medications to the exclusion of prescription drugs (9, 10). About two-thirds of migraineurs have sought relief within the healthcare system but one in five has lapsed from medical care (14–17).
Herein, we assess the patterns of diagnosis and treatment for PM within a health plan. We also assess patterns for subjects with SM and all migraine (AM), pooling together SM and PM. To achieve this objective, we linked the headache diagnoses and medication use obtained through a validated telephone interview with medical and pharmacy claims derived from a health plan.
Methods
Data collection and telephone interview
This study was approved by the Institutional Review Board. Participants were enrolees, aged from 18 to 55 years, of a large non-profit health maintenance organization (HMO) in south-eastern Michigan, who had been participating in the plan for a continuous 24 months prior to the study. To ensure active enrolment, eligible subjects had to have received out-patient, emergency department, or in-patient encounter with a health-plan physician for any reason (not necessarily headache) during the 24 months preceding the interview.
Potentially eligible members were mailed an introduction letter by the HMO organization, including a toll-free number for those who did not wish to be contacted. A total of 633 potentially eligible subjects declined to participate in the study. A call list was developed of the remaining 22 666 members and no less than 10 attempts were made to contact each individual at various times during the week, including weekends. From the 22 666 eligible participants, 14 087 could not be contacted for interview, and 8579 completed the computer-assisted telephone interview (CATI), for a participation rate of 37.8%.
The CATI has been extensively used and validated in independent studies in the UK and the USA (18), and has been shown to have high sensitivity (UK 91%, USA 85%) and specificity (UK 97%, USA 96%) for diagnosing migraine. In the CATI interview, we first asked how many different types of headache the subject experienced. For those who had more than one type, the two headache types that were considered most important by the subject were assessed.
Case definitions
Survey respondents were assigned to one of three groups based on their response to the CATI. The groups included: SM [had a CATI diagnosis of International Headache Society (IHS) 1.1 and 1.2, and had a medical visit for any reason, not necessarily headache, in the past year], PM (had a CATI diagnosis of IHS 1.6, and a medical visit for any reason in the past year), or non-migraine control subjects (had a medical visit for any reason within the past year, but did not meet criteria for SM or PM). Respondents were categorized as PM (n = 1252; 14.6%) if they fulfilled all but one of criteria for migraine without aura. To determine the missing feature which led to a diagnosis of PM, we identified the missing feature by looking at their number of life-time attacks (less than five attacks during their life), duration of headache (<4 h or > 72 h), pain features (headache did not fulfil two of four migraine pain characteristics) and associated symptoms (absence of nausea and vomiting, and the absence of at least one of photophobia and phonophobia). If a patient had two headache types and at least one type met criteria for migraine or tension-type headache, patients were so classified. Most individuals classified with PM (88.7%) had just one type of headache, and this headache met criteria for PM. The remaining 11.3% had two distinct types of headache that met criteria for PM. In these individuals we evaluated the missing diagnostic feature for the more severe of their two types of PM.
A control code of ‘0’ or ‘1’ was assigned to each of the 22 666 individuals in the call list. Once the call list was randomized, every sixth record was assigned a code of ‘1’ to designate that the subject was potentially eligible for inclusion in the control population. Therefore, respondents were categorized as controls (n = 960) if they had previously been assigned a code of ‘1’, had a medical visit for any reason within the past year, and did not meet the SM or PM case definitions. Survey respondents that did not meet the case definition for SM or PM, and had previously received a code ‘0’, were considered a non-case/non-control (n = 5102) and did not receive a follow-up interview.
Assessment of diagnosis and treatment
After completing survey data collection, we linked member survey responses to the matching 24-month medical and pharmacy claims records. The diagnosis was established after the telephone interview. The medical diagnosis and treatment were assessed based, respectively, on the medical and pharmacy claims. The individual variables included in the medical and pharmacy claims datasets were combined into summary variables.
The medical claims variables were defined as follows:
Any headache diagnosis: any headache in-patient or out-patient claims, in any diagnosis field. We included here diagnosis of migraine (ICD-9-CM = 346.xx), headache not otherwise specified (ICD-9-CM = 784.0), tension headache (ICD-9-CM = 307.81), headache secondary to lumbar puncture (ICD-9-CM = 349.0), and menopausal headache (ICD-9-CM = 627.2).
Primary migraine in-patient diagnosis: migraine code (ICD-9 = 346.xx) in in-patient primary diagnosis field.
Any migraine in-patient diagnosis: migraine code (ICD-9 = 346.xx) in any in-patient diagnosis field.
