
Abstract
This study explored the association between headache response and return to functioning, and identified migraine-associated symptoms related to functional status and acceptability of migraine treatment as reported by patients. Data from migraineurs enrolled in the active arms of a randomized, double-blind, parallel group, placebo-controlled, clinical trial were analysed. The relationships between headache response and functional response, and clinical factors and treatment acceptability were assessed using X 2 tests of proportions and logistic regressions. A greater proportion of patients with headache response at 0.5 h were functioning at 0.5, 1 and 2 h compared with patients who did not attain a headache response at 0.5 h (P < 0.0001). These patients also were more likely to find their treatment acceptable (P < 0.05). The results suggest a direct temporal relationship among the key determinants of migraine resolution. Rapid headache response is associated with faster return to functioning; rapid headache and functional responses are significant attributes of treatment acceptability.
Introduction
Migraine is a disabling and prevalent recurrent pain syndrome in which the impact of the condition and associated disability extend beyond simple pain, resulting in disruption of several physiological processes (1, 2). The array of negative symptoms associated with migraine places it among the world's most disabling medical illnesses (3). In 1989, the American Migraine Study estimated that 23 million people in the USA suffer from migraine (4); subsequent studies have shown that the prevalence of migraine is highest among the middle-age population and in women (5).
Optimal management of migraine includes proper diagnosis, appropriate pharmacotherapy and patient adherence to medication. Although efficient medication is available, migraine patients worldwide are still receiving inadequate treatment (6). Currently, migraine pharmacotherapy includes prophylactic, abortive and symptomatic treatment options (7).
Therapy for migraine should be patient specific, and is considered optimal when functioning is restored (8). Migraine, and the disabling loss of function associated with migraine, have a substantial impact on society, resulting in decreased productivity, missed workdays and disruption of family life (9).
Loss of functioning associated with migraine headache is the result of the actual headache, as well as migraine-associated symptoms such as nausea, vomiting, photophobia and phonophobia (10). A majority of migraineurs cannot concentrate or perform daily activities when migraine pain or associated symptoms are moderate to severe (11, 12). Stronks and colleagues quantified the loss of functioning associated with migraine. Migraine patients showed a greater degree of sleepiness and a lower level of vitality compared with the control group (13). This lower level of functioning leads to a decrease in productivity among migraineurs (13). Productivity in daily activities is significantly diminished in migraineurs (14).
While the onset of a migraine may lead a patient to miss work, there is evidence to show that individuals often do attend work during their migraine attacks (15). However, while at work they experience a decrease in productivity, resulting in what is commonly referred to as presenteeism or on-the-job productivity loss. In a multinational migraine study which evaluated the economic burden of the disease, migraineurs reported only 46% effectiveness while at work with migraine symptoms (16). A considerable economic impact is observed in migraine patients who become disabled during the most productive years of life (17).
Work loss is a major contributor to the economic burden resulting from migraine (9). The amount of work loss due to migraine has been found to be similar across Europe, Latin America and North America (16). In the USA, the annual work loss associated with headache is 3.2 workdays for migraine sufferers (18). Ninety-three per cent of the total cost of migraine is attributable to the indirect costs associated with work loss (17, 19). Gerth and colleagues estimated the economic impact of migraine to their company at approximately 23.8 million dollars, based on year 2000 data (17).
For individuals who work outside the home, it is possible to quantify the economic hardship caused by migraine through an estimation of the loss of income. It is more difficult to estimate migraine-associated economic losses for those who are primarily homemakers (20). Along with decreased productivity, and missed workdays, the burden of migraine also impacts family and social activities. Migraineurs reported more missed days from family and leisure activities than from missed days at work. In a 3-month period, there were on average 4.2 missed days of family and leisure time vs. 2.4 missed days from work/school (21).
