
Abstract
Information is sparse concerning the incidence and prognosis of headache in children from the general population, especially of tension-type headache. In this study, headache diagnoses and symptoms were reassessed in 122 out of 130 schoolchildren after 3 years. Nearly 80± of those with headache at first evaluation still reported headache at follow-up. Although the likelihood of experiencing the same headache diagnosis and symptoms was high, about one-fifth of children with tension-type headache developed migraine and vice versa. Female gender predicted migraine and frequent headache episodes predicted overall headache at follow-up. The estimated average annual incidence was 81 and 65 per 1000 children, for tension-type headache and migraine, respectively. We conclude that there is a considerable risk of developing and maintaining headache during childhood. Headache diagnoses should be reassessed regularly and treatment adjusted. Girls and children with frequent headache have a poorer prognosis and therefore intervention is particularly important in these groups.
Introduction
Headache is the most frequently reported pain in children (1–5), and is associated with missed schooldays, anxiety, depressive symptoms and other pains and physical symptoms (6, 7). Although headache usually has its onset during childhood and adolescence, knowledge of the incidence and prognosis is limited, especially for tension-type headache (TTH). The prognosis of migraine in children has been investigated primarily in clinic-based (8–14) but less often in population-based samples (15–20). To our knowledge, only three studies have described the outcome of TTH (12–14), none of them in a sample from the general population. Samples from tertiary clinics are more likely to include children with severe and recurrent headache (21) and their prognosis of headache is probably different from children in the general population because few children of the general population contact healthcare because of their headache (22).
The most extended longitudinal study was performed by Bille, who showed that more than half of schoolchildren with pronounced migraine still had migraine after 40 years (15). In recent longitudinal studies using the criteria of the International Headache Society (IHS) (23), a considerable proportion of children changed their headache diagnosis or became free from headache after a few years (12–14, 18, 20).
Information is sparse about factors influencing the prognosis of headache in children (13, 16, 18, 19). For TTH only one study exists on a sample from different headache clinics, reporting girls to become free from TTH less often than boys (13). Even less is known about the extent to which different headache symptoms persist within individuals over time. The only previous report found no correlation between initial headache intensity and that at follow-up 10 years later (12).
Increased knowledge about the natural history of headache and prognostic factors is important to identify children at risk of chronic headache and to evaluate the need and effect of treatment. Cross-sectional prevalence studies show a gradual increase of headache during childhood but, unlike longitudinal studies, they do not reveal the extent of remissions and relapses of headache.
Since there is little information about the incidence and prognosis of headache in children from the general population, especially for TTH, the objectives of this study in a sample of schoolchildren aged 7–15 years were as follows:
Describe the outcome of migraine, TTH, overall headache and headache symptoms after 3 years.
Determine whether age, sex, heredity for migraine, frequency, intensity and duration of headache can predict the outcome of migraine, TTH and overall headache.
Estimate the incidence of migraine, TTH and overall headache.
Methods
Study population
From a sample of 1371 schoolchildren aged 7–15 years who participated in a questionnaire study (24) in 1997 (T1), a random sample of 131 children, stratified according to age, gender and preliminary headache diagnosis, were interviewed together with a parent. After excluding one child with secondary headache diagnosed at the interview, the final sample consisted of 130 children. In 2000 (T2), the 130 children from the interview study were contacted by letter and asked to complete a second identical questionnaire about their headache symptoms during the preceding year. After one reminder a total of 122 children (94%), 64 girls and 58 boys, responded. At T1 they were aged 7–15 years (mean 11.2, SD 2.6). Of the eight children (six girls, two boys) who did not respond, one had a secret address and one declined participation, whereas the other six gave no specific reason. The mean age of the non-responders did not differ significantly from that of the responders.
The studied sample of 122 children was representative of the original sample of 1371 schoolchildren in age and sex distribution but, due to the stratification, differed according to headache diagnoses (Table 1).
