
Abstract
Background
Although probable migraine (PM) is common among headache sufferers, there is little knowledge of the prevalence and impacts of comorbid anxiety and depression in patients with PM. We assessed the prevalence and impact of anxiety and depression among PM sufferers in the general population.
Methods
We recruited Korean individuals aged 19–69 years via stratified random sampling and assessed headache type, anxiety, and depression among them using structured interviews.
Results
In a representative sample of 2695 individuals, 143 (5.3%) and 379 (14.1%) had migraine and PM, respectively. Fewer patients with PM had anxiety (17.7% vs. 30.1%, p = 0.002) and depression (8.7% vs. 16.8%, p = 0.007) compared to those with migraine. Prevalence of anxiety and depression was lower in people with PM than in those with migraine in univariable analysis, but insignificant after including headache intensity and headache frequency for adjustment. Headache frequency, headache intensity, and impact of headache were significantly higher among PM and migraine patients with anxiety and depression than among those without.
Conclusions
The prevalence of anxiety and depression was lower among individuals with PM compared to those with migraine. However, they were still prevalent and associated with an exacerbation of symptoms among individuals with PM.
Background
Among people who suffer from headaches, many experience migrainous headaches that fail to strictly fulfil the diagnostic criteria of migraine without aura (code 1.1) or with aura (code 1.2) according to the third beta edition of the International Classification of Headache Disorders (ICHD-3 beta), which we herein refer to as migraine (1,2). Some of these cases meet the criteria for probable migraine (PM, codes 1.5.1 and 1.5.2), which is a subtype of migraine that meets all but one criterion for migraine (2). PM has been reported to be a common primary headache disorder, with an approximately 10% prevalence rate according to various population-based studies (3–5). Epidemiological studies have shown that individuals with PM experience milder pain intensity during headaches compared to those with migraine (4,6).
Migraine often presents with various comorbid psychiatric conditions such as anxiety and depression (7,8). Notably, among individuals with migraine, the frequency of headache and severity of disability appear to be greater when such psychiatric comorbidities are present than when they are not (7,8). Anxiety is the most common psychiatric comorbidity of migraine, with a prevalence rate of 25.5%–57.6% (7–11). Patients with migraine and comorbid anxiety are more likely to suffer from disability and poor quality of life than are those with migraine but no comorbid anxiety (8,10). Depression is another common comorbidity of migraine, with a prevalence up to 29.1% among migraine sufferers (5).
Although anxiety and depression appear to be closely associated with migraine, the prevalence and clinical impact of anxiety and depression among individuals with PM had rarely been reported (8). Our hypothesis was that (1) levels of anxiety and depression would be lower among individuals with PM compared to those with migraine; and (2) PM patients with anxiety and depression would be shown more profound symptoms compared to PM patients without anxiety and depression. To clarify these, we aimed to (1) describe the prevalence of anxiety, depression, migraine, and PM in a general population of Korea; (2) compare the prevalence rates of anxiety and depression between individuals with PM and those with migraine; and (3) examine differences in headache frequency, intensity and quality of life of patients with migraine and PM according to their anxiety and depression status.
Materials and methods
Survey
We used data from the Korean Headache-Sleep study. This study was a nationwide, cross-sectional survey of headaches and sleep characteristics among the adult Korean population (aged 19–69 years). Although the study design and methods have been previously described in detail (12,13), it is briefly as follows. We adopted a two-stage systematic random sampling method for all Korean territories except Jeju-do. Specifically, we sampled individuals in proportion to the population distribution. Participants were stratified by age, gender, and occupation. To minimise potential interest bias, we informed candidates that the survey topic was ‘social health issues’ rather than headaches. After sampling, trained interviewers used a questionnaire to diagnose headache, anxiety, and depression via face-to-face interviews at the participants’ homes. All interviewers were employed by Gallup Korea and thus had previous experience in conducting social survey interviewing. Notably, none of the interviewers were medical personnel. Data for the Korean Headache-Sleep study were collected from November 2011 to January 2012. The study was approved by the institutional review board/ethics committee of Hallym University Sacred Heart Hospital and was performed in accordance with the ethical standards laid out in the 1964 Declaration of Helsinki and its subsequent amendments (14). Written informed consent was obtained from all participants before each interview.