Lipton and colleagues found that many partners of migraine sufferers reported decreased work performance, and dissatisfaction with work and responsibilities compared with non-migraineurs (9). In addition, a negative parent-to-child relationship among migraineurs was associated with an increased amount of missed school days by their children. Fagan suggests that migraine may be associated with dysfunctional mother-to-child parenting patterns. In a study of mothers with migraine, migraine-related disability was correlated with inappropriate expectations for children to assume parenting responsibility (22). Overall, impaired family relationships and social activities are reported by approximately 50% of all migraine patients (23). Compared with the general public, the loss of functioning resulting from migraine represents a significant burden to patients, their families and society (24).
In terms of desirable attributes of therapy, prior research indicates that migraineurs look for medications with consistent and rapid onset of action along with relief of pain (8). Silberstein conducted telephone surveys of 500 self-reported migraineurs who reported moderate or severe pain. Patients rated ‘quick headache relief’ as one of the most important factors. Other elements that patients considered important were ‘does not cause nausea’, ‘decreases sensitivity to light’, ‘decreases visual problems’, ‘decreased vomiting’, ‘does not cause drowsiness’, ‘orally administered’, and ‘decreases likelihood of recurrence’ (25). Lipton and Stewart found that the most important features of patient satisfaction from medication included complete relief of headache (87%), rapid onset of pain relief (83%), relief of associated symptoms (76%), no adverse effects (79%), and route of administration (56%). The most common reason for dissatisfaction with treatment was ‘when pain relief was not rapid’ (26). Davies and colleagues analysed patient satisfaction based on diaries from two clinical trials. Patients were somewhat satisfied with treatment when pain was completely relieved at 2 h (90%), compared with patients with moderate or severe pain at 2 h (10%). Lack of symptoms by 2 h, and pain relief within 90 min, had a 76% probability that migraineurs would be at least somewhat satisfied. Fast, complete pain relief was one of the most important factors in determining patient satisfaction with treatment (27).
Prior literature suggests that time lost due to impaired functioning is a main contributing factor to the burden associated with migraine. However, the temporal relationship between headache relief and return to functioning has not been rigorously tested. Thus, the aim of this study was to explore the association between the time to headache pain response and the time to a return to functioning, since treatments that reduce the time lost due to impaired functioning will be likely to decrease the burden of migraine. Because research on patient preferences indicates that the restoration of function and rapid relief of symptoms are important characteristics of migraine medication, this study also sought to determine which migraine-related factors were associated with patient acceptability.
Methods
Description of data
Data for this analysis are from a randomized, double-blind, parallel group, placebo-controlled, clinical trial that compared eletriptan 40 mg, sumatriptan 100 mg and placebo in the acute treatment of migraine. Patients enrolled in the trial were provided with a migraine diary card. Patients were instructed to take the study medication when they experienced a ‘typical’ migraine headache of at least moderate pain intensity and to manually complete their diary by recording headache pain severity, functional impairment, presence of migraine-associated symptoms, and recurrence of migraine at multiple time points from baseline (immediately predose) up to 24 h later.
The three key variables from the clinical trial were headache response, functional improvement and treatment acceptability. The first variable, ‘headache response’, was derived from the patient's assessment of headache pain, which was measured on a four-point scale ranging from none, to mild, moderate, or severe, based on the classification criteria put forth by the International Headache Society (1). Headache pain was assessed at baseline, and at 0.5 h, 1 h, 1.5 h, 2 h, 4 h and 24 h postdose. Patients in the clinical trial were classified as having achieved headache response at a given time if they experienced moderate to severe headache pain at baseline, which then resolved to mild vs. none at or before that time post baseline.
‘Functional response’ represents whether or not a patient's functional status improved at various time endpoints after initiation of therapy. Functional impairment was assessed at baseline, and at 0.5 h, 1 h, 1.5 h, 2 h, 4 h and 24 h postdose. Ratings for level of functional impairment ranged from requiring bed rest (severe impairment), to severe impairment of activities not requiring bed rest (moderate impairment), to reduction of activities (mild impairment), to normal functioning (no impairment). A patient was deemed to have achieved functional response if the patient experienced moderate or severe functional impairment at baseline, but then experienced mild to no functional impairment by the respective time postdose.