Distribution of headache diagnoses in the total questionnaire sample and the present sample in 1997 and weight of each stratum
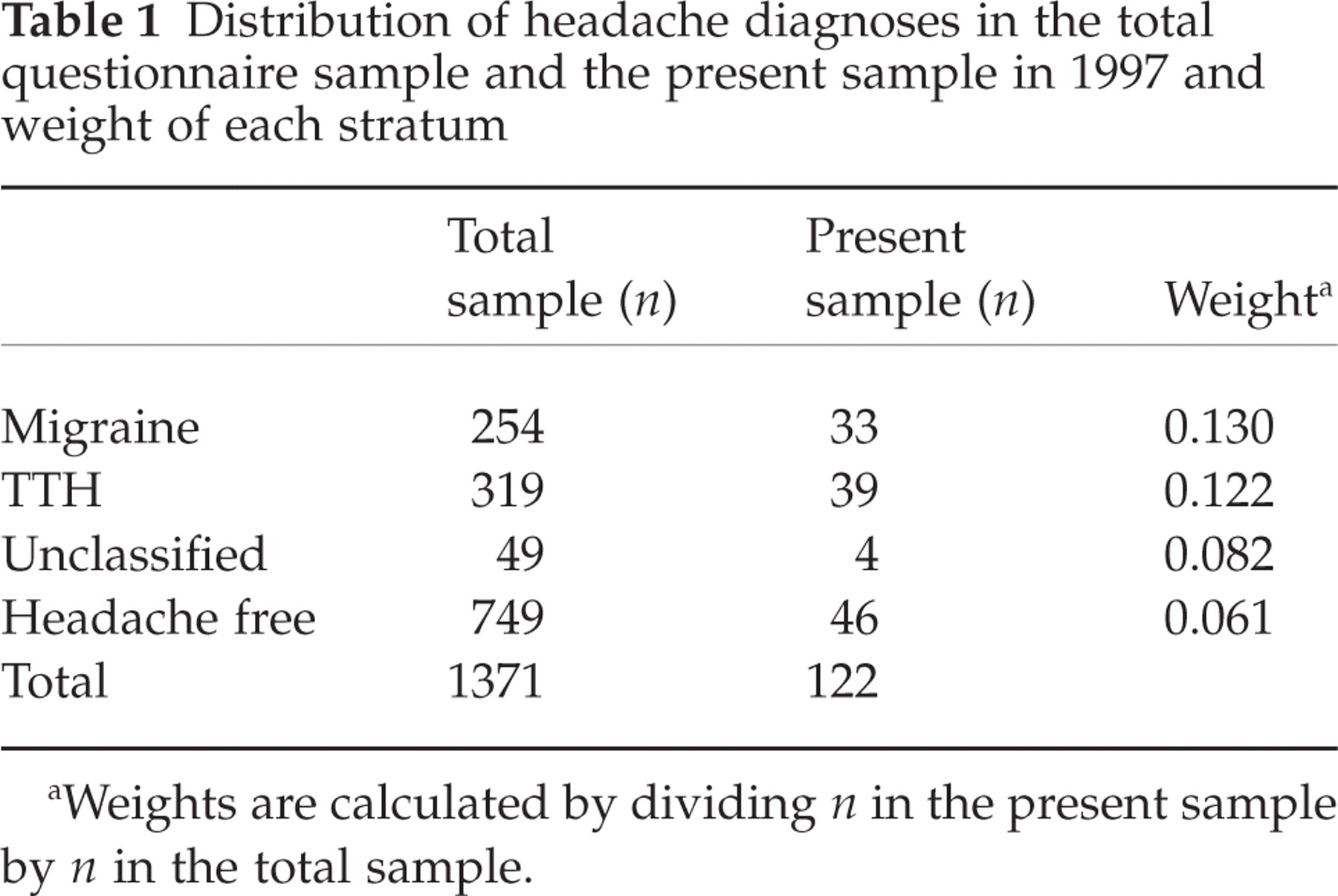
Weights are calculated by dividing n in the present sample by n in the total sample.
The ethics committee of Uppsala University approved the study and the children and their parents gave their informed consent to participate.