Primary migraine out-patient diagnosis: migraine code (ICD-9 = 346.xx) in out-patient primary diagnosis field.
Any migraine out-patient diagnosis: migraine code (ICD-9 = 346.xx) in any out-patient diagnosis field.
Pharmacy variables assessed prescribed medication only. Therefore, OTC medication used by the subjects was not captured in the summary pharmacy variables. Additionally, the pharmacy variables did not discriminate between new prescriptions or refills, or assess the number of prescriptions per patient. The pharmacy-derived variables were defined as follows:
Migraine drugs: ICD-9 codes for any triptan, dihydroergotamine (DHE), or ergotamine compound; drugs in this group may be used for other conditions but are used overwhelmingly for migraine.
Migraine analgesics: ICD-9 codes for medications containing butalbital or isometheptene. Drugs in these group contain analgesics and are used largely for migraine.
Antiemetics: ICD-9 codes for metochlopramide and prochlorperazine.
Non-specific analgesics: ICD-9 codes for acetaminophen, acetylsalicylic acid, non-steroidal anti-inflammatory drugs (NSAIDs), and narcotics. Drugs in this group are used for migraine, other headaches and other pain conditions.
NSAIDs: ICD-9 codes for NSAIDs. This is a subgroup of non-specific analgesics and prescriptions for NSAIDs were included in both categories (non-specific analgesics and NSAIDs).
Narcotics: ICD-9 codes for narcotics. Similarly, this category is a subgroup of non-specific analgesics and prescriptions for narcotics were included in both categories (non-specific analgesics and narcotics).
Migraine preventives. ICD-9 codes for β-blockers, antidepressants, calcium channel blockers, antiepileptic drugs, botulinum toxin.
Statistical analysis
Most of the analysis was descriptive and could be presented via simple cross-tabulations and frequencies. To compare categorical variables, Pearson's χ2 statistics were used. SAS 8.2 for Windows was used for all statistical analysis (SAS Institute, Cary, NC, USA).
Results
Participant characteristics
Demographics were described in detail elsewhere (6). In brief, among the 8579 respondents, 5557 (64.8%) were female; 3508 (59.1%) were 18–45 years old and 5569 (64.9%) were caucasian. A total of 1265 (14.7%) respondents had SM, including 1067 (prevalence of 19.2%) females and 198 (6.6%) males (gender ratio of 3.06). A total of 1252 (14.6%) cases fulfilled the criteria for PM, including 882 (15.9%) females and 370 (12.2%) males (gender ratio of 2.3). The prevalence was higher in females than in males for both SM (19.2% vs. 6.6%) and PM (15.9% vs.12.2%). The prevalence was similar in caucasian vs. non-caucasian for SM (15.3% vs. 14.3%) and PM (15.2% vs. 14.4%). Prevalence peaked in early middle life for both SM (26–35 years, 19%) and PM (36–45 years, 16.7%). AM had a prevalence of 29.2% (Table 1).
Distribution of socio-demographic characteristics by migraine status

Subjects diagnosed with PM were missing a single major criterion for migraine; most did not have the required associated symptom (i.e. nausea/vomiting, or photophobia and phonophobia) criteria for migraine (1027, 82.0%). In 208 (16.6%), the subjects did not have two of four required pain features. Just nine (0.7%) had fewer than five attacks and eight (0.6%) did not meet the 4–72 h duration criteria.
The crude prevalence of migraine was highest in the 26–45-year-olds for SM and PM.
Medical diagnosis
Any migraine claim in an out-patient field was assigned to 234 (18.4%) SM sufferers, 39 (3.1%) PM sufferers, and eight (0.6%) controls (Table 2). Any migraine claim in an in-patient field was assigned to six (0.4%) SM sufferers, no PM sufferers and no controls (Table 2). Therefore, just 240 (18.9%) SM, 39 (3.1%) PM sufferers and eight controls (0.6%) received any migraine claim in an in-patient or out-patient field (Table 2).
