
Abstract
We semiquantitatively analysed radionuclide cisternography in three patients with spontaneous cerebrospinal fluid (CSF) leakage diagnosed by typical symptoms and magnetic resonance imaging findings before and several months after treatment with epidural blood patch. Radioactivity in the whole CSF space was measured immediately after and at 1, 5, 7 and 24 h after intrathecal injection of 111In-diethylenetriaminepentaacetic acid (DTPA). Initial findings included the vague appearance of leakage in the thoracic spine in two patients, early bladder filling at 1 h in one and a lack of tracer filling into the high cranial convexity in all three. The radioactivity count rapidly decreased within several hours after injection and reached 20± of the initial value at 24 h. In contrast, no rapid decrease was observed after treatment and more than 50± of tracer remained at 24 h after injection. Semiquantitative analysis of tracer clearance may provide additional information in the diagnosis of CSF leakage, especially with no obvious qualitative findings.
Introduction
Radioisotope (RI) cisternography is a key in diagnosis of cerebrospinal fluid (CSF) leakage causing intracranial hypotension syndrome (1). Extradural accumulation of tracer is direct evidence of leakage, while early excretion into urine, or the absence of the intracranial ascent of tracer in RI cisternography, are considered indirect findings suggestive of CSF leakage (2, 3). However, the sensitivity of RI cisternography is low, and approximately 30% of cases show no direct sign (4, 5). This is due partly to the low spatial resolution of the study; however, flow rate is another factor significantly affecting the results. The rate of CSF leak can vary tremendously and evidence of leak cannot be confirmed on RI examination when leak flow is slow or intermittent (6, 7). Furthermore, these qualitative assessments are basically observer dependent and sometimes equivocal, and no standards have been established (1). In fact, reports of visualization timing of unusual early bladder filling have given values varying from 45 min to 7 h after injection (8–11). Threshold or level and width of window during imaging strongly affect the visualization of these findings and early visualization of the bladder can be seen even in patients without CSF leakage (12). Thus, qualitative RI cisternography sometimes gives inconclusive results in the detection of CSF leakage and patients without overt qualitative findings may be overlooked.
We conjectured that quantitative evaluation of tracer clearance from the CSF space may provide a more accurate means of diagnosing CSF leakage by establishing normal/abnormal threshold on tracer kinetics, although little has been reported on this. Here, we report three cases of spontaneous CSF leakage in which tracer kinetics was semiquantitatively analysed before and after treatment.
Patients and methods
Clinical features of the three patients are summarized in Table 1. All complained of acute onset of severe orthostatic headache associated with hearing impairment or tinnitus. One patient had disturbed consciousness due to a secondary accompanying subdural haematoma during the clinical course before admission. None had a preceding episode such as head or neck trauma, physical exercise or vigorous coughing. Spontaneous CSF leakage headache was diagnosed based on typical orthostatic headache combined with hearing impairment, low CSF open pressure and diffuse dural enhancement on magnetic resonance imaging (MRI). Two patients were initially treated with bed rest and intravenous hydration, and one with subdural drainage. Since this initial treatment was not effective, RI cisternography and treatment with epidural blood patches (EBP) were performed. All responded well to EBP and the symptoms were completely relieved within several days.
Summary of patients with spontaneous intracranial hypotension

OH, Orthostatic headache; DOC, disturbance of consciousness; MRI, magnetic resonance imaging; RIC, radioisotope cisternography; EBF, early bladder filling of tracer detected within 1 h of delivery; LCF, lack of high convexity filling shown 24 h after delivery; EBP, epidural blood patch. Relative radioisotope (RI) activity is presented with a ratio of against the initial value.