Diagnoses
At T1, 76 children had primary headache (i.e. headache not associated with infection or other disease) and 46 had no primary headache (in the following called headache free) according to the questionnaires. The IHS criteria 1988 (23) were used to classify the different headache types. However, children fulfilling all but one criterion for migraine (IHS 1.7) and TTH (IHS 2.3) were included in the migraine (n = 33) and TTH (n = 39) groups, respectively. Four children had unclassifiable headache. Of those with IHS 1.7 (n = 17), one (5.9%) did not fulfil criterion A (minimum number of earlier headache episodes), 15 (88.2%) did not fulfil criterion B (minimum duration of headache) and one (5.9%) did not fulfil criterion C or D (based on headache symptoms). The corresponding figures for IHS 2.3 (n = 13), were seven (53.9%), three (23.1%) and three (23.1%), respectively. We also included six children who fulfilled neither criterion A nor criterion B into the migraine and TTH group. This was because we previously, in the same sample, found better agreement between interview and questionnaire diagnoses and fewer unclassified headaches without criterion B (25), and because criterion A, requiring at least five previous episodes for migraine and 10 for TTH, is impractical when estimating new headache cases in children.
Headache symptoms
In children with headache, symptoms reported in the questionnaire at T1 (i.e. vomiting, quality of headache, visual aura, unilateral headache, photophobia, phonophobia, aggravation by physical activity, frequency, intensity and duration of headache) were compared with those reported in the questionnaire at T2.
Statistical methods
Predictors of headache at follow-up were analysed with logistic regression. Headache, migraine and TTH at T1 were included as covariates when analysing whether age, sex, heredity for migraine, frequency, intensity and duration of headache could predict headache, migraine and TTH at T2. Logistic regression analyses were also used to estimate the likelihood for persisting headache symptoms at T2. The level of significance was set to P < 0.05.
To estimate the cumulative incidence of headache, migraine and TTH, we used weighted calculations to correct for the different distribution of headache diagnoses in the present sample and the original sample of 1371 children. The weight of each stratum was calculated by dividing the number of children with migraine, TTH, unclassified headache and headache free among the 122 children at T1 by the number of children with respective diagnosis in the total sample at T1 (Table 1). Cumulative incidence was calculated by dividing the number of new cases deriving from other headache diagnoses and from the previously headache free with the population at risk (children without the studied diagnosis at T1). The population at risk was n = 1117 for migraine, n = 1052 for TTH and n = 749 for headache-free children. To achieve an annual average rate of cumulative incidence (in the following called annual incidence) we divided by three.
Results
Diagnoses
The number of children with headache at T1 (n = 76) was similar to that at T2 (n = 78). Sixty (78.9%) children reported headache on both occasions. The outcome of migraine, TTH and headache free is shown in Fig. 1 and the gender distribution for the different diagnoses in Fig. 2.
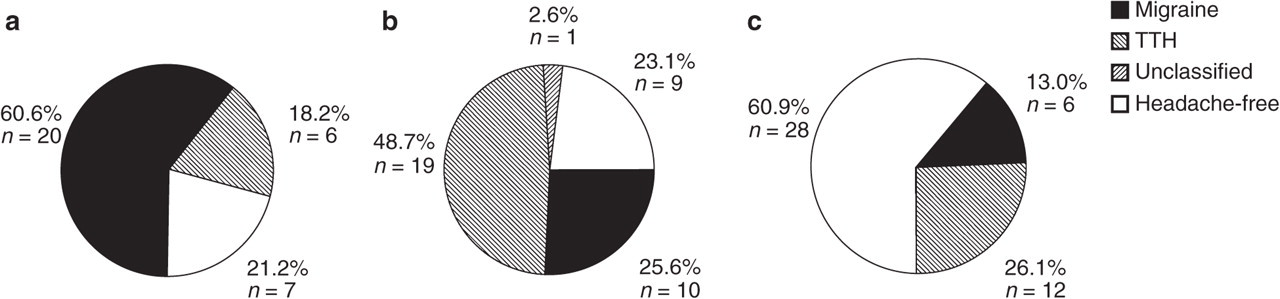
Outcome of migraine, tension-type headache (TTH) and headache free at the 3-year follow-up. Note that the circles represent all children with respective diagnoses at T1. (a)Migraine (n = 33). (b) TTH (n = 39). (c) Headache free (n = 46).