Case definition of migraine and PM
Diagnoses of migraine and PM were based on criteria (a) to (d) for migraine without aura (code 1.1) in the ICHD-3 beta ((a) five or more attacks in a lifetime; (b) attack duration of 4–72 hours; (c) any two of the four typical headache characteristics (i.e. unilateral pain, pulsating quality, moderate-to-severe pain intensity, and aggravation by routine physical activity); and (d) attacks associated with at least one of the following: nausea, vomiting, or both photophobia and phonophobia). Participants who met all of these criteria were considered to have migraine, whereas participants who met all criteria except one were considered to have PM. Cases with headaches that met criteria both for PM and tension-type headaches did not receive a PM diagnosis, as per the ICHD-3 beta. Because migraine and PM with aura (codes 1.2.1 and 1.5.2, respectively) are difficult to document using the questionnaire method, we did not investigate the presence of aura (15). As such, individuals who had migraine or PM with aura would be included among those with migraine or PM without aura, respectively. Accordingly, ‘migraine’ included migraine with and without aura (codes 1.1 and 1.2) and “PM” included PM with and without aura (codes 1.5.1 and 1.5.2). These questions have been previously found to have 75.0% sensitivity and 88.2% specificity in comparison with doctors’ diagnoses obtained from additional telephone interviews (16).
Case definition of anxiety and depression
We used the Goldberg Anxiety Scale to diagnose anxiety among participants. This comprises four screening items and five supplementary items (17,18). Individuals who gave positive answers for two or more screening items and five or more of all scale items were diagnosed with anxiety. The Korean version of the scale has an 82.0% sensitivity and 94.4% specificity for diagnosing anxiety (18), and shows good correlations with the State-Trait Anxiety Inventory, a highly valid tool for assessing anxiety (19).
The Patient Health Questionnaire-9 was used to diagnose depression (20). Participants who had scores of 10 or more on this measure were considered to have depression. The Korean Patient Health Questionnaire-9 has an 81.1% sensitivity and 89.9% specificity (21). Additionally, we investigated the visual analogue scale for headache and Headache Impact Test-6 scores for quality of life among patients with migraine and PM.
Analyses
According to the definitions of migraine and anxiety, the one-year prevalence rates of both are presented as the number of cases per 100 people. Age- and gender-specific prevalence rates were also calculated. The Kolmogorov-Smirnov test was used to confirm the normality of the distribution; after the normality was confirmed, we utilised Student’s t-test, Chi-square test, and Mann–Whitney U test for comparison of prevalence rates where appropriate. A significance level of p < 0.05 was set for all analyses. The results were analysed using the Statistical Package for the Social Sciences 22.0 (SPSS 22.0; IBM, Armonk, NY, USA).
We calculated the odds ratios (ORs; 95% confidence intervals (CIs)) for the occurrence of anxiety and depression in patients with PM compared to those with migraine using univariable and multivariable logistic regression analyses. In the univariable analyses, we modelled the ORs for PM vs. migraine without adjusting for covariates. In the multivariable analyses, we developed four models. In Model 1, adjustment conducted for the sociodemographic variables (age, gender, size of residential area and education level). Model 2 included headache frequency to Model 1. Model 3 incorporated Model 1 and headache intensity. Finally, Model 4 incorporated the sociodemographic variables, headache frequency and headache intensity.
As with most survey sampling designs, there were missing data (resulting from non-response) for several variables. All of the reported results are based on the available data; as such, the total numbers of some variables diverge from 2695 because of missing data for that particular variable. We did not employ imputation techniques because we wanted to minimise non-response effects (22).
