
Abstract
The goal of the present study was to test the impact of administration time of the angiotensin II type 1–receptor blocker candesartan on cerebral blood flow (CBF), infarct size, and neuroscore in transient cerebral ischemia. Therefore, 1-hour middle cerebral artery occlusion (MCAO) was followed by reperfusion. Rats received 0.5-mg/kg candesartan intravenously 2 hours before MCAO (pretreatment), 24 hours after MCAO, every 24 hours after MCAO, or 2 hours before and every 24 hours after MCAO. Infarct size (mm3) and a neuroscore at day 7 were compared with controls. CBF was quantified by radiolabeled microspheres and laser-Doppler flowmetry. Compared with controls (95 ± 8), infarct size in candesartan-treated groups was smaller (59 ± 5, 68 ± 10, 28 ± 3, and 15 ± 3, respectively; P < 0.05). Although there was no difference in neuroscore between pretreatment and controls (1.55 ± 0.18, 1.80 ± 0.13), other treatment regimens resulted in improved neuroscores (1.33 ± 0.16, 1.11 ± 0.11, 0.73 ± 0.15; P < 0.05). CBF in pretreated animals at 0.5 hours after MCAO was significantly higher than in controls (0.58 ± 0.09 mL · g−1 ·· min−1 and 44% ± 7% of baseline compared with 0.49 ± 0.06 mL · g−1 ·· min−1 and 37% ± 6%, microspheres and laser-Doppler flowmetry; P < 0.05). Thus, candesartan reduces infarct size even if administered only during reperfusion. Apart from pretreatment, other treatment regimens result in significantly improved neuroscores. In the acute phase of cerebral ischemia, candesartan increases CBF.
Keywords
Complete occlusion of the middle cerebral artery (MCA) occurs in 10% to 15% of stroke patients. With the emergence of aggressive therapies for ischemic stroke, such as thrombolysis with subsequent reperfusion (Hacke et al., 1995;NINDS rt-PA Stroke Study Group, 1995), the clinical prognosis of patients with such infarcts could be improved. The severity of clinical manifestations after transient cerebral ischemia depends mainly on the location and size of the infarcted brain area (Hunter et al., 1998).
The ischemia-induced changes and functional impairments after permanent or transient occlusion of the MCA in rats closely resemble those observed after focal occlusion of the MCA in humans (Yamori et al., 1976), resulting in the frequent use of rat models of cerebral ischemia to examine neuroprotective agents (Müller et al., 1995). Long-term pretreatment with angiotensin-converting enzyme inhibitors or angiotensin II type 1 (AT1)-receptor blockers prevented the occurrence of cerebral ischemia in stroke-prone, spontaneously hypertensive rats and salt-loaded Dahl salt-sensitive rats (Inada et al., 1997;Stier et al., 1993;von Lutterotti et al., 1992). Additionally, angiotensin-converting enzyme inhibitors exert beneficial effects on the metabolic and circulatory derangement in the ischemic brain in spontaneously hypertensive rats (Sadoshima et al., 1993) and improve neurologic recovery from cerebral ischemia in normotensive rats (Werner et al., 1991).
Nishimura and colleagues showed that pretreatment with the AT1-receptor blocker candesartan resulted in significantly reduced infarct size from transient cerebral ischemia in hypertensive and normotensive rats (Nishimura et al., 2000a). Additionally, pretreatment with the intracerebroventricularly infused AT1-receptor blocker irbesartan resulted in a significantly improved neurologic outcome at 24 hours after vessel occlusion (Dai et al., 1999). However, no data exist on the impact of time of AT1-receptor blocker administration (single or chronic, pretreatment or posttreatment) in transient cerebral ischemia. In particular, it is unclear whether posttreatment with AT1-receptor blockers achieves any benefit in terms of infarct size reduction or improved neurologic outcome. In addition, data on the influence of AT1-receptor blocker administration on cerebral blood flow (CBF) in the acute phase of cerebral ischemia as one potential mechanism of reduced infarct size are still lacking.
Therefore, the present study was designed to evaluate the effects of single AT1-receptor blocker before and after treatment as well as chronic pretreatment and posttreatment in transient cerebral ischemia in normotensive rats on blood pressure and CBF, infarct size, and neurologic outcome.
MATERIALS AND METHODS
For all experiments, male Sprague-Dawley rats (280–320 g) were used. Animals were allowed free access to food. The local authorities approved the study.
Part I: Impact of time of AT1-receptor blocker administration on infarct size and neurologic outcome
Focal cerebral ischemia was induced in 50 rats using an intraluminal suture occlusion model of the MCA first described by Longa et al. (1989). This endovascular stroke model is a well-established and ideal model because it resembles human embolic stroke as closely as possible and allows reperfusion by withdrawal of the occluding suture. For preparation, rats were anesthetized with ketamine (4 mg/100 g) and xylazine (1.5 mg/100 g) by intramuscular injection. During surgery, monitoring of hematocrit, pH, PO2, PCO2, and blood pressure was performed using a femoral artery catheter. Rectal temperature was maintained at 37°C with a feedback-regulated heating pad.
In all animals, the right MCA was occluded as previously described in detail (Engelhorn et al., 2003). To maximize beneficial reperfusion effects, we chose 1 hour of permanent MCA occlusion (MCAO) (Engelhorn et al., 2003).