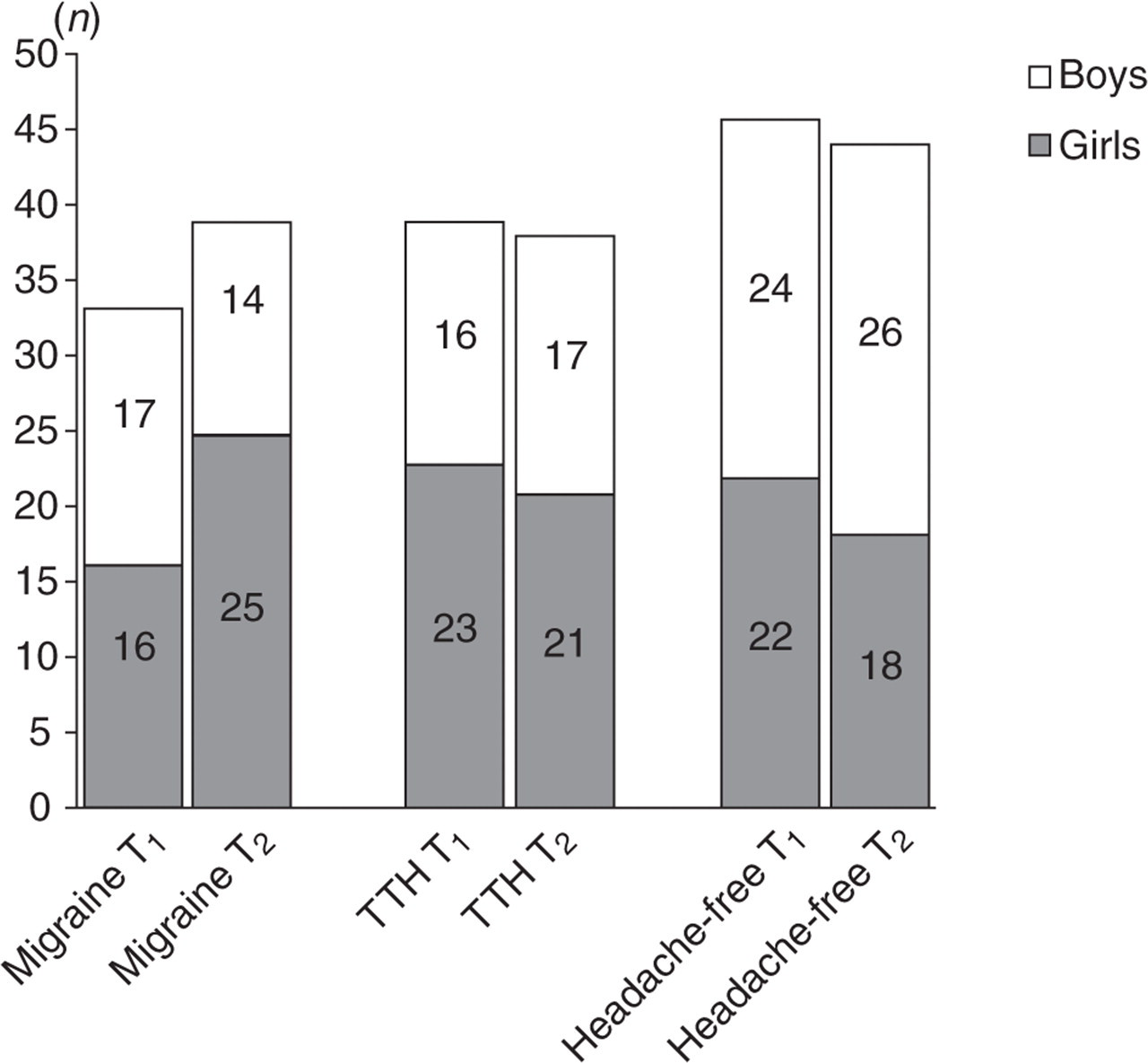
Gender distribution and total number of children in relation to headache diagnoses at T1 and T2.
Prognostic factors
The results of logistic regression analyses showed that headache at T1 predicted headache at T2 [odds ratio (OR) = 5.8, confidence interval (CI) 2.6, 13.2, P < 0.001]. Similarly, migraine at T1 predicted migraine at T2 (OR = 5.7, CI 2.4, 13.5, P < 0.001) and TTH at T1 predicted TTH at T2 (OR = 3.2, CI 1.4, 7.2, P < 0.01). Frequent headache at T1 predicted the occurrence of headache at T2 (OR = 3.2, CI 1.2, 8.3, P < 0.05), female sex predicted migraine at T2 (OR = 2.5, CI 1.1, 6.1, P < 0.05), whereas none of the included variables significantly predicted the outcome of TTH.