RI cisternography with 37 MBq of 111In-diethylenetriaminepentaacetic acid (DTPA) was performed by the intrathecal lumbar injection of tracer using a 25-G pencil-type spinal needle. Tracer in the needle was flushed out with a small amount of saline to prevent iatrogenic pushing out of the tracer into the epidural space during withdrawal of the needle. Whole-body planar scintigraphic images were obtained with a single headed gamma camera immediately after and 1, 5, 7–8 and 24 h after injection. Distribution of the tracer was continuously imaged during the first hour and successful intrathecal injection was confirmed in all by observing the rod-shaped accumulation of tracer with gradual ascent along with the spinal axis. Patients were kept recumbent in the RI room for 1 h after injection, then released to the ward and kept under bed rest without urinary voiding for a further 5–6 h. One patient was kept in bed rest for the entire day because continuous subdural drainage had already started. Tracer efflux from the dural sac, the detection of considerable amounts of tracer in the bladder within 1 h of delivery and the lack of tracer filling in the high cranial convexity within 24 h were considered as signs of abnormal CSF kinetics suggestive of leakage from the spinal dural sac. For semiquantitative assessment of RI excretion, RI activity was counted in the range of the whole CSF space. After correcting for radioactive decay of the tracer, the ratio of RI count to that at delivery was plotted against time. Follow-up RI cisternography was performed several months after treatment when complete cure was confirmed.
RI cisternographic findings
Lack of cranial ascent of tracer at 24 h after injection was observed in all three patients. In two patients, the tracer ascended as high as the anterior interhemispheric fissure and the bilateral Sylvian fissures but not into the high cranial convexity, resulting in a trident-like accumulation in the anteroposterior view (Fig. 1). In the patient with subdural haematoma, the tracer reached only as far as the cisterna magna at 24 h (patient 3). The urinary bladder was mildly delineated at 1 h in one patient (Fig. 1). Subtle extradural accumulation of tracer indicative of CSF leakage at the thoracic spine was suspected in two and no leakage was revealed in patient 2. These abnormal findings disappeared completely after treatment in all patients. After treatment, the cranial cavity was invariably visualized as a round shadow at 24 h in all patients (Fig. 2).
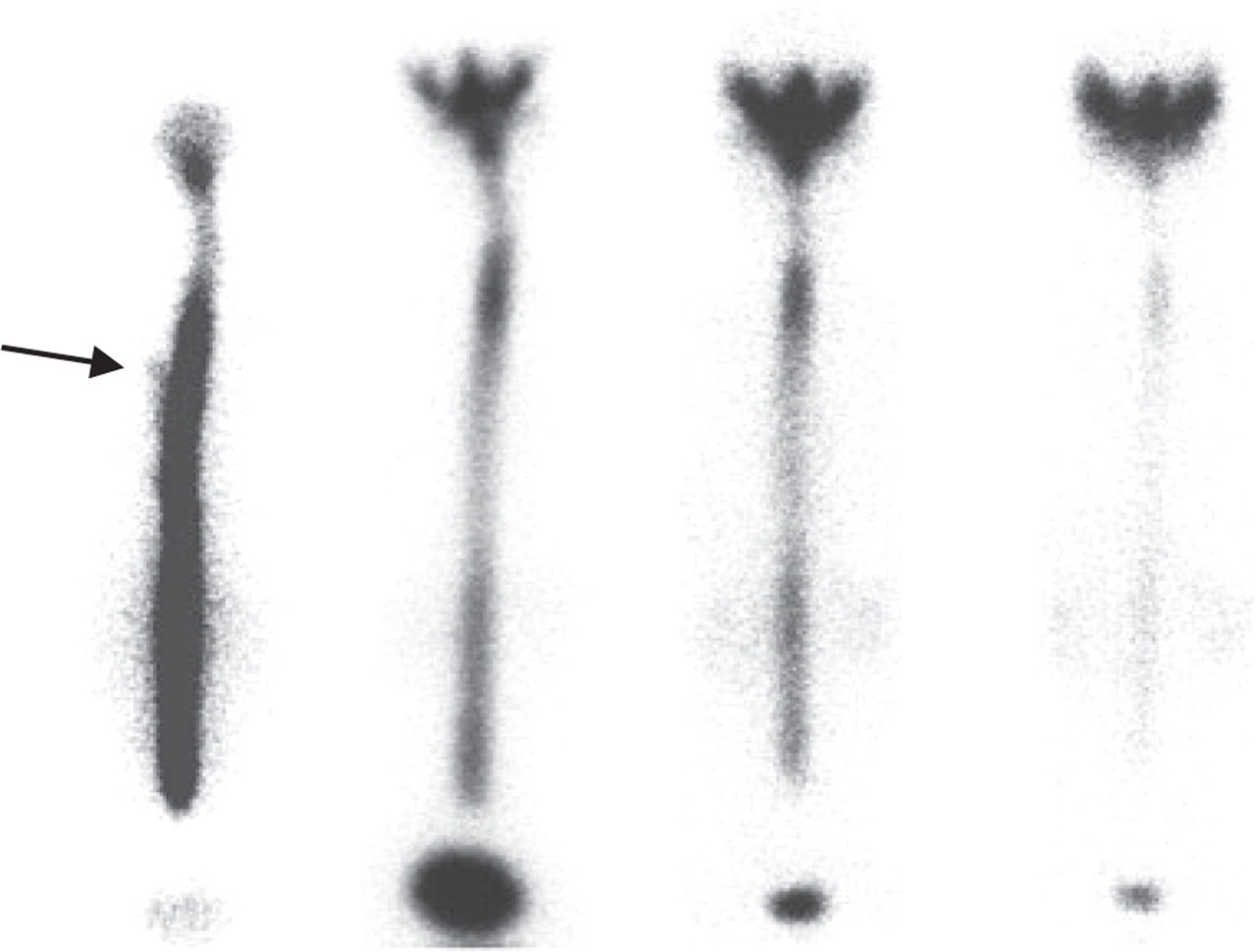
Radioisotope cisternographic images of patient 1 before treatment. The urinary bladder was visualized starting 1 h after injection and was densely delineated at 5 h. Tracer did not reach the high cranial convexity by 24 h. Vague extradural accumulation of tracer is suspected in the right upper thoracic spine (arrow).