The 50 animals were assigned to five treatment groups (n = 10 for each group). Animals in group A (single pretreatment) received 0.5-mg/kg candesartan intravenously through the tail vein 2 hours before MCAO. This dose of candesartan has previously been shown to significantly reduce infarct size after cerebral ischemia with reperfusion (Nishimura et al., 2000). Animals in group B (single posttreatment) received candesartan at 24 hours after MCAO, whereas animals in group C received candesartan every 24 hours after MCAO until the end of reperfusion (chronic posttreatment). Animals in group D (combined pretreatment and posttreatment, chronic treatment) received candesartan 2 hours before MCAO and every 24 hours after MCAO. Animals in group E only underwent MCAO and reperfusion and served as controls. At day 7, all surviving animals were examined neurologically using an established scoring system (Bedersen et al., 1986a;Menzies et al., 1992) (Table 1). Body weight was also measured. Animals were then reanesthetized and killed. The brains were rapidly removed and 1-mm brain slices were incubated for 30 minutes in a 4% solution of 2,3,5 triphenyltetrazolium-chloride (TTC) at 37°C and fixed by immersion in 10% buffered formalin solution (Bedersen et al., 1986b). Finally, the TTC-stained brain sections were photographed, digitized, and quantified using a computer system. On each slice, the nonstained area (ischemic brain) was marked and the infarct size was calculated according to the slice thickness of 1 mm per slice. An investigator blinded to the treatment groups performed all measurements and calculations of infarct volume. To avoid overestimation of infarct size, the corrected infarct size was calculated (Lin et al., 1993).
Neurologic score after MCAO according to Bedersen et al. (1986) and Menzies et al. (1992)
MCAO, middle cerebral artery occlusion.
Part II: Impact of AT1-receptor blocker administration on cerebral blood flow and blood pressure in the acute phase of ischemia
The study protocol consisted of two groups. Animals in group A (n = 7) received 0.5-mg/kg candesartan intravenously through the tail vein 2 hours before MCAO. Animals in group B (n = 7) served as controls and received no pretreatment. All animals underwent MCAO and reperfusion at 1 hour after MCAO. Absolute CBF was measured by injection of radioactive labeled microspheres into the left ventricle immediately before and at 30 minutes after MCAO.
The rats were initially anesthetized with ketamine and xylazine, intubated, and ventilated with air to keep the blood gases within the physiologic range. Rectal temperature was maintained at 37°C with a feedback-regulated heating pad. The femoral artery and vein were catheterized to monitor blood pressure and for withdrawal of the arterial reference blood samples. Hemodynamic parameters reported are heart rate and left ventricular end-diastolic and peak pressures. For application of radiolabeled microspheres (15-μm diameter, 141CE, 95Nb, and 46Sc; NEN, Du Pont Co., Boston, MA, U.S.A.), a thoracotomy was performed and the heart was exposed. The microspheres were injected directly into the left ventricle to determine the regional blood flow and its distribution through the brain. This procedure has been validated for the determination of myocardial blood flow (Schulz et al., 1992). For CBF measurement, approximately 2 × 105 microspheres supplied in 0.1 mL saline with 0.002% tween 80 were injected. The withdrawal of the arterial reference blood samples was started 15 seconds before injection of the microspheres and continued for 45 seconds at a rate of 1 mL/min (Withdrawal Pump model 901A; Harvard Apparatus, South Natrick, MA, U.S.A.). To prevent a significant decline in hematocrit due to the withdrawal of the arterial reference blood sample, blood was replaced by injecting 1 mL blood from a donor animal during the time of withdrawal of the reference sample into the femoral vein.
At the end of the experiment, all animals were killed and brain sections were stained with TTC to calculate infarct size. The three central brain slices were then dissected into the right and the left hemisphere. Radioactivity of each brain sample and the reference blood withdrawal samples were counted for 3 minutes in a germanium counter; the peak to noise ratio was always above 100:1. Regional CBF was then calculated for the infarcted and noninfarcted hemisphere, as previously described in detail (Schulz et al., 1992).
Part III: Impact of AT1-receptor blocker administration on relative cerebral blood flow in the MCA-supplied cortex and blood pressure in the chronic phase
The study protocol consisted of two groups of rats. Animals in group A (n = 7) received 0.5-mg/kg candesartan intravenously through the tail vein 2 hours before MCAO and every 24 hours after MCAO until the end of reperfusion. Animals in group B (n = 7) served as controls and received no pretreatment. All animals underwent MCAO and reperfusion at 1 hour after MCAO. To ensure proper reperfusion and to monitor relative CBF in the MCA-supplied cortex in the acute phase of ischemia and after reperfusion, laser-Doppler flowmetry (LDF) was used.
The occluding suture was inserted into the internal carotid artery but not pushed intracranially. Animals were then immobilized in a stereotactic frame and the skull was exposed with a midline sagittal incision and a burr hole with a diameter of 2 mm was performed at 3 mm to the right and 4 mm anterior to the lambda suture. The dura was pierced and a single-fiber LDF probe, mounted on a micromanipulator, was placed on the cerebral cortex. For MCAO, the suture was gently advanced into the internal carotid artery till a resistance was felt.
We used a Moor Blood Perfusion monitor (MBF 3D; Moor Instruments, Axminster, U.K.) with a low-power (1.6 mW) laser diode as source of coherent light (820 nm) and a single-fiber probe with a diameter of 0.1 mm. Parameters were measured within an estimated tissue volume of 0.4 mm3. The LDF values were collected over a period of 10 minutes before MCAO and were averaged as baseline (100%) followed by 90 minutes of continuous measurement.
At day 7, all surviving animals were examined neurologically and the body weight was measured. Animals were then reanesthetized and the second femoral artery was catheterized for monitoring of blood pressure. Animals were then killed and infarct size was calculated by TTC staining.