The third key variable was ‘treatment acceptability.’ Patients were asked to respond to the following question 24 h after the initial attack or recurrence: ‘Given the choice between this and any other medication to treat a migraine attack, would you take this again?’. The patient's dichotomous response to this question (yes/no) was used as a global measure of treatment acceptability.
In addition to the three key variables described above, eight additional variables related to demographic characteristics and migraine-associated symptoms were selected for analysis: presence or absence of nausea, vomiting, photophobia or phonophobia (recorded at baseline, 0.5 h, 1 h, 1.5 h, 2 h, 4 h and 24 h postdose); second dose of treatment; use of rescue medication; patient age, and gender.
Inclusion/exclusion criteria
Patients had a baseline, and at least one post-baseline evaluation. At baseline, patients must have had moderate or severe headache pain, and moderate or severe functional impairment. Only data from patients enrolled in the active therapy arms of the trial (e.g. data from those patients randomized to eletriptan or sumatriptan) were included in the analysis. This analysis was not treatment specific and focused only on data from the first treated attack, although the clinical study was designed to assess the effect of treatment on multiple attacks.
Analysis of functional improvement
The first study aim was to assess whether a greater proportion of patients who achieved a headache response by a given time point would experience a functional response at the same time point. To test this hypothesis, the statistical relationship between headache response and functional response was assessed using a χ2 test of proportions.
The second aim was to assess which clinical response factors were determinants of functional improvement in patients with migraine. The primary independent variable was headache response. The independent variables associated with symptoms were nausea, vomiting, photophobia and phonophobia. Age and gender were also considered. Most of the variables of interest were coded as binary responses (yes/no); only age was left as a continuous variable.
Two logistic regressions were performed to model which clinical factors influenced whether a patient was able to achieve functional improvement by a certain point in time. In the first regression, the dependent variable was functional improvement at 1 h, and the independent variables were headache response at 0.5 h and 1 h, presence or absence of nausea at 1 h, presence or absence of vomiting at 1 h, presence or absence of photophobia at 1 h, presence or absence of phonophobia at 1 h, gender and age. The second regression was nearly identical to the first, with the exception that the dependent variable was functional improvement at 2 h, and headache response at 2 h was included as an independent variable.
Analysis of treatment acceptability
The third aim of the study was to analyse the relationship between treatment acceptability and the independent variables discussed above. For these bivariate analyses, 2 × 2 tables were created using acceptability and variables of interest. The statistical relationship between treatment acceptability and each of these variables was assessed using a χ2 test of proportions.
Similar to the analysis for functional responses, logistic regressions were performed to model which clinical factors influenced whether a patient reported that the treatment was acceptable. It was hypothesized that patients who had achieved functional improvement would be more likely to find treatment acceptable 24 h after triptan dosing vs. patients who did not achieve functional improvement. For each model, the dependent variable was the binary response variable for overall treatment acceptability.
Functional improvement at 2 h was selected as the primary independent variable in our models. The other independent variables in the models were headache response, age, gender, use of rescue medications and use of second dose of active treatment. Based on the initial results of a bivariate analysis that considered the relationship between treatment acceptability, and the four migraine-associated symptoms (photophobia, phonophobia, nausea or vomiting), a dummy variable representing the presence or absence of any of the four migraine-associated symptoms at 2 h was created, and used in lieu of the individual variables themselves.
Three models were developed to describe the impact of the variables of interest on acceptability of treatment. The first model included the independent variables described above, along with headache relief at 0.5 h. For the second model, headache relief at 1 h was substituted for headache relief at 0.5 h. In the third model, headache relief at 2 h replaced headache relief at 0.5 h. All other variables remained the same.
Results
Patient demographics
Table 1 provides basic demographics and symptom frequency data for patients enrolled in the trial. Of the 1355 patients who met the inclusion/exclusion criteria, 1173 (86.6%) were female, with a mean age of 42 years (median 43 years). Nearly equal numbers of patients were randomized to the two active treatments. Table 1 gives the percentage of patients experiencing symptoms associated with migraine at baseline (t = 0), 0.5 h, 1 h and 2 h. At baseline, 67% of patients experienced nausea, 78% had photophobia and 70% reported phonophobia. Fewer than 8% of patients experienced vomiting at baseline. At 2 h, the proportion of patients experiencing symptoms decreased by approximately half (nausea 31%, vomiting 4%, photophobia 35% and phonophobia 32%).
