
Abstract
Background:
Radioisotope cisternography (RICG) is useful for detecting cerebrospinal fluid (CSF) leakage in spontaneous intracranial hypotension (SIH) patients. However, RICG can cause iatrogenic CSF leakage (ICSFL) due to a lumbar puncture.
Objectives:
To compare the RICG findings of SIH and ICSFL.
Methods:
The presence of direct findings suggesting CSF leakage and indirect findings including early visualization of the bladder and absence of radioactivity over the brain convexities were evaluated in seven SIH and six ICSFL patients. Radioisotope clearance was assessed semi-quantitatively.
Results:
In contrast to the variety of anatomical levels at which direct findings were detected in the SIH patients, the ICSFL patients only displayed direct findings at the lumbosacral level. None of the ICSFL patients displayed direct findings at 1 hour after the tracer injection. Although early visualization of the bladder was depicted in all patients, no activity was visualized over the brain convexities in the SIH patients. In the semi-quantitative analysis, the tracer retention index at 24 hours was lower in the SIH patients than the ICSFL patients.
Conclusions:
The early appearance of direct findings above the lumbosacral level, the absence of radioactivity over the brain convexities and a low tracer retention index are suggestive of SIH.
Keywords
Introduction
Orthostatic headache is a characteristic symptom of spontaneous intracranial hypotension (SIH) but, recently, various atypical types of headache and associated symptoms as well as the presence of a normal cerebrospinal fluid (CSF) pressure have been reported (1–4). As the spectrum of its clinical manifestations widens, the diagnosis of SIH by imaging findings including subdural fluid collection, enhancement of the pachymeninges, and sagging of the brain, and the demonstration of low CSF pressure are insufficient as is the efficacy of epidural blood patching (5,6); therefore, the demonstration of paraspinal CSF leakage (i.e. the presence of extrathecal CSF) by diagnostic imaging is expected to become very important.
Radioisotope cisternography (RICG), computed tomography myelography, spinal magnetic resonance imaging (MRI) and magnetic resonance myelography (MRM) have been reported to be useful for detecting CSF leakage (7–11). In particular, RICG is considered to be useful because it can evaluate not only the direct signs of leakage but also indirect signs and allows quantitative analysis (12,13). However, RICG carries a risk of iatrogenic CSF leakage (ICSFL), even when the puncture is performed carefully using a fine needle, and ICSFL can mimic SIH, leading to misdiagnosis (14). Since the imaging findings of SIH and ICSFL have rarely been compared (15), the present study attempted to investigate the differences in the RICG findings of SIH and ICSFL patients.
Materials and methods
Subjects
Clinical features of the SIH and ICSFL patients.

SIH: spontaneous intracranial hypotension; ICSFL: iatrogenic cerebrospinal fluid leakage; F: female; M: male;
L: lumbar; S: sacral; N.A.: not applicable.
Radionuclide cisternography
The intrathecal injection of 37 MBq (1 mCi) In-111 diethylenetriamine-penta-acetic acid was performed carefully at the L3/4 or L4/5 level using a 25-gauge (G) pencil point spinal needle (excluding patient no. 13, who was punctured with an 18-G spinal needle). After the injection, all patients took bed rest for 2.5 hours. Whole cerebrospinal axis planar images were obtained at 1.0, 2.5, 6.0 and 24 hours after the injection using a dual-head gamma camera system (E.CAM; Siemens, Erlangen, Germany) equipped with medium-energy low penetration parallel hole collimators at an acquisition time of 6.7 min. The energy window was centered at 172 and 247 keV and opened by ±15%. Images were acquired in a 256 × 1024 matrix. Before the intrathecal injection of the radionuclide, the measurement of CSF pressure and CSF sampling was performed.