Headache symptoms
Among those reporting headache at T1, the risk of experiencing the same headache symptom at T2 was considerable, with ORs ranging from 2 to 25 (Table 2). ‘Headache at least once a week’ and ‘vomiting’ persisted to the highest extent at follow-up (80.0% and 66.7%) and few children with these symptoms became headache free (6.7% and 0%). Among the headache-free children at T1 who developed headache at T2, the most common symptoms were headache less than 2 h and pulsating quality (Table 2).
Outcome of headache symptoms among children with headache at T1 (A) and new headache symptoms among previously headache-free children (B)
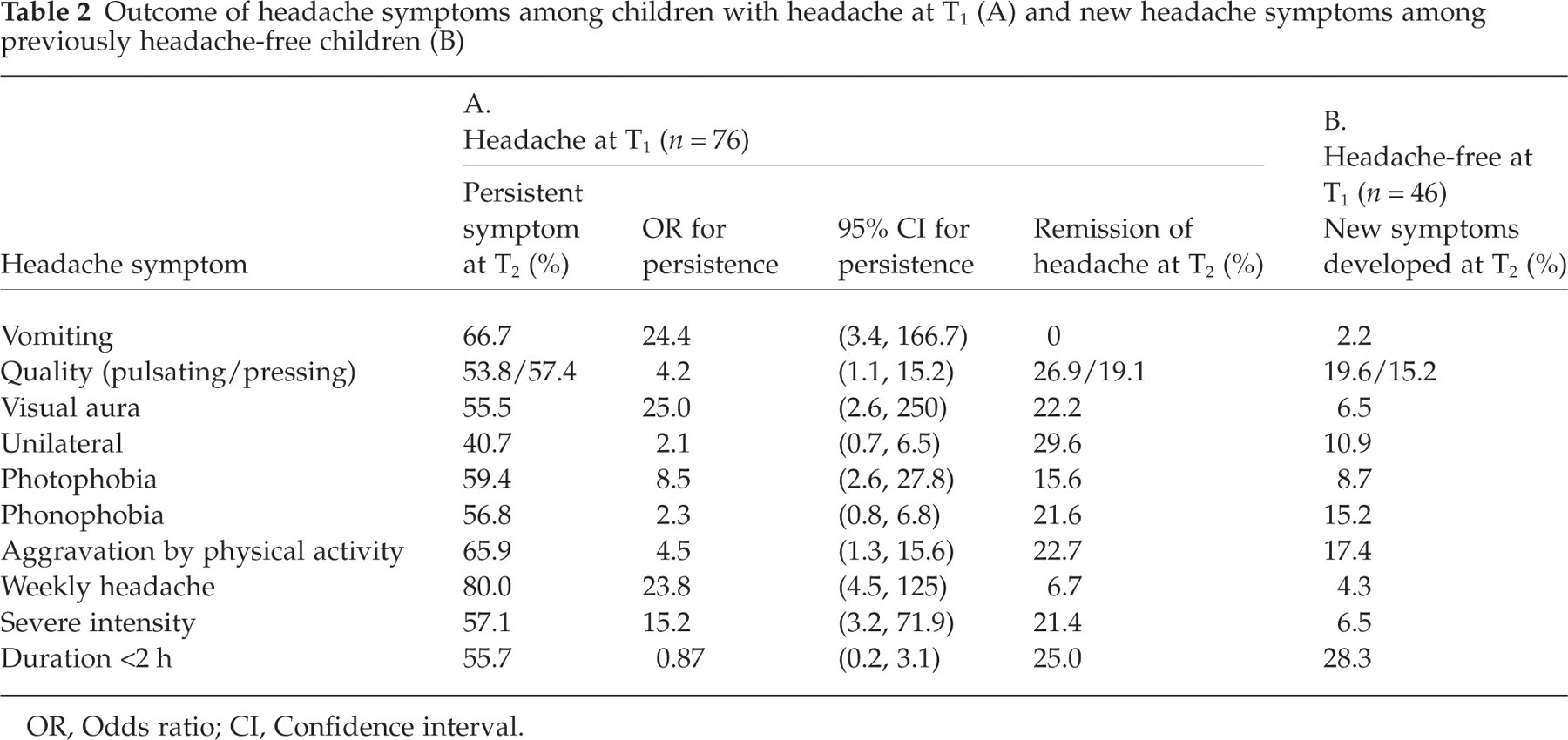
OR, Odds ratio; CI, Confidence interval.