Radioisotope cisternographic images of patient 1 obtained 7 months after treatment. Early bladder filling at 1 h, lack of filling into the high cranial convexity at 24 h and extradural accumulation at the right upper thoracic spine were not seen.
Before treatment, RI activity in the CSF space decreased rapidly in patients 1 and 3 and more gradually in patient 2. (Table 1). Residual activity at 24 h was less than 20% of the initial dose in all patients. After treatment, the reduction invariably slowed, remaining at more than 80% of initial dose at 5–7 h and more than 50% at 24 h (Table 1, Fig. 3).

Mean and SD (vertical bar) in radioisotope (RI) activity in the whole CSF space in the three patients before (lower line) and after treatment (upper line). Values of RI activity (ordinate) are a ratio to those at delivery.
Applied case of semiquantitative analysis
A 32-year-old woman driver was involved in a multivehicle road crash 1 year earlier. A few days later, she experienced headache, retro-orbital and neck pain, lumbago and numbness of the left arm and tongue. She also suffered from loss of concentration and memory and was diagnosed with post-traumatic headache and whiplash-associated disorder. Medical treatment and physiotherapy had no effect on the symptoms, but pain was markedly alleviated in a recumbent position. Neurological and radiological evaluation disclosed no objective abnormalities. CSF pressure was 85 mmH2O. RI examination was apparently normal, but revealed vague tracer accumulation in the bladder at 1 h and massive accumulation at 5 h, leading to an equivocal diagnosis of extradural leakage of tracer at the lower lumbar spine (Fig. 4). Additionally, the rapid clearance of tracer similar to that with spontaneous CSF leakage was supportive of the diagnosis (Fig. 5, lower line); EBP was attempted. After two sessions of EBP, her headache resolved completely, but the neck pain and finger numbness remain to the present at 9 months after treatment. RI cisternography at 10 months after the initial treatment revealed normalized CSF kinetics (Fig. 5, upper line). Considering the marked changes in tracer clearance curve before and after treatment and the response of her symptoms to EBP, this exceptional case was considered to have a CSF leakage attributed to the mechanical impact on the pre-existing weak point of the dura.

Radioisotope cisternographic images of a representative case before treatment. The urinary bladder was vaguely visualized starting 1 h after injection and densely so at 5 h. In contrast to patients 1–3, tracer reached the high cranial convexity by 24 h. Extradural accumulation of tracer was equivocal in the left lumbar spine (arrow).

Ratio of radioactivity in the whole CSF space to the initial value is plotted against time, taken before (lower line) and after treatment (upper line). Activity before treatment was 74.9% of initial activity at 5 h and 22.1% at 24 h. Respective values after treatment were 94.5% and 53.3%.