Results
Survey
Interviewers approached 7430 individuals, of whom 3114 agreed to participate in the survey (rejection rate 58.1%). After 419 individuals were suspended participation in the interview, 2695 patients completed the survey (cooperation rate 36.3%; Figure 1). We found no significant differences in the distributions of age, gender, size of residential area, and educational level from those of the general population of Korea (Figure 1 and Table 1).
Flowchart depicting the participation of individuals in the Korean Headache-Sleep Study. Sociodemographic characteristics of survey participants; the total Korean population; and cases identified as having migraine, probable migraine, anxiety, and depression. N: number; CI: confidence interval. Variables are presented as number (%) or number, % (95% confidence interval). Compared with gender, age group, size of residential area, and education level between the sample of the present study and the total population of Korea.

Prevalence and clinical characteristics of migraine and PM
Of the 2695 participants, 1299 (47.2%) had had at least one headache attack, and 147 (5.4%) were classified as having migraine during the previous year. The prevalence of migraine was highest in the 30–39 age group (7.0%) (Table 1). A total of 379 (14.1%) individuals with PM had had at least one attack during the previous year (Table 1). The prevalence rates of PM were highest in the 30–39 and 40–49 age groups (16.8%). Among the 379 individuals diagnosed with PM, 339 (89.5%) did not meet criterion (b) (typical headache duration), 29 (7.7%) did not meet criterion (c) (typical headache characteristics), and 11 (2.8%) did not meet criterion (d) (associated symptoms) (2). Visual analogue scale score for headache intensity was significantly lower among individual with PM than those with migraine (5.2 ± 1.7 vs. 6.2 ± 1.9, p < 0.001). Headache frequency per month was not significantly different between migraine and PM (2.8 ± 5.6 vs. 3.9 ± 6.3, p = 0.060).
Prevalence of anxiety and depression among patients with migraine and PM
A total of 268 (10.0%) individuals were classified as having anxiety and 116 participants (4.3%) were classified as having depression (Table 1). Of the 143 patients with migraine, 43 (30.1%) had anxiety and 24 (16.8%) had depression. Moreover, of the 379 participants with PM, 67 (17.7%) had anxiety and 33 (8.7%) had depression. The prevalence rates of anxiety (p = 0.002) and depression (p = 0.008) were significantly lower among patients with PM than among those with migraine.
Differences in anxiety and depression between migraine and PM according to sociodemographic variables, headache frequency and headache intensity
Univariable and multivariable odds ratios of anxiety and depression for migraine and probable migraine as a function of sociodemographic variables, headache frequency and headache intensity in the population.

PM: probable migraine; OR: odds ratio; CI: confidence interval.
Variables are presented as number (%).
Adjusted for gender, age, size of residential area and educational level.
Adjusted for gender, age, size of residential area, educational level and headache frequency.
Adjusted for gender, age, size of residential area, educational level and headache intensity.
Adjusted for gender, age, size of residential area, educational level, headache frequency and headache intensity.
Prevalence of anxiety and depression among patients with migraine and PM according to headache frequency
Prevalence and odds ratios a of anxiety (a) and depression (b) among individuals with migraine and probable migraine according to headache frequency.