Image analysis
Qualitative analysis
In RICG, focal areas of increased radioactivity in the unilateral or bilateral paraspinal regions were defined as a direct abnormal finding that was suggestive of CSF leakage. This finding was graded on a 4-point scale: grade 0, no paraspinal activity; grade 1, possible leakage (faint paraspinal activity involving an area with a diameter that is shorter than the transverse diameter of the area of spinal canal activity); grade 2, probable leakage (strong paraspinal activity involving an area with a diameter that is shorter than the transverse diameter of the area of spinal canal activity); grade 3, definite leakage (strong paraspinal activity involving an area with a diameter that is longer than the transverse diameter of the area of spinal canal activity) (10). The anatomical level at which direct findings appeared and the time at which they were first detected was assessed. Indirect abnormal findings were defined as early visualization of the bladder (radioactivity in the bladder at 1.0 or 2.5 hours after injection) and no visualization of activity over the brain convexities (no marked accumulation around the brain at 24 hours after injection) (12). The RICG images were independently reviewed by a neuroradiologist (K.S.) and a neurosurgeon (M.N.), who were blinded to the patients’ clinical information, and abnormal findings were determined by agreement.
Semi-quantitative analysis
As a semi-quantitative assessment, the degree of radioactivity in the whole CSF space excluding the bladder was assessed on postero–anterior RICG images in order to evaluate radioisotope clearance from the CSF space at 1.0, 2.5, 6.0 and 24 hours after the tracer injection (Figure 1). Due to the square shape of the region of interest, radioactivity in the kidneys and epidural space could not be excluded from the count. After correcting for the radioactive decay of the tracer, the tracer retention index of each scan phase relative to the first scan (1 hour after the injection) was calculated for both the SIH and ICSFL patients.
RICG posteroanterior image of a 44-year-old ICSFL patient (case 9). RICG was performed at 24 hours after the tracer injection and detected abnormal activity in the left paraspinal area. The square indicates the region of interest in which radioactivity was counted.
Statistical analysis
Statistical analyses were carried out using the SPSS 11.0 statistical software program (SPSS Inc., Chicago, IL, USA). The Mann–Whitney U test was used for comparisons of the patients’ age data, the timing of the initial appearance of direct findings, the grade of the direct findings and the tracer retention index. Fisher’s exact test was used for comparisons of the gender distribution between groups. Differences were considered significant when p < 0.05.
Results
There were no significant differences in the mean age or gender distribution between the SIH and ICSFL patients (p = 0.20 and 0.59). The radiological features of the patients are summarized in Table 2. In six of the seven SIH patients, spinal MRI and MRM was performed before RICG; four were found to have a spontaneous leakage at the lumber level and two were not. In one subject (case no. 4), spinal MRI and MRM was performed only after the RICG examination, so it was difficult to determine whether or not the lumbar level leakage on RICG was spontaneous or iatrogenic. However, CSF leakage appeared 2.5 hours after the tracer injection at the cervicothoracic level, but at the lumbosacral level it appeared 6 hours later. The cervicothoracic level finding was considered to be caused by SIH. In contrast to the variety of anatomical levels at which direct findings were observed in the SIH patients (Figures 2, 3), the ICSFL patients only displayed direct findings at the lumbosacral level on RICG (Figure 4). Furthermore, the ICSFL patients revealed a higher grade of lumbosacral direct findings than the SIH patients; the mean direct finding grade (±SD) was 1.6 ± 0.8 in the SIH patients and 2.8 ± 0.4 in the ICSFL patients (p = 0.04). The initial appearance of direct findings occurred earlier in the SIH patients than the ICSFL patients (p = 0.02). None of the ICSFL patients displayed direct findings at 1 hour after the tracer injection.