Statistical analysis
For statistical analysis, commercial software (StatView; Brain Power Inc., Miami, FL, U.S.A.) was used. One-way analysis of variance and Fisher least significant difference test were used for statistical analysis of infarct size, body weight, CBF (microspheres and LDF) and blood parameters; the Kruskal-Wallis test was used for statistical analysis of the neurologic score, and a probability value of P < 0.05 was considered to be significant (represented as asterisks in tables and figures). The means and standard deviations are presented for the various groups.
RESULTS
Part I: Impact of time of AT1-receptor blocker administration on infarct size and neurologic outcome
One animal in group A (pretreatment) and one animal in group D (chronic posttreatment) were excluded from data analysis. Both animals died within 30 minutes after MCAO and had massive subarachnoid hemorrhage due to vascular perforation with the suture.
No statistically significant differences were noted in the remaining 48 animals among the five groups for any of the intraoperative physiologic parameters. Throughout the surgical preparation, the average body temperature for all animals was 36.9 ± 0.5°C (mean ± SD). Arterial blood gases (PO2, 103 ± 19 mm Hg; PCO2, 38 ± 6 mm Hg; pH, 7.37 ± 0.04) and hematocrit (40.6% ± 2.8%) remained stable.
Body weight
All animals of the study had a decline in body weight. Body weight is expressed as percentage of initial weight. Seven days after MCAO, the average body weight of the control group E was 83% ± 3%. In animals undergoing candesartan pretreatment (group A), the average body weight was 83% ± 2% (not significant compared with controls). The average body weights of animals undergoing single posttreatment (group B), chronic posttreatment (group C), and combined pretreatment and posttreatment (group D) were 94% ± 1%, 95% ± 1%, and 95% ± 1%, respectively. Compared with controls and animals undergoing pretreatment, the loss in body weight of these animals was significantly smaller.
Neurologic score
Fig. 1 illustrates the neurologic scores at day 7 after MCAO. The neurologic scores of the controls (group E) and animals undergoing candesartan pretreatment (group A) were not significantly different. Neurologic scores of animals undergoing single posttreatment (group B), chronic posttreatment (group C), and combined pretreatment and posttreatment (group D) were significantly reduced compared with controls. Additionally, compared with animals undergoing single pretreatment and posttreatment, the neurologic scores of animals undergoing chronic posttreatment and combined pretreatment and posttreatment were significantly lower (P < 0.05).
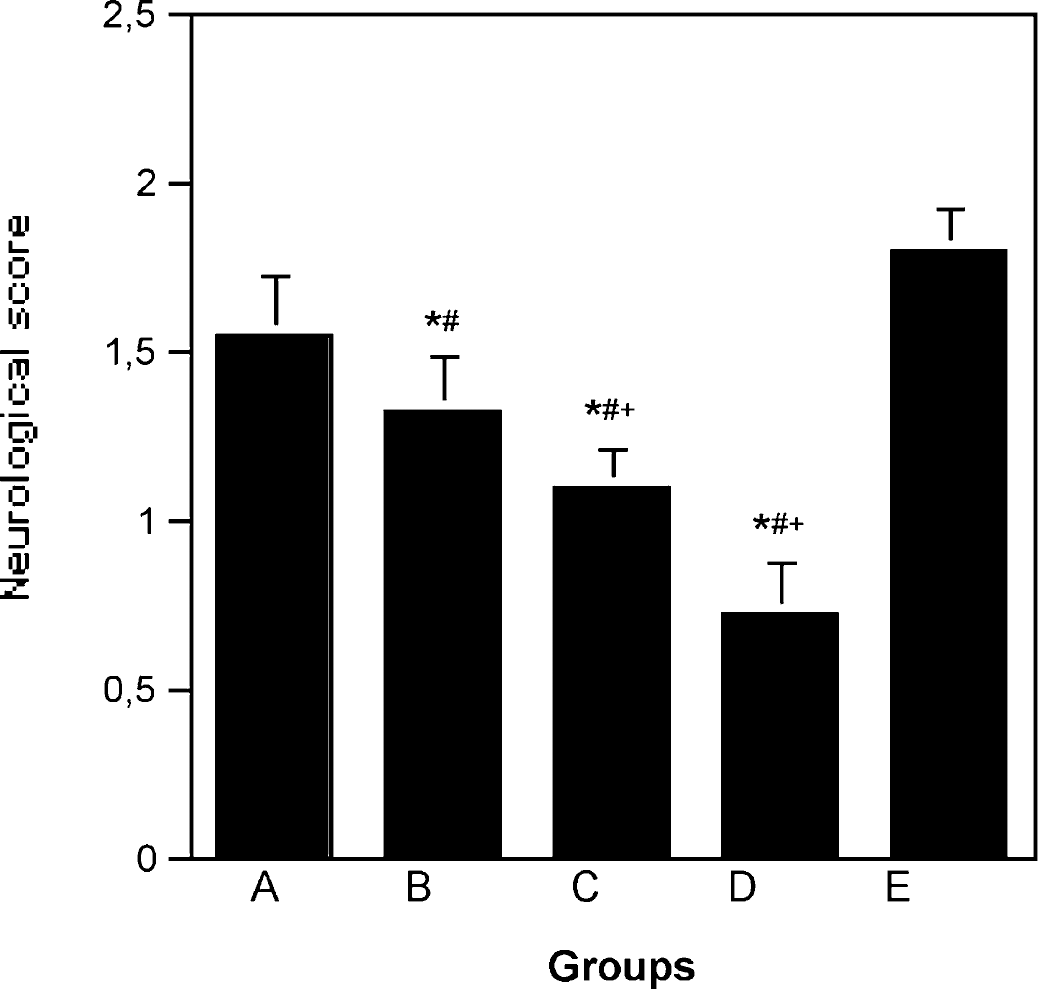
Neurologic scores at day 7 after MCAO. Animals in group B (single posttreatment), group C (chronic posttreatment), and group D (combined pretreatment and posttreatment) had better (lower) neurologic scores than controls (group E). Pretreatment 2 hours before MCA occlusion (group A) did not improve neurologic score after ischemia and reperfusion. *P < 0.05 compared with control group E; #P < 0.05 compared with pretreatment group A; †P < 0.05 compared with posttreatment group B.