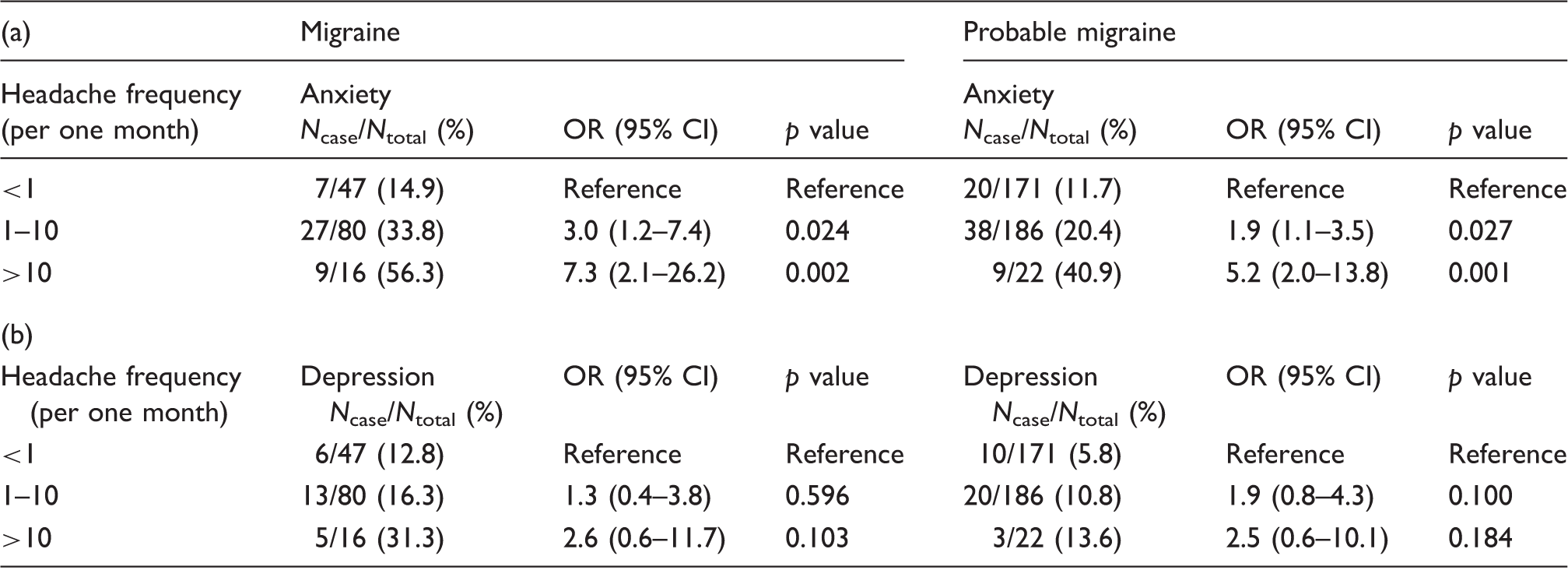
OR: odds ratio; CI: confidence interval.
Adjusted for gender, age, size of residential area and education level.
Clinical characteristics of migraine and PM patients with anxiety and depression
Mean headache frequency, headache pain intensity (VAS score), and Headache Impact Test-6 score according to anxiety (a) and depression (b) status.
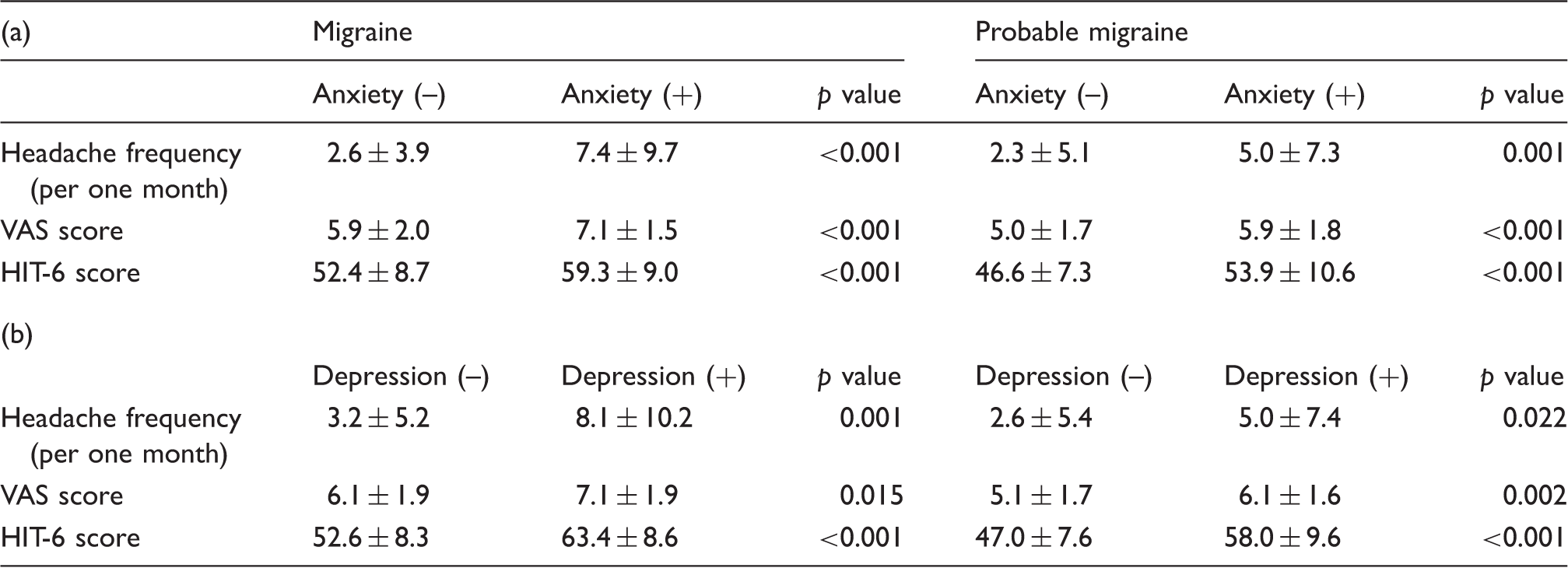
VAS: visual analogue scale of headache pain intensity; HIT-6: Headache Impact Test.
Discussion
Our key findings are as follows. First, the prevalence rates of anxiety, depression, migraine, and PM in a representative sample of the Korean population were 10.0%, 4.3%, 5.3%, and 14.1%, respectively. Second, among participants with PM, 18.1% had anxiety and 8.9% had depression; these prevalence rates were significantly lower than were those for individuals with migraine. Finally, headache frequency and pain intensity and Headache Impact Test-6 scores were higher among migraine and PM patients with anxiety and depression than among those without these conditions.
The one-year prevalence rates of PM according to previous studies—most of which were conducted in North American or European countries—ranged from 4.3% to 14.6% (1,3–5,23–26). Thus, the prevalence rate we found (14.1%) was similar to those observed previously. The one-year prevalence data of PM are available for only three Asian countries—Hong Kong, Singapore, and Korea (6,27,28)—and ranged from 6.2% to 11.5%, making them similar or somewhat lower than the rates we observed. This discrepancy might be explained by differences in cultural background, survey method, and socioeconomic status.