Demographic and clinical characteristics

Table 1 also reports the levels of headache pain and functioning impairment at baseline and at subsequent time points. At baseline, 54% patients were experiencing moderate headache pain and 46% were experiencing severe headache pain. Six per cent of patients achieved headache response by 0.5 h, while 26% experienced response by 1 h and 61% experienced response by 2 h. Seventy-one per cent of patients had moderate functional impairment at baseline, and 30% had severe functional impairment. By 0.5 h, 9% of patients had achieved functional response. This increased to 31% at 1 h and 65% at 2 h. Sixty per cent of patients found treatment acceptable.
Analysis of functional improvement
Bivariate analysis
A significantly greater proportion of patients who had headache response at 0.5 h achieved functional response at 0.5 h, 1 h and 2 h compared with patients who did not achieve headache response at one-half hour (χ2, P < 0.0001 for all comparisons).
Similarly, a significantly greater proportion of patients who had headache response at 1 h experienced functional responses at 1 and 2 h. This trend continued over time, as a significantly greater proportion of patients who had headache response at 2 h achieved functional response at 2 h, compared with those who had not achieved headache response at two hours (χ2, P < 0.0001 for all comparisons).
Multivariate analysis
For the first functional improvement model, headache response at 1 h was associated with a significant positive impact on functional response [odds ratio (OR): 67.38, 95% confidence interval (CI): 42.12, 107.79]. The presence of nausea, photophobia and phonophobia all had a significant negative impact on functional response with odds ratios, respectively, equal to 0.41, 0.40, and 0.58 (Table 2). The variable representing vomiting at 1 h was dropped from this model, because none of the patients had experienced both functional response at 1 h and vomiting at 1 h.
Logistic regression estimates for functional response models
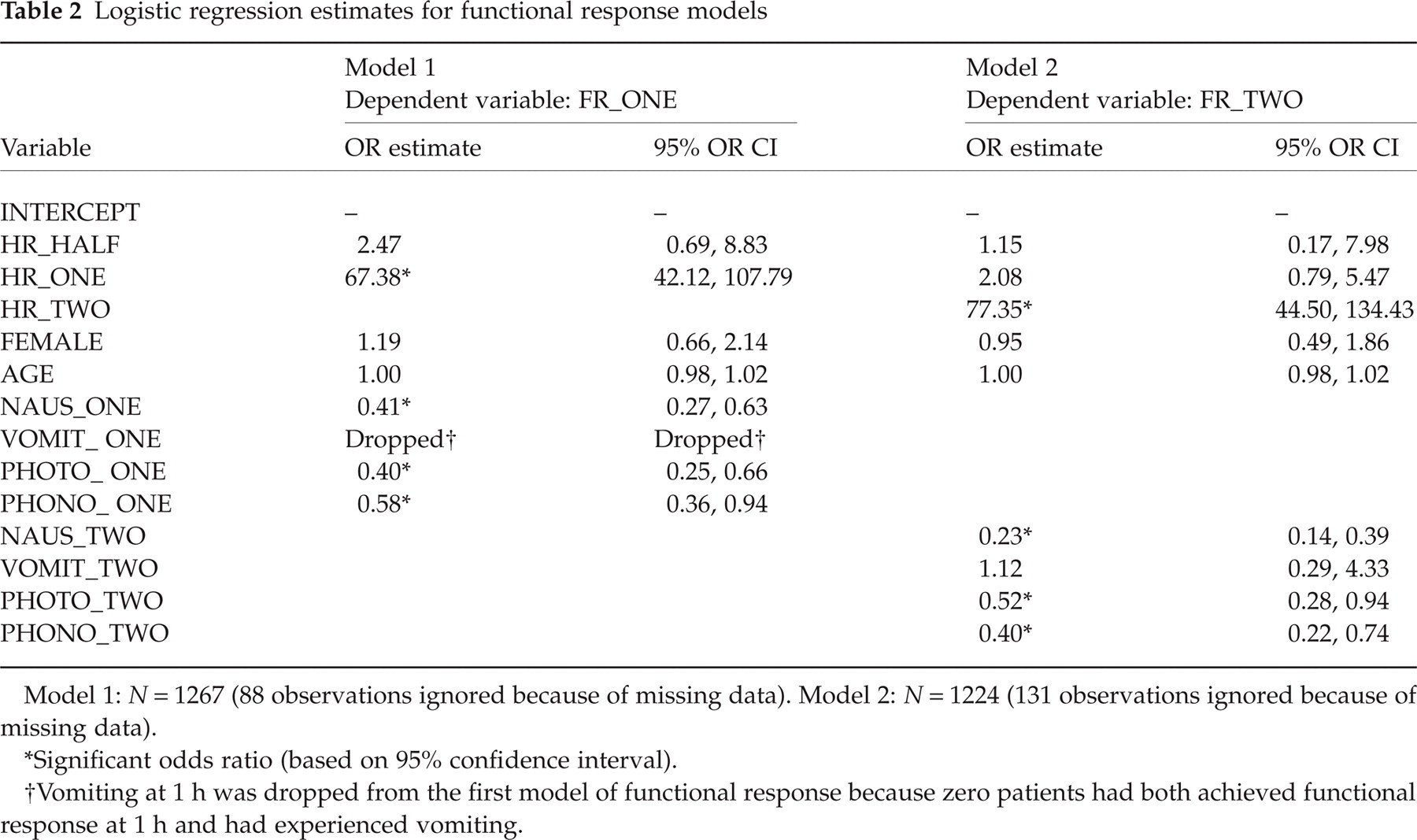