Infarct size
Fig. 2 shows TTC-derived infarct size at day 7 after MCAO. Fig. 3 illustrates TTC-stained coronal brain slices at the level of the optic chiasm of one animal undergoing combined pretreatment and posttreatment (group D) and a control (group E).
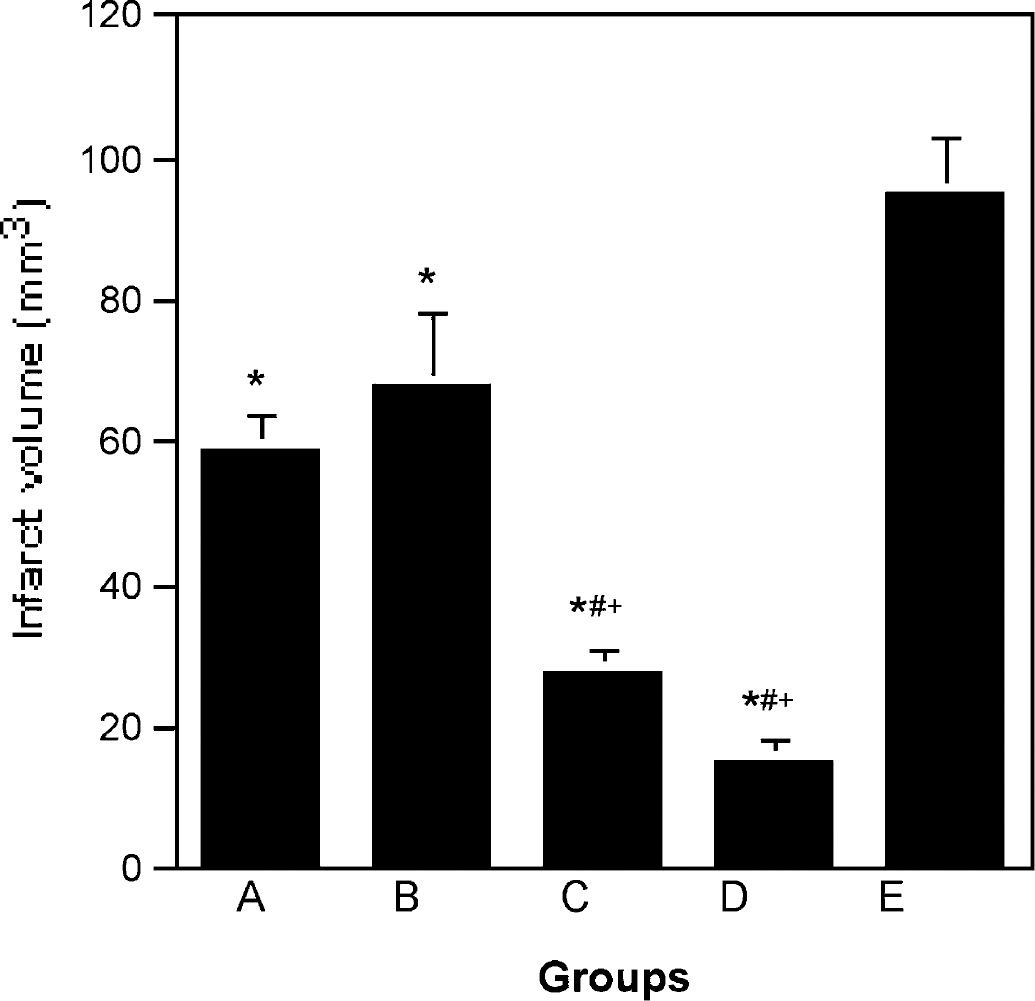
The TTC-derived absolute infarct size at day 7 after MCAO. All animals undergoing candesartan treatment (groups A—D) had significantly smaller infarct size than controls (group E). Chronic posttreatment (group C) and combined pretreatment and posttreatment (group D) resulted in significantly smaller infarct size than single pretreatment (group A) and single posttreatment (group B). *P < 0.05 compared with control group E; #P < 0.05 compared with pretreatment group A; †P < 0.05 compared with posttreatment group B.

The TTC-stained coronal brain slices on the level of the optic chiasm of one animal undergoing combined pretreatment and posttreatment (group D) and one control (group E). The animal undergoing combined pretreatment and posttreatment (left) had a smaller infarct size than the control (right).
Total brain volume did not differ among all groups (data not shown; lowest brain volume was 1,262 ± 98 mm3 in group A, highest was 1,327 ± 84 mm3 in group B). In rats undergoing single pretreatment (group A), single posttreatment (group B), chronic posttreatment (group C), and combined pretreatment and posttreatment (group D), infarct size was significantly reduced compared with controls (group E). There was no significant difference in infarct size in animals undergoing single pretreatment (group A) compared with single posttreatment (group B). Compared with single pretreatment and posttreatment, chronic posttreatment (group C) and combined pretreatment and posttreatment (group D) resulted in further reduced infarct size (P < 0.05).