Number and percentage of participants meeting claims-based definitions
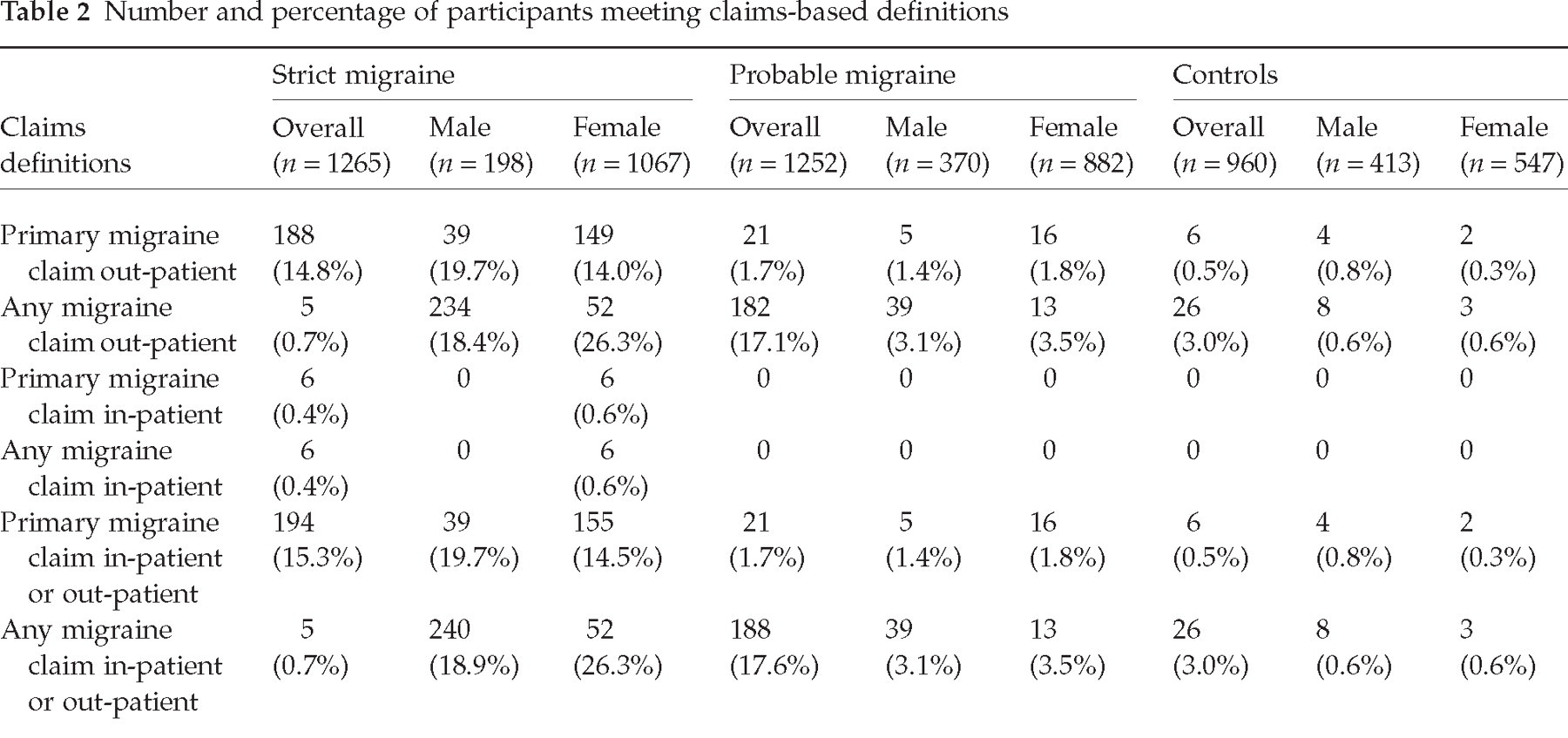
Pooling SM and PM together (AM), any migraine claim in an out-patient field was assigned to 273 (10.8%) participants and any migraine claim in an in-patient field was assigned to six (0.5%) participants (Table 2). Any migraine claim in either an out-patient or in-patient field was assigned to 279 (11.1%) participants (Table 2).
Any headache diagnosis was assigned to 504 (39.8%) of the SM and 260 (20.8%) of the PM sufferers (respectively 40.2% and 23.8% in females, and 37.9% and 13.5% in males), but also for 147 (12.5%) of the controls (17% in females, 6.5% in males).
We also assessed, within SM, PM and controls, the likelihood of ever having received a medical migraine diagnosis (Table 3). While 52.9% of the SM sufferers included in this study had a previous diagnosis of migraine, just 16.1% of those with PM ever received a diagnosis of migraine, compared with 6.9% of the controls (P < 0.0001, Pearson's χ2).
Self reported previous diagnosis of migraine within subjects with current strict migraine, probable migraine, and controls

151 subjects did not provide this information.