Incidence
A total of 19 new migraine cases at the 3-year follow-up were derived from children with previous TTH (n = 10), unclassified headache (n = 3) and headache-free children (n = 6). The number of new cases with TTH at T2 was also 19, deriving from migraine (n = 6), unclassified headache (n = 1) and headache-free children (n = 12). The number of new headache cases in the headache-free group was 18. To estimate the number of new cases at T2 in the original sample of 1371 schoolchildren, we used weighted calculations as described in Statistical methods. Thus, the calculated number of new migraine cases in the original sample was 217, of which 82.0 (10/0.122) were from those with TTH, 36.6 (3/0.082) from those with unclassified headache and 98.4 (6/0.061) from the previous headache-free group. The number of calculated new TTH cases in the total sample was 255, deriving from the migraine (n = 46.2), unclassified (n = 12.2) and the headache-free (n = 196.7) groups. The number of new headache cases was calculated to be 295 (18/0.061). Thus, the estimated annual incidence of migraine was 65 per 1000 children and for TTH 81 per 1000 children. The annual incidence of overall headache was 131 per 1000 children. The sum of the annual incidence rates for migraine and TTH was larger than the incidence for overall headache because the populations at risk were different.
Discussion
In this sample of schoolchildren, nearly 80% of those with headache at first evaluation still reported headache 3 years later and nearly 40% of the headache free had developed headache. Although the likelihood of still experiencing the same headache diagnosis and symptoms at follow-up was high, about one-fifth of children with migraine developed TTH and vice versa. In logistic regression analyses, female gender predicted migraine at follow-up and frequent headache predicted the occurrence of headache at follow-up.
Most previous longitudinal studies in children have focused on migraine. To our knowledge, this is the first study describing the outcome of TTH in a sample of children from the general population.
Unexpectedly, children with TTH became headache free less often (23%) and developed migraine more often (26%) compared with children at tertiary clinics, where 33–50% became headache free and 8–12% changed into migraine at follow-up (12–14). One explanation is that treatment received in these clinic-based samples may have influenced the outcome positively. For example, Dooley and Bagnell (12) reported that a majority of their patients had received treatment, most commonly non-prescribed drugs and relaxation. Another explanation for the better outcome in two of the studies is the longer follow-up time of 10 and 8 years, respectively (12, 13). Mazzotta et al. (14) found that 33% of the children with TTH had become headache free at follow-up after 3 years, a figure closer to our result. The follow-up time, sex and age distribution were similar to our study but the response rate (54%) was substantially lower than our own (94%).
The outcome of migraine with 21% headache free and 18% changing into TTH was similar to most recent clinic-based and population-based studies (12–14, 17, 20) in which the corresponding figures were 17–28% and 13–26%, respectively. However, in a study of 8–9-year-old children from the general population, Metsähonkala et al. (18) found a worse outcome of migraine with only 5% headache free and 8% transformed into TTH after 3 years. In publications from the 1980s and earlier, the prognosis of migraine seemed more favourable with 22–48% free from headache at follow-up (8–11, 16, 19).
The high rates of transition between migraine and TTH found in this and previous studies suggest that these diagnoses are related or, as previously proposed, extremes of the same disease spectrum (26). Another explanation may be co-occurring TTH and migraine and difficulties separating these two headache types. However, this is less likely in the present sample since none of the children who changed headache diagnosis at follow-up obtained two different diagnoses at a previous interview (25).
Our findings that female gender predicted migraine and frequent headache predicted the occurrence of headache at follow-up are in line with findings by Bille, who reported that girls (27) and those with high frequency of attacks (19) had a poorer outcome of migraine. Only a few other studies have described the prognosis separately for boys and girls, mostly with a more favourable prognosis for boys (13, 16, 28). However, in one study the outcome was better for girls (18).