Model 1: N = 1267 (88 observations ignored because of missing data). Model 2: N = 1224 (131 observations ignored because of missing data).
Significant odds ratio (based on 95% confidence interval).
Vomiting at 1 h was dropped from the first model of functional response because zero patients had both achieved functional response at 1 h and had experienced vomiting.
In the second functional improvement model, headache response at 2 h was associated with the highest significant positive impact on the likelihood of functional response (OR: 77.35, 95% CI: 44.50, 134.43). In this analysis, all but one migraine-associated symptoms had a significant impact on the odds of achieving functional response (Table 2). The presence of nausea had a strong negative impact on functional response, as did photophobia and phonophobia. For both functional response models, the likelihood ratio test of the global null hypothesis (β= 0) indicated that the estimates yielded were significantly different from zero (P < 0.0001).
Analysis of treatment acceptability
Bivariate analysis
Statistical analysis revealed that patients who continued to experience one of the four symptoms (photophobia, phonophobia, nausea and vomiting) at 1 and 2 h were significantly less likely to find the treatment acceptable (χ2, P < 0.05). Patients who achieved both headache response and functional response at 0.5 h, 1 h and 2 h were significantly more likely to find the treatment acceptable (χ2, P < 0.05).
Multivariate analysis
In the first model of treatment acceptability, those patients who achieved functional response at 2 h were significantly more likely to have found the treatment acceptable vs. those who did not achieve functional response (OR: 2.56, 95% CI: 1.82, 3.58). Patients who had experienced one or more of the migraine-associated symptoms at 2 h were significantly less likely to have found treatment acceptable vs. those who experienced no symptoms; additionally, those patients who reported use of rescue medications were significantly less likely to have found treatment acceptable compared with those who did not use rescue medications (Table 3).