Part II: Impact of AT1-receptor blocker administration on cerebral blood flow and on blood pressure in the acute phase of ischemia
There were no significant differences in any measured physiologic parameter (Table 2) under baseline conditions (i.e., after intubation and ventilation, thoracotomy, and preparation of the neck vessels immediately before advancement of the suture) between groups A and B. In candesartan-pretreated animals in group A, there was no decline in blood pressure for all measured time points compared with control animals in group B.
Physiologic parameters for animals of group A and B (part II)
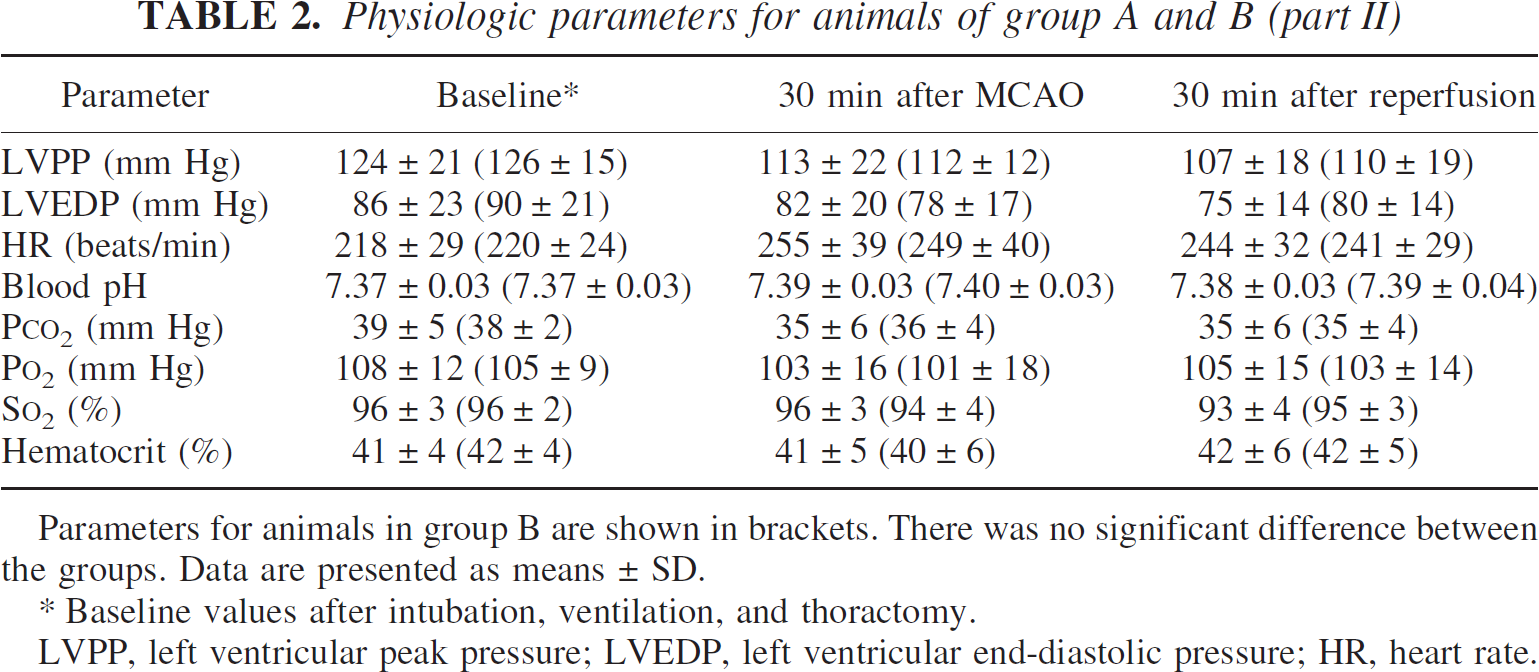
Parameters for animals in group B are shown in brackets. There was no significant difference between the groups. Data are presented as means ± SD.
Baseline values after intubation, ventilation, and thoractomy.
LVPP, left ventricular peak pressure; LVEDP, left ventricular end-diastolic pressure; HR, heart rate.
In both groups, after advancement of the occluding suture and in the reperfusion phase, the left ventricular end-diastolic pressure and the left ventricular peak pressure decreased, whereas heart rate increased significantly compared with baseline (P < 0.05). Blood pH, hematocrit, PCO2, PO2, and oxygen saturation were stable over time.
TTC-derived infarct size
None of the animals experienced subarachnoid hemorrhage. All animals survived until 2 hours after MCAO, and hence, infarct size was calculated from TTC stained brain sections for these animals. The absolute infarction volume was 36 ± 10mm3 in candesartan pretreated animals in group A and 99 ± 9 mm3 in control animals in group B. Infarct volume in group A was significantly reduced compared with group B (P < 0.05).
Microspheres-derived cerebral blood flow
Fig. 4 shows the absolute CBF immediately before and at 30 minutes after MCAO in both groups. Absolute CBF in the infarcted hemisphere of candesartan pretreated animals (group A) measured at baseline conditions and at 30 minutes after MCAO was significantly higher than in controls (group B).