Medical treatment
There were claims for migraine drugs (ICD-9 code for triptans or ergot compounds) for just 140 (11.1%) SM sufferers (7.6% in men and 11.7% in women), and 34 (2.7%) of the PM sufferers (1.6% in men and 3.2% in women). A total of seven (0.8%) controls also received a migraine drugs claim (1.2% in men and 0.4% in women) (Table 4). Migraine analgesics (butalbital and isomethepthene compounds) were prescribed for 80 (6.3%) SM sufferers, 27 (2.2%) PM sufferers, and seven (0.7%) controls. Antiemetics were prescribed for just 38 (3%) SM and 21 (1.7%) PM sufferers, but also for 14 (1.5%) controls. Non-specific analgesics were used for 55.8% SM and 48.8% PM sufferers, as well as for 46.5% of the controls. Similarly, NSAIDs were used for 50.9% of SM and 42.5% of PM sufferers as well as for 41.2% of controls; and narcotics, for 20.7%, 18% and 17%, respectively (Table 4).
Number and percentage of respondents meeting selected pharmacy claims definitions
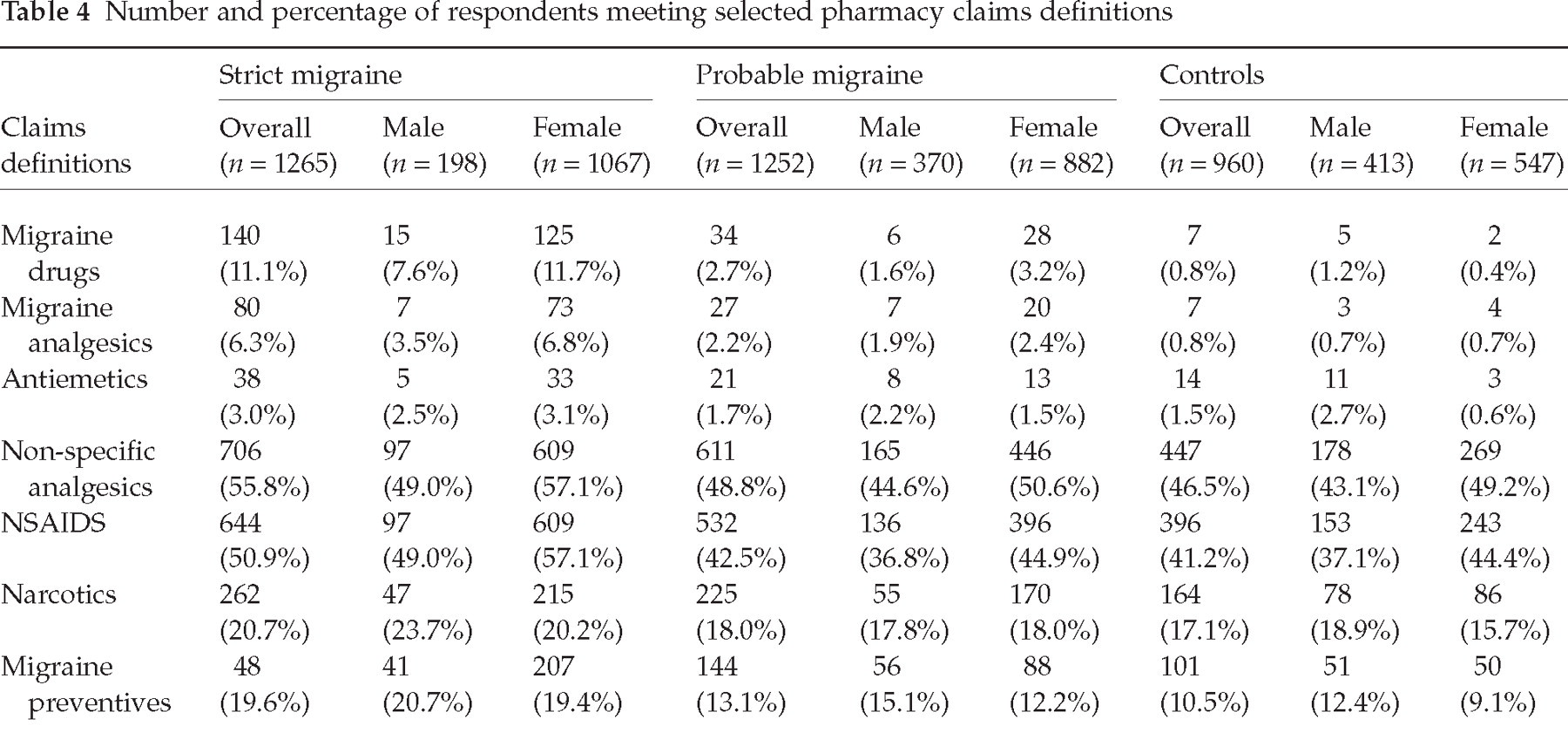
Migraine preventives were used for a larger number of SM sufferers (19.6% overall; 20.7% of men and 19.4% of women) and PM sufferers (respectively 13.1%, 15.1% and 12.2%), but also for controls (10.5% overall, 12.4% of men and 9.1% of women).