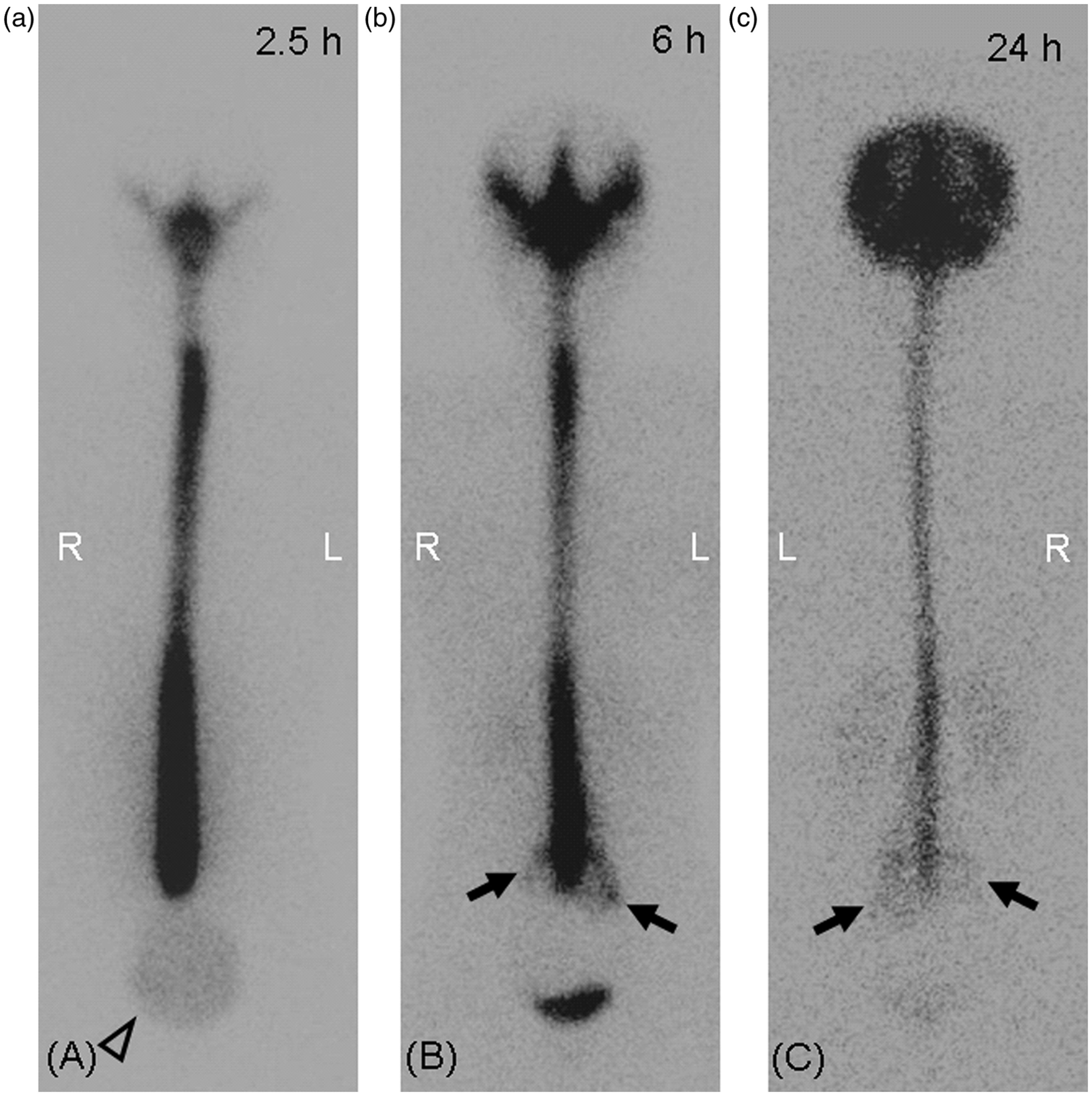
Direct finding of CSF leakage at the thoracic level on serial RICG images taken at 2.5, 6, and 24 hours after the tracer injection in a 55-year-old SIH patient (case 3). Left-dominant abnormal paraspinal activity was seen at the lower thoracic level at 2.5 to 24 hours after the tracer injection ((a)--(c), arrows). Early visualization of the bladder was depicted at 2.5 hours after the tracer injection ((a), open arrowhead). At 24 hours after the injection, an RICG image revealed limited uptake and rapid washout of the intrathecal tracer and the absence of activity over the brain convexities ((c), open arrow). Direct findings were observed at multiple levels on serial RICG images taken at 2.5, 6 and 24 hours after the tracer injection in a 39-year-old SIH patient (case 5). In addition to the abnormal right paraspinal activity observed at the level of the cervicothoracic junction at 2.5 to 24 hours after the tracer injection ((a)--(c), arrows), RICG images revealed a cervical level leak at 2.5 hours and a lumbosacral level leak at 24 hours ((a), small arrow; (c), arrowhead). Similar to the RICG images of case 3, early visualization of the bladder, limited uptake of the tracer and the absence of activity over the brain convexities were depicted ((a), open arrowhead; (c), open arrow). The white arrowheads (a) indicated tracer accumulation along the urethral catheter. Serial RICG images taken at 2.5, 6 and 24 hours after the tracer injection in a 34-year-old ICSFL patient (case 8). RICG images revealed left-dominant abnormal paraspinal activity at the lumbosacral level at 6 to 24 hours