Logistic regression estimates (dependent variable: treatment acceptability)
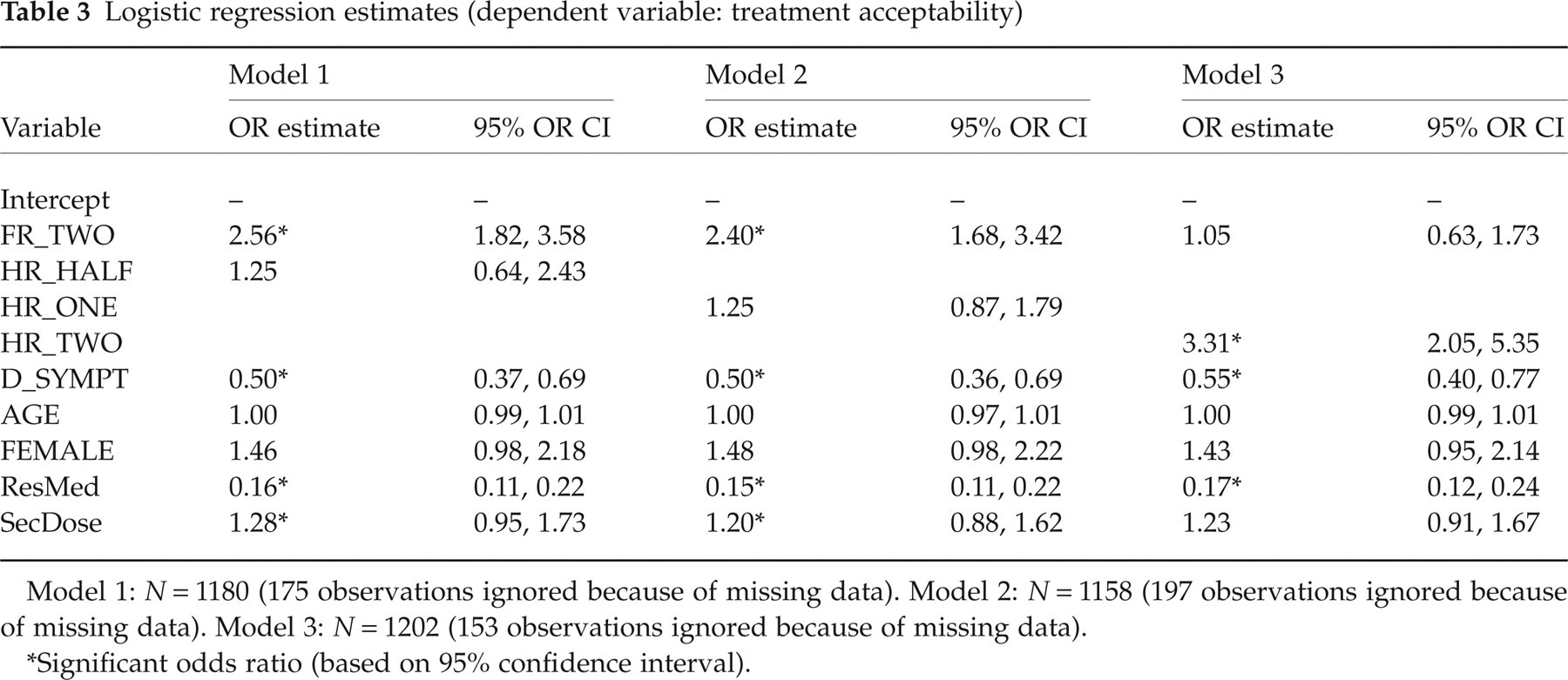
Model 1: N = 1180 (175 observations ignored because of missing data). Model 2: N = 1158 (197 observations ignored because of missing data). Model 3: N = 1202 (153 observations ignored because of missing data).
Significant odds ratio (based on 95% confidence interval).
The results for the second model are consistent with the results of the first model. The same three variables (functional response at 2 h, presence of one or more of the migraine-associated symptoms and use of rescue medication) were deemed to have a significant impact on the acceptability of treatment (Table 3).
The third model included headache response at 2 h. Consequently, functional response at 2 h was no longer significant. Thus, the model predicts that headache response at 2 h, presence of one or more of the migraine-associated symptoms and use of rescue medication significantly impact acceptability of treatment (Table 3). Interestingly, in all three models the use of a second dose of medication is not a significant independent predictor of acceptability.