Accordingly, a minority of the AM sufferers ever received migraine drugs claim (174, 6.9%), migraine analgesic claims (107, 4.2%) or migraine preventives (392, 15.6%); 1317 (52.3%) of AM sufferers received a code for non-specific analgesics, 1117 (46.7%) for NSAIDS, and 487 (19.3%) for narcotics.
Discussion
In this health-plan-based study both SM and PM were prevalent disorders. A population-based study assessing 4000 4-year-old males and females using the ICHD-1 criteria found that the lifetime prevalence of PM was 2.5% with a female/male ratio of 1.2 : 1 (2). The 1-year period prevalence in the American Migraine Study II was similar (2.6%, 6.3% female) (3). In a French population study, Henry and colleagues screened 10 585 subjects aged ≥ 15 years and found a standardized prevalence of migraine (IHS categories 1.1 and 1.2) of 7.9% (11.2% for women and 4.0% for men) and 9.1% for PM (IHS category 1.6) (17). Prevalence of PM may be higher in the current study than in previous reports because the sample enrolled health-plan members using medication services at the ages of peak risk as discussed below.
Our data show that both SM and PM are underdiagnosed and suboptimally treated despite having access to medical care and prescription drugs in a health plan. Just 15.4% SM and 1.7% PM sufferers received an in-patient or out-patient primary migraine claim in the previous 24 months. Any headache diagnosis was assigned to just 39.8% of the SM and 20.8% of the PM sufferers. Around 50% of the SM sufferers and the vast majority of the PM sufferers self-reported not ever receiving a medical diagnosis of migraine in the past. Migraine drugs claims were filled by just 11.1% of the SM and 2.7% of the PM sufferers (0.7% of the controls). Non-specific analgesics were filled by 55.8% SM and 48.8% PM sufferers, as well as 46.5% of the controls. Preventives were filled by 19.6% and 13.1% of the SM and PM sufferers, but also controls (10.5%), indicating that they might be used for other medical reasons. One possible explanation for the extremely low diagnosis rate of PM is that doctors probably perceive the associated symptoms (nausea, photophobia and phonophobia) as the distinguishing features of migraine. Since most PM sufferers were so diagnosed because they missed the associated symptoms, this may offer one explanation to our findings.
Caution is required when interpreting these data. First, only participants who were members of a health plan and received medical care in the last 24 months were eligible to participate. This sample may not be fully representative of the general population; the lowest and highest socio-economic stratum of the population are probably under-represented in this sample comprising subjects covered by HMO health insurance. Also, as we and others have shown, many migraine sufferers do not consult healthcare professionals explicitly for headache (17, 19, 20). Second, the SM and PM groups were defined using a telephone interview that was based on IHS criteria, not by clinical assessment. The telephone interview has been well validated, both in the UK and the USA, and has excellent operating characteristics for migraine (19); nonetheless, classification errors are possible. The telephone interview has not been assessed for PM. Third, most of the migraine therapeutic armamentarium is composed of non-specific acute treatments (e.g. OTC and prescription analgesics) and preventive treatments (e.g. β-blockers, antiepileptic medication, antidepressants), which are widely used for problems other than migraine (21, 22). Most migraine sufferers do not receive prescription drugs, and most of the prescription drugs they receive are not specific for migraine, leading to difficulty in identifying migraine using traditional methods of analysing claims and pharmacy data (23, 24). We tried to address this issue by comparing prescription claims in SM and PM sufferers with controls. Finally, our data do not suggest that every headache sufferer assessed should have received a diagnosis or a prescription, because we did not assess the proportion of subjects that sought care for headache.
In a recent study, we showed many similarities between PM and SM sufferers, including a higher prevalence of females than males, a peak of prevalence in middle life, and a lower prevalence in African-Americans. We also showed that both PM and SM sufferers have reduced quality of life and increased disability compared with controls (6). Here, we have shown that both migraine subtypes are underdiagnosed and suboptimally treated. Therefore, AM is an underestimated and still poorly recognized disorder. Educational strategies should focus on physician education, addressing diagnosing the full spectrum of migraine, and physician management of migraine with migraine-specific therapy in appropriate patients. Further research identifying the clinical consequences of underdiagnosis and suboptimal treatment of migraine is warranted.
Footnotes
Acknowledgements
This manuscript and the probable migraine initiative are supported by GSK. Previous collection of database was sponsored by AstraZeneca.