after the tracer injection ((b) and (c), arrows). In addition to the direct findings, early visualization of the bladder was depicted at 2.5 hours after the tracer injection ((a), open arrowheads). Radiological features of the SIH and ICSFL patients. SIH: spontaneous intracranial hypotension; ICSFL: iatrogenic cerebrospinal fluid leakage; h: hour(s); EVB: early visualization of the bladder; NVA: no visualization of activity over the brain convexities; C: cervical; Ct cervicothoracic; T: thoracic; L: lumbosacral; N.A.: not applicable. *Radioisotope cisternography showed a small area of epidural accumulation on the caudal side of the dural sac at 6 hours after the tracer injection, but this finding was not categorized as cerebrospinal fluid leakage.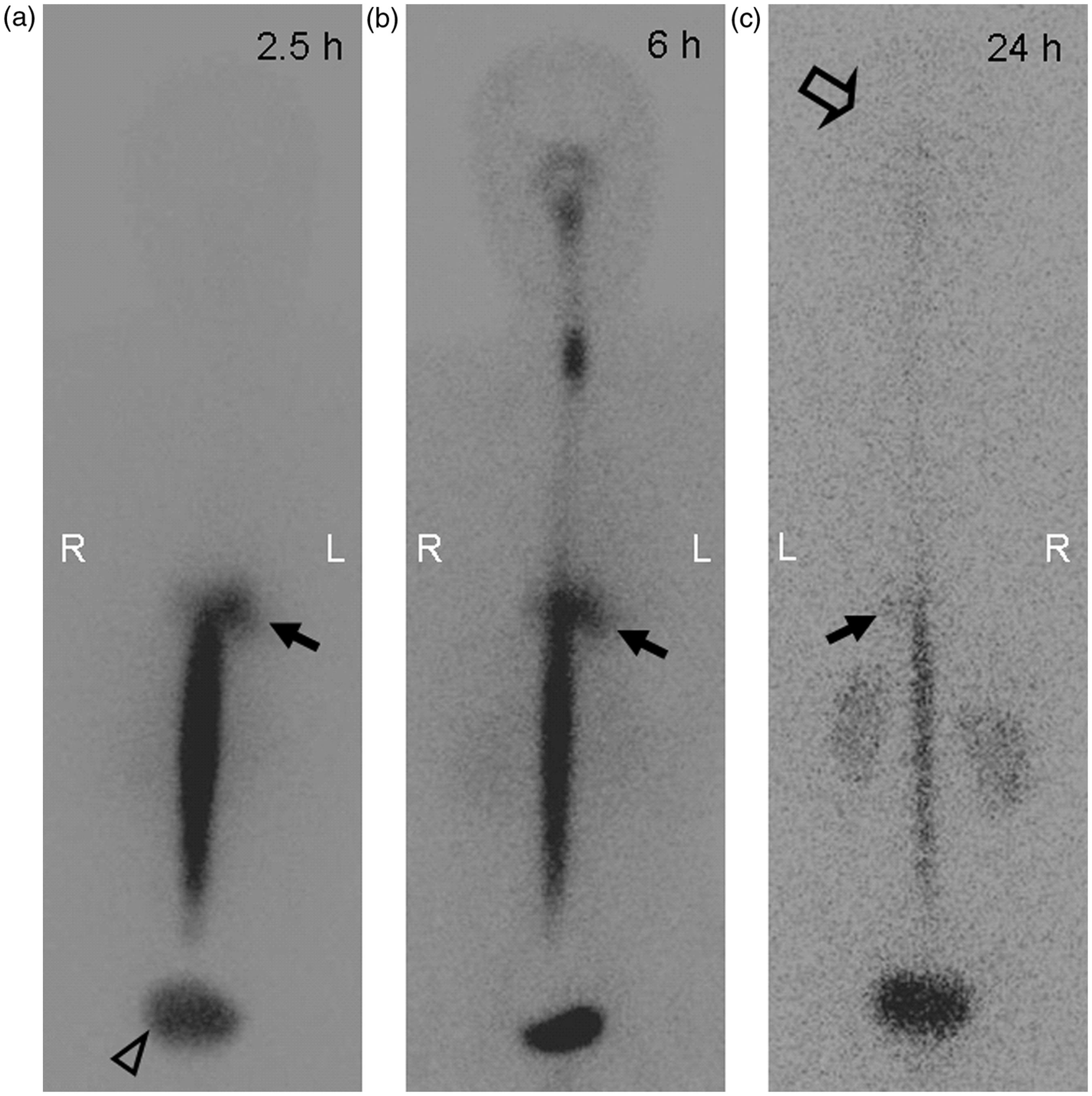


During the evaluation of indirect findings, early visualization of the bladder was depicted in all patients (Figures 2–4). Contrary to other findings, the absence of activity over the brain convexities was exclusively detected in the SIH patients (Figures 2, 3). The tracer retention index data obtained in the semi-quantitative analysis are shown in a boxplot (Figure 5). The SIH patients displayed a lower mean tracer retention index than the ICSFL patients at 24 hours after the tracer injection (p = 0.03). Notably, the tracer retention index of one of the ICSFL patients (case 13) was relatively high, despite them being punctured with an 18-G spinal needle (18% at 24 hours).