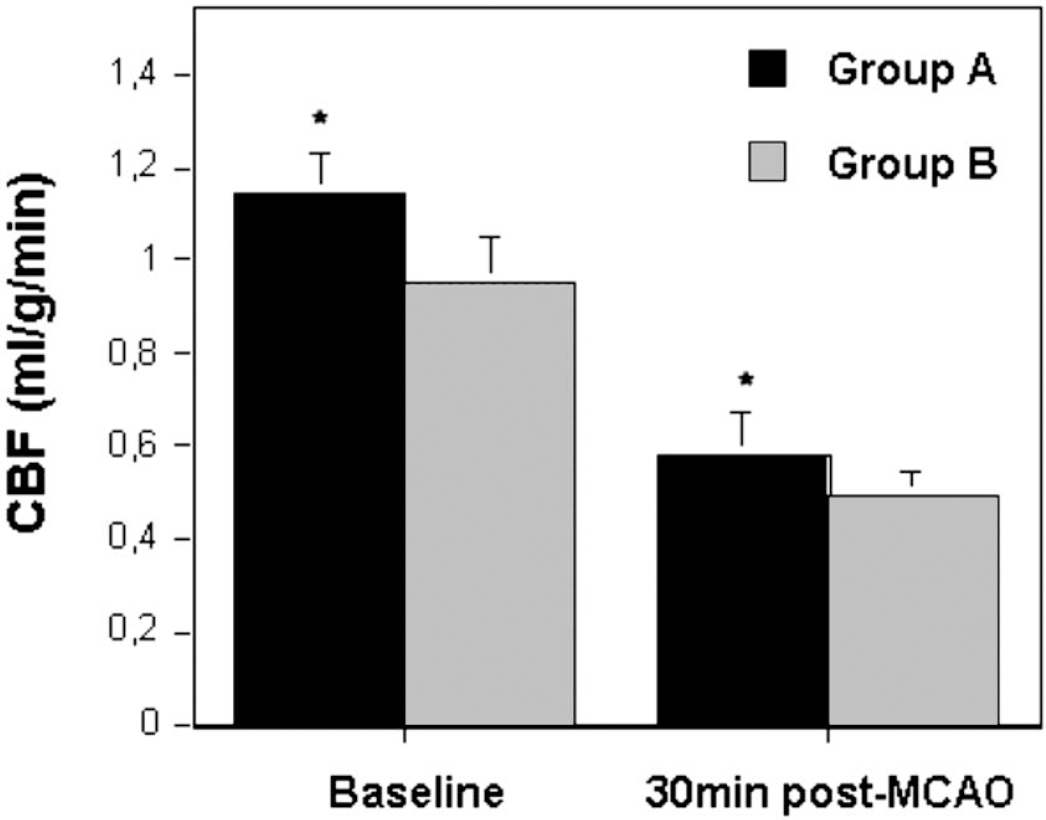
Radiolabeled microspheres-derived absolute CBF immediately before and at 30 minutes after MCA occlusion in the infarcted hemisphere of both groups. Candesartan pretreated animals (group A) had a significantly higher absolute CBF than controls (group B). *P < 0.05 compared with control group B.
Part III: Impact of AT1-receptor blocker administration on relative cerebral blood flow in the MCA-supplied cortex and blood pressure in the chronic phase
No animal died due to a suture perforation. No statistically significant differences were noted in the 14 animals between the two groups for any of the intraoperative physiologic parameters. Throughout the surgical preparation, the average body temperature for all animals was 37.0° ± 0.5°C. Arterial blood gases (PO2, 105 ± 16 mm Hg; PCO2, 37 ± 5 mm Hg; pH, 7.37 ± 0.04) and hematocrit (41.0% ± 2.4%) remained stable.
At 168 hours after MCAO, there was no significant difference between the candesartan-pretreated or candesartan-posttreated animals (group A) and the controls (group B) in systolic and diastolic pressure with 112 ± 24/80 ± 17 mm Hg and 115 ± 29/82 ± 17 mm Hg, respectively.
Body weight, neurologic score, and infarct size
Compared with control animals in group B, candesartan-pretreated and candesartan-posttreated animals in group A had a significantly smaller loss in body weight, better neurologic score, and smaller infarct size at day 7 after MCAO (95% ± 1%, 0.86 ± 0.35 mm3, and 25 ± 6 mm3 compared with 84% ± 3%, 1.86 ± 0.35 mm3, and 108 ± 12 mm3, respectively; P < 0.05).
Laser-Doppler flowmetry—derived perfusion changes
Fig. 5 shows the relative CBF measured with LDF in the MCA-supplied cortex of both groups over a period of 90 minutes. Candesartan-pretreated and candesartan-posttreated animals in group A had a significantly (P < 0.05) higher relative CBF at 30 and 60 minutes after MCAO (44% ± 7% and 41% ± 8%) than animals in control group B (37% ± 5% and 33% ± 6%). At 30 minutes after reperfusion, there was no significant difference between the two groups (108% ± 22% vs. 109% ± 24%).
