
Abstract
The effect of a nonpeptide CC chemokine receptor antagonist, TAK-779, on ischemic brain injury resulting from 1-hour middle cerebral artery occlusion followed by 48-hour reperfusion was examined in ddY mice. On intracerebroventricular injection of vehicle or TAK-779, infarct volume in the vehicle-treated group was 44.2 ± 13.2% of the contralateral hemispheric volume, and TAK-779 (25 and 250 ng/mouse) dose-dependently reduced the infarct volume to 35.0 ± 12.2% and 31.1 ± 12.9%, respectively. On intravenous injection, infarct volume in the vehicle-treated group was 32.0 ± 16.1%, and TAK-779 (5 μg per 20 g body weight) significantly reduced this to 22.0 ± 10.5%. The results showed for the first time that a nonpeptide chemokine receptor antagonist is protective against ischemic brain injury.
Chemokines are a group of cytokines having chemotactic activity for leukocytes, and divided into four subfamilies: CXC, CC, C and CX3C (Mackay, 2001; Zlotnik and Yoshie, 2000). Although their expressions and functions were originally described in relation to inflammatory and allergic responses in peripheral organs (Feng et al., 1995; Frevert et al., 1995; Barker et al., 1990), they have been recently shown to be expressed in the brain under various pathologic conditions including multiple sclerosis, Alzheimer disease, and AIDS dementia (Asensio and Campbell, 1999), indicating important roles in these diseases. In addition, mRNA of various chemokines such as macrophage inflammatory protein-1α (MIP-1α), monocyte chemoattractant protein-1, and cytokine-induced neutrophil chemoattractant-1 has been detected in ischemic brain (Takami et al., 1997; Wang et al., 1995; Kim et al., 1995; Liu et al., 1993). Furthermore, we recently reported that intracerebroventricular administration of a chemokine receptor antagonist peptide, viral macrophage inflammatory protein-II (vMIP-II), protected the brain against transient focal cerebral ischemia (Takami et al., 2001). These findings suggest that chemokines play a crucial role in ischemic brain injury, and that their receptors are potential targets for therapeutic intervention in stroke. In this context, it is interesting to examine whether nonpeptide chemokine antagonists exert a neuroprotective effect. TAK-779 (Fig. 1) is a small-molecule, nonpeptide compound that selectively binds to a certain subtype of the CC chemokine receptor, CCR5, with high affinity (Baba et al., 1999). It also binds to the CCR2 subtype, but with about 20-fold lower affinity. In the present study, the protective effects of centrally or systemically administered TAK-779 on ischemic brain were examined using a middle cerebral artery (MCA) occlusion model in mice.
Chemical structure of TAK-779, N,N-dimethyl-N-[4-[[[2-(4-methylphenyl)-6,7-dihydro-5 H-benzocyclohepten-8-yl]carbonyl]amino]benzyl]tetrahydro-2 H-pyran-4-aminium chloride.
MATERIALS AND METHODS
Male ddY mice (4 weeks old; Japan SLC, Inc., Hamamatsu, Japan) were housed under diurnal lighting and allowed food and water ad libitum. The surgery for focal cerebral ischemia was conducted as previously described (Takami et al., 2001). Briefly, animals were anesthetized with 1.5% halothane for induction and maintained with 1.0% halothane in 70% N2O/30% O2. Rectal temperature during the surgical procedure was kept at 37°C with a thermostatically controlled heating pad (NS-TC; Neuroscience Inc., Tokyo, Japan), and temporal muscle temperature was measured using a needle probe (BAT-12; Physitemp Instruments, Inc., Clifton, NJ, U.S.A.). The MCA was occluded with an 8.0 nylon monofilament (11-mm length) coated with a mixture of silicone resin and hardener. After ligation of the common carotid artery and external carotid artery, the filament was introduced into the left internal carotid artery through the incision at the external carotid artery, and pushed up to the anterior cerebral artery to occlude the MCA. After 1 hour of occlusion, the filament was withdrawn and the external carotid artery was coagulated with bipolar forceps, then the common carotid artery was released from ligation. In each animal, regional cerebral blood flow at the ischemic core was monitored by laser-Doppler flowmetry (FLO-C1; Omegawave, Tokyo, Japan), and the animals in which the blood flow was reduced to less than 25% by occlusion and recovered to more than 65% by reperfusion were used for further evaluations. Mice were kept in a warming chamber (Thermocare, Incline Village, NV, U.S.A.) for 3 hours after surgery. Animal experiments were performed in accordance with the National Cardiovascular Center's guidelines for animal care and experiments.