In the three models for acceptability, the likelihood ratio test of the global null hypothesis (β= 0) showed that the estimates yielded are significantly different (P < 0.0001). Additionally, for each of the three models, the analysis of predicted probabilities indicated a concordance rate of approximately 80%.
Discussion
The relationships among headache response, return to normal functioning and treatment acceptability are clinically and economically important considerations in the selection of appropriate migraine therapy. The results of this study suggest that migraineurs who experience rapid headache pain response obtain a faster return to functioning. The analyses show a direct temporal relationship among these key determinants of migraine resolution. Rapid headache pain response and functional response were found to be the main attributes that correlate with treatment acceptability among migraineurs. Considering the negative effects of impaired functioning, our study suggests that a faster headache response could have a positive effect on the burden associated with migraine. Faster headache response was associated with a decrease in the time lost to an impaired functional status, and an increase in treatment acceptability from migraineurs. These results suggest that a treatment providing faster headache response could probably reduce the total burden associated with migraine by decreasing productivity loss, presenteeism and absenteeism, and impaired family and social interactions.
This study is unique in showing the temporal relationship between headache response and functional response. Our analysis presents functional response at 0.5, 1 and 2 h for patients who are successfully treated at 0.5, 1 and 2 h. With effective treatment at 1 h, functional response is likely at either 1 or 2 h. Additionally, a significant number of patients who are effectively treated for pain at 2 h also achieved functional response at 2 h. Headache pain response at 1 h is associated with the highest significant impact on functional response at 1 h. These results are similar for functional status at 2 h. Our findings clearly suggest that faster headache pain response results in a faster return to functioning.
While headache pain response was positively associated with functional improvement, migraine symptoms were negatively correlated with an improvement in functioning. Absence of nausea and photophobia were associated with return of functioning at 1 h. Although there was a negative association between presence of phonophobia and functional response, this association was weaker compared with photophobia and nausea. Resolution of negative symptoms can hasten the process of functional return in migraine patients. Our results confirm that important determinants of functional status are the level of pain and migraine-associated symptoms. These results have important implications, as treatments that shorten the duration of headache and migraine-associated symptoms could probably reduce the time patients spend with impaired functioning.
The results of this study are consistent with prior findings regarding patient satisfaction with treatment. Headache response and functional return were the main factors of acceptability of treatment to patients. Migraineurs with headache response, and functional response at 0.5, 1 and 2 h were likely to find treatment acceptable. Patients who did not experience migraine-related symptoms were also inclined to find treatment acceptable. This study indicates that factors which deterred patients from accepting treatment include lack of treatment efficacy and slow onset of pain relief.
Understanding patients’ perspectives when making treatment decisions may result in better outcomes, and satisfaction with care (28). Ideally, a medication with faster pain relief will also enable faster return to functioning. Since these attributes are associated with acceptability, there is a higher chance that patients will show functional improvement, adhere to medication and subsequently reduce their suffering and that of their family members, as well as reduce the economic burden associated with migraine.
These study results are based on data from patients enrolled in a clinical trial. These patients may differ from typical migraineurs and generalization of the results to the out-patient population should be made with caution. Additionally, all data in this study were reported by patients through the use of diaries or through the use of scales which, although widely used in migraine clinical research, have not been validated.
Conclusion
The results of this study suggest a direct temporal relationship among the key determinants of migraine resolution. Rapid headache response is associated with faster return to functioning, and rapid headache and functional responses are significant attributes of treatment acceptability.
This study provides new insight regarding migraine treatment and factors associated with faster return to functioning, and acceptability. Additional prospective studies are warranted for further investigation of the relationship between earlier headache relief and functional improvement, and patient-reported treatment acceptability. Also, future studies may be necessary to evaluate the relationship of migraine symptoms with functional response over a longer time interval.
Footnotes
Acknowledgements
We thank Lisa Blatt MA, Medical Writer, for her final edits. This project was supported in part by a non-restricted predoctoral fellowship grant from Pfizer, Inc.