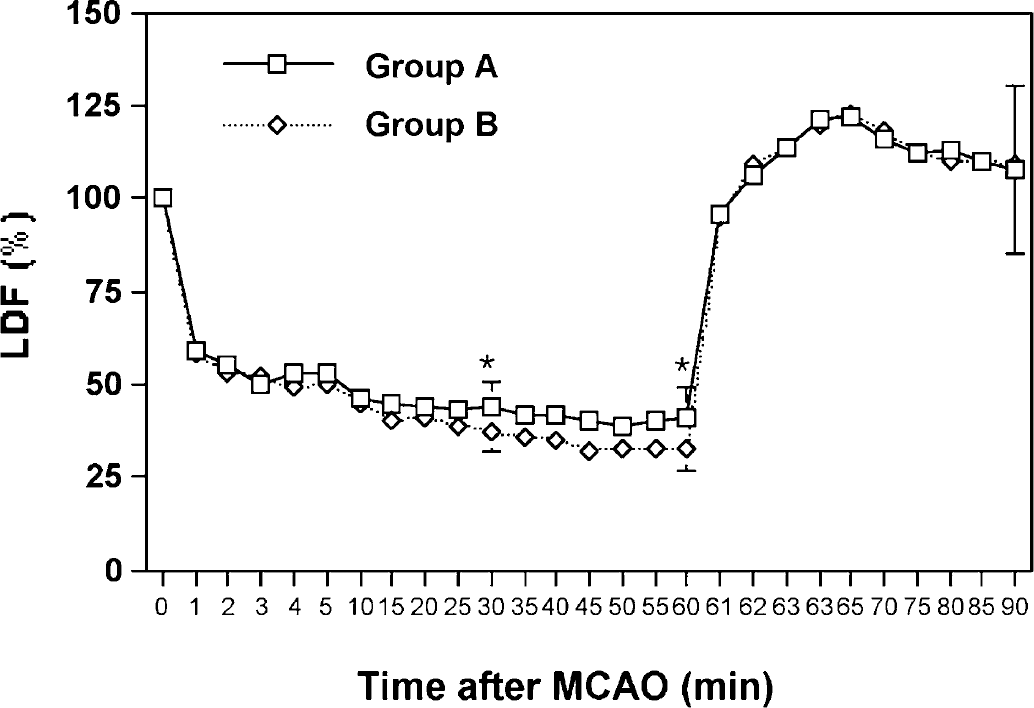
Relative CBF measured with LDF in the MCA-supplied cortex of both groups over a period of 90 minutes after MCAO. Candesartan-pretreated animals (group A) had a significantly higher relative CBF at 30 and 60 minutes after MCA occlusion than controls (group B). After reperfusion, all animals showed hyperemia (> 100%) in the MCA-supplied cortex. At 30 minutes of reperfusion, there was no significant difference in relative CBF between both groups. *P < 0.05 compared with control group B.
DISCUSSION
The present study investigated the effects of time of administration of the AT1-receptor blocker candesartan on infarct size and neurologic outcome after transient cerebral ischemia in normotensive rats. Additionally, effects on CBF (absolute and relative) in the acute phase of cerebral ischemia and effects on blood pressure in the acute phase (90 minutes after MCA occlusion) and in the chronic phase (7 days after MCA occlusion) were studied.
By comparing TTC-derived infarct size, loss in body weights, and neurologic scores at 7 days after MCA occlusion, this study shows that (1) single candesartan administration 2 hours before MCA occlusion significantly reduces infarct size. Compared with controls, infarct size was nearly 40% smaller. Using radiolabeled microspheres and LDF, we showed that (2) the protective effect of candesartan when given before vessel occlusion is probably due to an increase in CBF in the acute phase of ischemia. Nevertheless, neurologic score and loss in body weight were not improved. (3) For the first time, the present study shows that single and chronic candesartan treatment starting no earlier than 24 hours after MCA occlusion still result in significant reduction of infarct size. Importantly, neurologic scores and body weight of animals undergoing posttreatment were significantly better preserved than in controls. (4) Combined pretreatment and chronic posttreatment achieved the best results. Infarct size in these animals was more than 80% smaller than in controls. Like with single and chronic posttreatment, neurologic score and body weight were better preserved. (5) The neuroprotective dose of candesartan in the present study had no significant effect on blood pressure in both the acute and chronic phase of cerebral ischemia.
Our first result is well known and therefore confirmatory; Nishimura and colleagues pretreated spontaneously hypertensive rats and normotensive rats with candesartan by using subcutaneously implanted osmotic minipumps (Nishimura et al., 2000a). In their study, 0.5-mg/kg can-desartan per day was given for 3 to 14 days before animals were subjected to 1 or 2 hours MCAO with reperfusion. This treatment significantly reduced infarct size, as determined at 24 hours after MCAO, by 58% and 64% compared with controls, respectively. This dose of candesartan sufficiently blocked angiotensin II binding to brain AT1 receptors (Nishimura et al., 1998). Most interestingly, candesartan inhibited binding of angiotensin to AT1 receptors to the same extent in brain areas outside and inside the blood—brain barrier, indicating that candesartan readily penetrates the blood—brain barrier (Nishimura et al., 2000b). Using this previous study as a reference, the same candesartan dose of 0.5 mg/kg was used in the present study. Effects of this dose of candesartan on other receptors appear unlikely because candesartan is more than 105 times more selective in binding to AT1 receptors than to AT2 receptors or to other receptors (Shibouta et al., 1993).
Although the present study confirms those findings on infarct size measured at 7 days after MCA occlusion, loss in body weight and neurologic outcome were also determined. Interestingly, the average loss in body weight and the neurologic score of animals undergoing candesartan pretreatment were not different from controls, though there was a tendency towards a lower (better) neurologic score (1.55 ± 0.18 vs. 1.80 ± 0.13, P = 0.10).
Interestingly, infarct size in animals undergoing candesartan pretreatment measured at 1.5 hours after MCAO (part II) compared with 7 days after MCAO (part I) was somewhat different (36 ± 10 mm3 vs. 60 ± 10 mm3, respectively). Li and colleagues determined infarct size after a short period of MCAO (0.5 hours) followed by reperfusion (Li et al., 2000) by using noninvasive repetitive measurements with diffusion-weighted magnetic resonance imaging. They found that infarct size maximized at 48 hours reperfusion. Thus, reperfusion injury contributes to the definite infarct size.