Boxplots of the tracer retention index for RICG in the SIH and ICSFL patients. At 2.5 and 6 hours after the tracer injection, there was no significant difference between the SIH (0.86 ± 0.13 [SD], 0.47 ± 0.23) and ICSFL patients (0.92 ± 0.07, 0.56 ± 0.11) (p = 0.72 and 0.77, respectively). However, at 24 hours after the injection, the tracer retention index of the SIH patients (0.09 ± 0.05) was lower than that of the ICSFL patients (0.22 ± 0.09) (p = 0.03).
Discussion
Although the most common sites of CSF leakage in spinal CSF leak syndrome have been reported to be the cervicothoracic junction and the thoracic area (17), multiple simultaneous spinal CSF leaks were detected at the initial presentation in some of the patients reported in the literature, as well as some of the patients in this study (7,10). On the other hand, lumbosacral dominant leakages have also been reported (13,18). As lumbar puncture carries a risk of CSF leakage, it is necessary to carefully evaluate not only the presence of direct findings but also other imaging findings that are suggestive of CSF leakage.
It is not surprising that the ICSFL patients only displayed direct findings at the lumbosacral level because the thecal punctures were performed at this location. Direct findings appeared later in the ICSFL patients than the SIH patients (at 6 hours after the tracer injection in three of the five cases and at 2.5 hours in two cases). Notably, none of the ICSFL patients displayed direct findings at 1 hour after the tracer injection. Taking the 2.5 hours’ bed rest enjoyed by the subjects into account, it is plausible to assume that body movements including upright positioning after bed rest can worsen CSF leakage through post-puncture dural tears and, hence, cause the late appearance of direct findings.