Discussion
All three cases in this study fulfilled the criteria for headache due to spontaneously low CSF pressure as defined by the International Classification of Headache Disorders (13). In patient 3, CSF open pressure was not low at the time of RI cisternography, which was performed after unsuccessful drainage for a recurrent subdural haematoma, suggesting that the low CSF pressure might already have been mitigated by the volume effect of the haematoma. However, it is also well known that several cases with CSF leakage actually show CSF pressure within normal limits (14). From this view point, CSF hypovolaemia is more adequate to present this clinical entity than intracranial hypotension (15, 16).
In this study, although an excessive decrease in tracer from the CSF space was clearly demonstrated in all patients, leakage itself was vaguely delineated in only two. In this regard, several patients with spontaneous CSF leakage in previous studies showed no abnormalities on MRI or conventional RI (4, 5, 17, 18). To improve the sensitivity of RI cisternography in the diagnosis of CSF leakage, we introduced a semiquantitative analysis of tracer clearance to supplement the qualitative assessment. All three patients showed accelerated tracer excretion from the CSF space and residual activity at 24 h was low in all three. To our knowledge, only one report has described RI clearance of the whole CSF space in patients with CSF leakage (1). Moriyama et al. reported that RI clearance in cases with overt leakage on RI showed an exponential pattern. Although the present and these previous results are similar, their cases showing serrate-shaped accumulation of tracer along the spinal axis seemed markedly more severe than ours. In contrast, our patients showed only subtle extradural leakage, which might have been easily overlooked by inexperienced physicians. Against this, clearance curves in our patients were definitely abnormal and the result suggests that this semiquantitative analysis provides higher sensitivity to a mild rate of leakage.
The clearance curves obtained after treatment in these patients with spontaneous CSF leakage appear to imply normal tracer kinetics in RI cisternography, although the involvement of an unrecognized effect of EBP cannot be ruled out. To our knowledge, the normal pharmacokinetics of 111In-DTPA tracer in the whole CSF space has not been reported. In the present study, tracer activity remained at more than 90% at 5 h and more than 50% at 24 h. Timing of repeated examination after treatment might influence the results. Weber et al. reported a case in which RI cisternography showed similar results at 1 week to those at initial study, even though the patient had become symptom free (8). To obtain a normalized cisternographic pattern, we conducted post-treatment RI examination after confirming complete cure at 4–7 months after treatment. This longer duration after treatment may render these findings more reliable than those obtained at shorter intervals.
The slower tracer clearance in patient 2 than in the others may have been due to differences in location of the leak as well as in the rate of leakage itself. When the site of leakage is close to the injection point, clearance may be more rapid, whereas when it is in the upper cervical area or craniocervical junction, it may appear normal in the first few hours. Regardless of differences in the early reduction rate in the present patients, tracer reached <20% after 24 h. From this result, we feel a lower limit of normal range is around 40–50% at 24 h, while a decrease to <20–30% at 24 h, especially with a two-phase pattern, may strongly suggest CSF leakage. Based on our results, we were able to diagnose an additional patient with post-traumatic postural headache as having a CSF leakage and the patient was successfully treated with EBP. Interestingly, the clearance curve of the patient after treatment was the same as those of the three cases with spontaneous CSF leakage.
RI cisternography is theoretically a paradoxical means of evaluating the CSF circulation, since the examination requires a dural puncture. The potential for CSF leakage caused by puncture remains a hindrance in quantitative analysis. We used a 25-G pencil-type needle and kept patients under bed rest for 6–7 h after injection to minimize iatrogenic CSF leakage. As a distinct difference in RI clearance before and after treatment was demonstrated, iatrogenic leakage in this study may have been negligible, but leakage was probably also minimized by the effect of bed rest on CSF circulation. Some authors have emphasized the importance of maintaining an upright position during the examination to promote leakage, notwithstanding that this may produce false-positive leakage from the injection site (19). We do not advocate use of this analysis for all patients with intracranial hypotension syndrome. However, the present findings suggest that quantitative RI assessment as a standardized procedure may be useful in identifying CSF leakage in particular cases with slow-flow leak resulting in apparently normal or equivocal MRI/RI findings. To establish a normal threshold of tracer clearance, further experience with a variety of patients is necessary, since the patient's age may affect the results.