The one-year prevalence of migraine (5.3%) was lower in the present study than in previous studies from European (10–25%) and North American (9–16%) countries (29). In contrast, the prevalence rates were similar to those in previous studies in Asian countries, which ranged from 4.7% to 9.1% (6,30). We also noted that the prevalence rates of anxiety and depression were similar to those previously reported, ranging from 5.6% to 19.3% for anxiety and 3.6% to 8.8% for depression (31–34). Although these ranges are somewhat large, they nonetheless suggest that our findings are reliable. As noted above, few studies have looked at the relation of anxiety and depression with PM.
A population-based study in France reported that the prevalence rates of anxiety (46.8% vs. 45.9%) and depression (22.8% vs. 21.9%) did not significantly differ between migraine and PM, and that headache pain intensity and headache-related disability were greater among individuals with migraine than among those with PM (4). However, this past study did not investigate differences in the clinical characteristics of PM according to anxiety and depression status. In contrast to this previous study (4), we found that anxiety and depression were less prevalent among those with PM compared to those with migraine.
In multivariable analyses of the present study, prevalence of anxiety and depression was lower in participants with PM than in those with migraine in univariable analysis, but was not significant after including headache frequency and headache intensity in adjustment of the multivariable analysis. These findings suggest that the decreased effect of anxiety and depression in individuals with PM compared to individuals with migraine may be attenuated or be more strongly influenced by other factors such as headache frequency and headache intensity.