Indirect findings as well as direct findings of CSF leakage have been utilized for the diagnosis of SIH, especially in cases in which RICG fails to demonstrate direct findings (12,19). However, the utility of indirect findings is disputed. For example, early visualization of the bladder has been reported in both SIH and ICSFL patients (14,20,21). This suggests that tracer leakage through dural defects, even those caused by the small sized 25-G pencil point spinal needle, could migrate into the extrathecal space and produce imaging findings similar to those of SIH.
Although semi-quantitative evaluations of RICG images have also been performed for the diagnosis of SIH (13,22,23), no study has compared the results of these evaluations between SIH and ICSFL. In this study, the SIH patients displayed a lower mean tracer retention index at 24 hours than the ICSFL patients. As well as the absence of activity over the brain convexities in the SIH patients, this finding indicates the unusual diffusion of tracer into the extra-arachnoid space and its rapid uptake by the circulation. As reported previously (9), the precise cause of spontaneous CSF leakage was not clarified in this study. However, considering the presumed underlying structural weakness of the spinal meninges due to small dural tears and the complex and fragile nature of the meningeal diverticula (17), it is plausible to assume that these structural abnormalities could cause more intense temporal tracer leakage than iatrogenic post-puncture dural tears caused by fine spinal needles.
The RICG findings, including the presence of CSF leakage outside the lumbosacral levels, the absence of radioactivity over the brain convexities and the chronological changes, should be useful to diagnose SIH, irrespective of the CSF leakage findings at the lumbosacral levels. Considering the similarities of the direct findings at the lumbosacral levels between ICSFL and SIH, it appears important to evaluate these findings on RICG. Another advantage is that these findings can be evaluated through usual examination and any special analysis software or MRI is not required.
The small number of subjects, especially SIH patients with CSF leakages localized to the lumbosacral levels, is the main limitation of this study. This would not affect our results regarding the timing of the initial appearance of direct findings of CSF leakage because the SIH patients displayed an earlier initial appearance time despite the distal location of their puncture sites. However, the small number of subjects might have affected the diagnostic value of the semi-quantitative evaluation of the tracer retention index. Thus, it is necessary to compare the findings of SIH patients with localized lumbosacral-level CSF leaks with those of ICSFL patients in order to further analyze the severity and distribution of direct findings of CSF leakage at the lumbosacral level. Another limitation is that healthy normal controls were not recruited for ICSFL subjects. There are two reasons why we used symptomatic subjects for the comparison of ICSFL and SIH. One is that RICG is a costly and invasive examination, which could cause various complications, including not only ICSFL but also infectious meningitis, intracranial, spinal hematoma and so on (24–26). Another is related to the clinical indication of RICG. Generally, RICG is performed to evaluate symptomatic subjects with a suspicion of CSF leakage and hydrocephalus. Therefore, it is highly unusual to perform this examination in asymptomatic subjects. Thus, we think that evaluating symptomatic subjects is more reasonable in the clinical situation than evaluating healthy subjects. Since abnormal imaging findings appeared only after the intrathecal injections of the radioisotope, lumbar punctures were considered to be the primary cause of the CSF leakages in ICSFL patients (even if a small amount of image-negative spontaneous CSF leakage might exist). Finally, our results regarding the direct findings and tracer retention index in ICSFL patients should not be applied to all kinds of ICSFLs because needle sizes and anatomical levels for thecal punctures could affect the results.
In conclusion, additional imaging findings that are related to chronological changes would be useful for distinguishing post-puncture ICSFLs from SIH. Lumbosacral dominant CSF leakage and early visualization of the bladder should be carefully interpreted because CSF leakage, even that caused by the use of fine spinal needles, can cause these findings.
Footnotes
Funding
This research received no specific grant from any funding agency in the public, commercial or not-for-profit sectors.
Conflict of Interest
None declared.