We also found that frequent headache (at least once a week) was the most persistent headache feature. A higher frequency and intensity of headache has been associated with lower quality of life in adolescents (29) and in a previous study we found that frequency of headache correlated significantly with other pain and physical symptoms as well as visiting healthcare because of headache (7). Thus, effective interventions in children with frequent headache are particularly important because of the associations with a poor prognosis as well as an increased impairment.
There are few prospective studies estimating incidence rates of headache. Our result of an overall annual incidence of headache (131/1000) was higher than the incidence of troublesome and frequent headache (at least once a week) among 12–14-year-old children (65/1000) (30), but lower than that reported for children at school entry (292/1000) (31). Anttila et al. (31) suggested that the stressful event of starting school contributed to a high incidence of headache. Their finding is in accordance with the considerably higher prevalence rates of headache reported for children aged 7 years than for preschool children (32–35). The lower incidence rates reported for children aged 12–14 years may be explained by the inclusion of severe cases only (30).
Existing information about the incidence of migraine is limited. The incidence of migraine without aura based on retrospective data of onset age was estimated to peak in males at the age of 10–11 years (10.1/1000) and in females at the age of 14–17 years (18.9/1000) (36). Although the authors made mathematical corrections for recall bias, retrospective incidence data are less reliable. Bille revealed such recall bias for age at onset (19) and aura symptoms (15).
At 6-year follow-up of schoolchildren aged 7–15 years, Bille found that among 73 headache-free controls, one girl had developed migraine and four girls had developed frequent non-migrainous headache (19). In addition, seven out of 59 children with frequent non-migrainous headache had developed migraine. For the total group of 132 children, this would correspond to an average annual incidence of about 10/1000 for migraine. Our estimate of incidence for migraine was considerably higher, probably because we also included children with infrequent headache. The incidence of headache may also have changed over a longer period of time. In Uppsala, significantly more schoolchildren reported no headache in 1955 (41%) compared with 1997 (16%) (24).
To our knowledge, there is no previous study with incidence data for TTH. We found a slightly higher incidence of TTH (81/1000) compared with migraine (65/1000), which is in accordance with TTH being less prevalent than migraine among young children but considerably more frequent in adults. The incidence of TTH probably increases over a longer period and peaks later in life than migraine.
The strengths of this study are the inclusion of children from the general population, the use of identical questionnaires on both test occasions and the low drop-out rate. In a previous study we found good agreement between questionnaires and interviews for headache diagnoses and symptoms when compared within a few days (25), suggesting that changes obtained in this study were time related and not due to unreliable methods. The possibility of generalizing the incidence rates back to the original population of schoolchildren was increased by the mathematical corrections for the different distribution of headache diagnosis in the present sample. The high rates of transition between headache diagnoses in this and previous studies emphasize the importance of including not just a headache-free group but also cases with other headache diagnoses, when estimating the incidence of migraine or TTH.
Some limitations of the present study need to be considered. Since the study was performed in 1997 and 2000, the IHS classification from 1988 was used (23). In 2004, the IHS criteria for migraine were revised for children by lowering of the minimum duration criterion from 2 to 1 h and accepting bilateral headache (37). In the present study, 12 out of 17 children with IHS 1.7 reported headache lasting between 30 min and 2 h, and are thus likely to fulfil the revised IHS criteria for migraine. This supports our decision to merge IHS 1.7 into the migraine group.
The estimates of incidence were based on a limited number of children and on a period of 3 years, instead of measurements each year. It is probable that the annual incidence rates differed during this time because the children in the sample became older.
In future research, it would be valuable to estimate incidence annually as well as describe the prognosis of migraine and TTH in large cohorts from the general population.
Conclusion
There is a considerable risk of developing and maintaining headache during childhood. Headache diagnoses should be reassessed regularly and treatment adjusted. Girls with migraine and children with frequent headache have a poorer prognosis and therefore treatment is particularly important in these groups.
Acknowledgements
We thank Jesper Sperber for his assistance with data collection. This study was supported by grants from Uppsala County Council, Uppsala University, Swedish Migraine Society, and the foundations of Gillberg and Selander.