We posit several possible explanations for the difference in the prevalence rates of anxiety and depression between migraine and PM. One is that PM shares with migraine a common vulnerability to anxiety and depression. A twin study revealed that anxious depression and migraine share certain genetic factors (35). Furthermore, longitudinal studies have indicated a close association between depression and migraine, thus suggesting a common underlying vulnerability (36), given that most PM patients did not meet criterion (b) (typical headache duration) but still had migrainous headache features (4,6). That is, PM may be a mild form of migraine. As such, it may be less influenced by common vulnerability and thereby lead to less severe anxiety and depression than migraine. To confirm this hypothesis, further longitudinal study is needed. Another possible explanation is the fact that PM has shorter attack durations and milder symptoms (e.g. nausea, vomiting, photophobia) which may lead to relatively less impairment in mental functioning and thus relatively less severe anxiety and depression.
We also investigated anxiety and depression prevalence according to headache frequency among individuals with PM; notably, anxiety was prevalent among PM patients with frequently occurring headaches than among those with infrequent headaches; this same pattern was also found for migraine patients. These higher prevalence rates among PM patients with more frequent headaches add support to the association of anxiety with PM.
This study has several limitations. First, although the questionnaire used for diagnosis of migraine and PM had been validated for individuals with migraine, it has never been validated for those with PM. Furthermore, the diagnostic criteria for PM were based on the ICHD-3 beta criteria, wherein a diagnosis of PM is indicated by fulfilling all but one of the migraine criteria. However, the questionnaire itself is based on the diagnostic criteria of the ICHD-3 beta for migraine and PM; nevertheless, it was deemed appropriate to use since specific validation of PM was not considered necessary. Second, we used the Goldberg Anxiety Scale to diagnose anxiety. This scale includes one question about a participant’s headaches or neck aches. Based on these questions, people with migraine may have obtained higher Goldberg Anxiety Scale scores, and hence be more likely to be diagnosed as having anxiety. However, we believe that our results reliably reflect comorbidity rates for anxiety and migraine for the following reasons: (1) the Korean version of the Goldberg Anxiety Scale has been validated with high sensitivity and specificity (18), and (2) individuals with migraine showed a higher prevalence of anxiety compared to those with PM, who might have also responded positively to the item on head and neck aches. Third, although the present study is population based and had a low sampling error, its statistical power was limited in terms of examining the subgroups. In other words, the nonsignificant results for subgroup analysis, such as according to age, education level, or size of residential area, could merely be the result of the limited sample size. Lastly, we did not separately diagnose migraine with aura and migraine without aura because it is very difficult to diagnosis in epidemiological studies (15).
Despite its limitations, the study also has several strengths. First, our study was based on clustered random sampling proportional to the Korean population. Combined with the low sampling error, this approach allowed us to accurately describe rates of anxiety, depression, PM, and migraine among the Korean adult population. Second, we investigated both anxiety and depression, which are common psychiatric comorbidities among individuals with migraine, and assessed clinical characteristics of migraine and PM according to anxiety and depression status. Considering both the limitations and strengths, we believe that the present study was able to accurately describe the rates of anxiety and depression among participants with migraine and PM.
Conclusion
Prevalence of anxiety and depression was lower among individuals with PM compared to individuals with migraine, and these differences of prevalence were diminished after adjusting for headache frequency and headache intensity. However, anxiety and depression were still prevalent and associated with worse symptoms among the former group. Our findings suggest that proper diagnosis and treatment of anxiety and depression are needed for better management of PM.
Clinical implications
Approximately 1/5 and 1/10 of individuals with probable migraine (PM) had anxiety and depression, respectively. Anxiety and depression were more prevalent among individuals with PM with more frequent headaches than among those with less frequent headaches. People with PM who had anxiety and depression showed more severe symptoms of headache than did those without anxiety or depression. Although prevalence rates of anxiety and depression among PM sufferers were lower than migraine sufferers, a significant proportion of individuals of PM had anxiety and depression. Our findings suggest that proper diagnosis and treatment of anxiety and depression are needed for better management of PM like migraine.
Footnotes
Acknowledgement
The authors would like to thank Gallup Korea for providing technical support for the Korean Headache Survey.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: this study was supported by a 2011 grant from the Korean Academy of Medical Sciences.