The results on neurologic outcome in the present study are in contrast to previously published data by Dai et al. (1999). In their study, the AT1-receptor blocker irbesartan was infused intracerebroventricularly over a 5-day period before 90 minutes of MCA occlusion with reperfusion. Using a three-point grading scale to determine neurologic outcome, the authors reported a significantly improved neurologic score at 24 hours after MCA occlusion in animals undergoing irbesartan treatment compared with controls (1.33 vs. 1.93, P < 0.05). Aside from the different, less differentiating neurologic score system, a possible explanation for the discordance might relate to the duration of reperfusion. Dai et al. obtained the score at 24 hours after MCA occlusion, whereas in the present study the neurologic outcome was determined at 7 days after MCA occlusion. Such reduced benefit in neurologic outcome suggests that the beneficial effect of AT1-receptor blocker pretreatment on neurologic outcome after vessel occlusion may vanish over time.
In the present study, candesartan had no significant effect on blood pressure in either the acute or chronic phase of cerebral ischemia. These results are in line with other studies, in which the protective effect of angiotensin-converting enzyme inhibitors and AT1-receptor blockers was also achieved with doses that had no or only little effect on blood pressure (Inada et al., 1997;Sadoshima et al., 1993;Stier et al., 1993;von Lutterotti et al., 1992).
By using radiolabeled microspheres, we showed that the absolute CBF was significantly higher in the infarcted hemisphere of candesartan-pretreated rats immediately before and at 30 minutes after MCA occlusion compared with controls. In addition, we used LDF to noninvasively monitor relative CBF in the MCA-supplied cortex and to ensure proper reperfusion. Since Dirnagel et al. (1989) reported that LDF could be used to provide accurate measurements of relative CBF in focal cerebral ischemia and reperfusion, many studies have used this method to monitor cortical CBF (Dorfler et al., 1997;Morikawa et al., 1992). In the present study, relative CBF in candesartan pretreated animals at 60 minutes after MCA occlusion was 20% higher than in controls. Both the microsphere and LDF data imply that the benefit of candesartan treatment starting before the onset of cerebral ischemia is due in part to an increase of CBF in the acute phase of ischemia.
In the recently published ACCESS study, Schrader et al. (2003) examined the effect of modest blood pressure reduction produced by candesartan in stroke patients. Candesartan was applied daily starting at the first day after the onset of vessel occlusion. The cumulative 12-month mortality and the number of vascular events were significantly lower in the candesartan group than in controls.
In agreement with these clinical findings, we showed that single and chronic candesartan treatment starting at 24 hours after MCA occlusion still results in a significant reduction of infarct size and improved neurologic outcome. Single AT1-receptor blocker administration at 24 hours after MCAO still resulted in a reduction of infarct size by 29%, whereas continuous treatment for 7 days reduced infarct size by 64%. The benefit of AT1-receptor blockade when applied after ischemia cannot be explained by an increase in blood flow to the ischemic area, because any benefit of increased blood flow during reperfusion in the used rat suture model is limited to a time frame of approximately 2 or 3 hours after MCAO (Kaplan et al., 1991;Lin et al., 1993). Although reduction in infarct size after single candesartan posttreatment was not significantly smaller than with single pretreatment, neurologic score and body weight at day 7 after MCA occlusion were significantly better preserved.
One possible mechanism by which the AT1-receptor blocker might reduce infarct size in the reperfusion phase after cerebral ischemia is through inhibition of inducible nitric oxide synthase (iNOS) expression. Nitric oxide produced by iNOS is one of the factors contributing to the expansion of brain damage in the late postischemic period. Expression of iNOS starts between 24 and 48 hours and peaks at 96 hours after transient or permanent vessel occlusion (Iadecola et al., 1997;Nagayama et al., 1998). Zhang et al. (1996) studied the effect of the iNOS inhibitor aminoguanidine on infarct size in the rat suture model. Aminoguanidine, when administered 24 hours after a 2-hour MCA occlusion with reperfusion, resulted in a reduction of infarct size by 26%. Even with permanent MCA occlusion, iNOS-inhibitor treatment starting at 18 hours after MCA occlusion still resulted in a reduction of infarct size by 31% (Parmentier et al., 1999).
Several lines of evidence indicate that AT1 receptor blockade can interfere with the induction of iNOS. (1) In cultured vascular smooth muscle cells, tumor necrosis factor-α increases nitric oxide production through the expression of iNOS. An AT1-receptor blocker can block such tumor necrosis factor-α–induced NO production (Nakayama et al., 1994). (2) In stroke-prone spontaneously hypertensive rats, early mortality of untreated controls is reduced by treatment with candesartan (Bennai et al., 1999). In these animals, the expression of iNOS is largely reduced compared with controls, and this effect is more pronounced in brain than in kidney. (3) AT1-receptor blockade decreases the iNOS expression in rat astroglial cultures (Chandler et al., 1995). (4) Candesartan, at doses that do not affect blood pressure, reduces iNOS expression in failing hearts of Dahl salt-sensitive hypertensive rats fed a high-salt diet (Kobayashi et al., 2001). Myocardial remodeling and left ventricular dysfunction were significantly attenuated by candesartan.
Apart from reduced iNOS expression, AT1-receptor blockade improves stroke outcome by stimulation of neuronal regeneration by AT2 receptors (Unger et al., 2001). Similarly, AT2-receptor activation secondary to AT1-receptor blockade was responsible for myocardial infarct size reduction in pigs (Jalowy et al., 1998).
Thus, reduced iNOS expression and increased AT2-receptor stimulation after candesartan treatment may contribute to reduced infarct size and improved neurologic outcome after MCAO. It should be the goal of further studies to measure iNOS expression and to assess the importance of AT2-receptor stimulation for such improved outcome.