TAK-779 was kindly provided by Takeda Chemical Industries, Ltd. (Osaka, Japan). It was dissolved in dimethyl sulfoxide at 5 mg/mL and diluted with phosphate-buffered saline (PBS) to a given concentration at use. TAK-779 (25 or 250 ng in 5 μL) was administered by intracerebroventricular injection (1.0 mm lateral, 0.5 mm posterior, 3.0 mm ventral to bregma) at 10 minutes before MCA occlusion, or by intravenous injection (5 μg/100 μL per 20 g body weight) in the left femoral vein at 10 minutes before reperfusion. Vehicle-treated mice were injected with 1% dimethyl sulfoxide in PBS.
Forty-eight hours after reperfusion, the animals were killed by transcardial perfusion with 10% formalin in 0.1 mol/L PBS (pH 7.4) under anesthesia by intraperitoneal injection of sodium pentobarbital (100 mg/kg). The brains were removed quickly and kept in 10% formalin/0.1 mol/L PBS for 24 hours. After incubation in PBS containing 20% sucrose for 12 hours, the brains were cut into coronal sections 50-μm thick at an interval of 500 μm throughout the cerebrum (from bregma 3.2 mm to bregma −3.8 mm) (Franklin and Paxinos, 1997). The sections were mounted onto gelatin-coated glass slides, and stained with hematoxylin and eosin. The infarct area of each section was measured using the Olympus Image Analysis System (Olympus Optical Co., Ltd., Tokyo, Japan) and integrated to give the infarct volume. Infarct volume was presented as a percentage of the contralateral hemispheric volume, and data are presented as mean ± SD. Infarct volumes in the experiments using intracerebroventricular injection were analyzed by one-way analysis of variance (ANOVA) followed by Bonferroni's post hoc test. Infarct volumes in the experiments using intravenous injection were analyzed by Student's t-test.
Leukocytic infiltration was examined by immunohistochemical analyses. Five animals were selected at random from each group intravenously injected with TAK-779 or vehicle, and the brain section (50-μm thick) at bregma −0.3 to −0.8 mm from each animal was used for immunostaining. Rabbit anti-mouse myeloperoxidase antibody (DAKO Japan Ltd., Kyoto, Japan) and rat anti-mouse Mac-1α antibody (Chemicon International, Inc., Temecula, CA, U.S.A.) were used as primary antibodies to stain neutrophils and activated macrophages/microglia, respectively. The sections were incubated with each primary antibody for 15 to 16 hours at 4°C, and the primary antibody was visualized using a Vectastain ABC elite kit (Vector Laboratories, Inc., Burlingame, CA, U.S.A.) with 0.02% 3,3′-diaminobenzidine tetrahydrochloride/0.003% H2O2. The number of myeloperoxidase-or Mac-1α–positive cells in an area of 500 × 500 μm2 was counted in the dorsomedial region of the striatum, the region where the ischemic penumbra was constantly observed.
RESULTS
First, the effect of an intracerebroventricular administration of TAK-779 on brain infarction was examined (Fig. 2A). In the vehicle-injected group, the infarct volume was 44.2 ± 13.2% of the contralateral hemispheric volume. Intracerebroventricular injection of TAK-779 at 25 ng decreased this to 35.0 ± 12.2%, but the change was not significant. The injection of 250 ng of TAK-779 significantly decreased the infarct volume to 31.1 ± 12.9%. There were no significant differences in the temporal muscle and rectal temperatures between the groups. In the vehicle-, TAK-779 (25 ng)-, and TAK-779 (250 ng)–injected groups, the temporal muscle temperatures were 35.9 ± 0.7°C, 36.1 ± 0.9°C, and 36.1 ± 0.8°C at the start of surgery, and 36.0 ± 0.4°C, 36.2 ± 0.9°C, and 36.2 ± 0.7°C at the end of surgery, respectively. The rectal temperatures were 37.0 ± 0.4°C, 37.1 ± 0.2°C, and 36.9 ± 0.7°C at the start of surgery, and 37.0 ± 0.4°C, 37.2 ± 0.2°C, and 36.9 ± 0.7°C at the end of surgery, respectively. In five animals from each group injected with vehicle or 250 ng of TAK-779, the rectal temperatures were monitored 1, 2, and 3 hours after reperfusion. The temperatures were 37.5 ± 0.3°C, 36.8 ± 1.3°C, and 37.4 ± 1.6°C in the vehicle-injected group, and 37.2 ± 0.4°C, 36.7 ± 1.2°C, and 35.9 ± 1.1°C in the TAK-779–injected group.
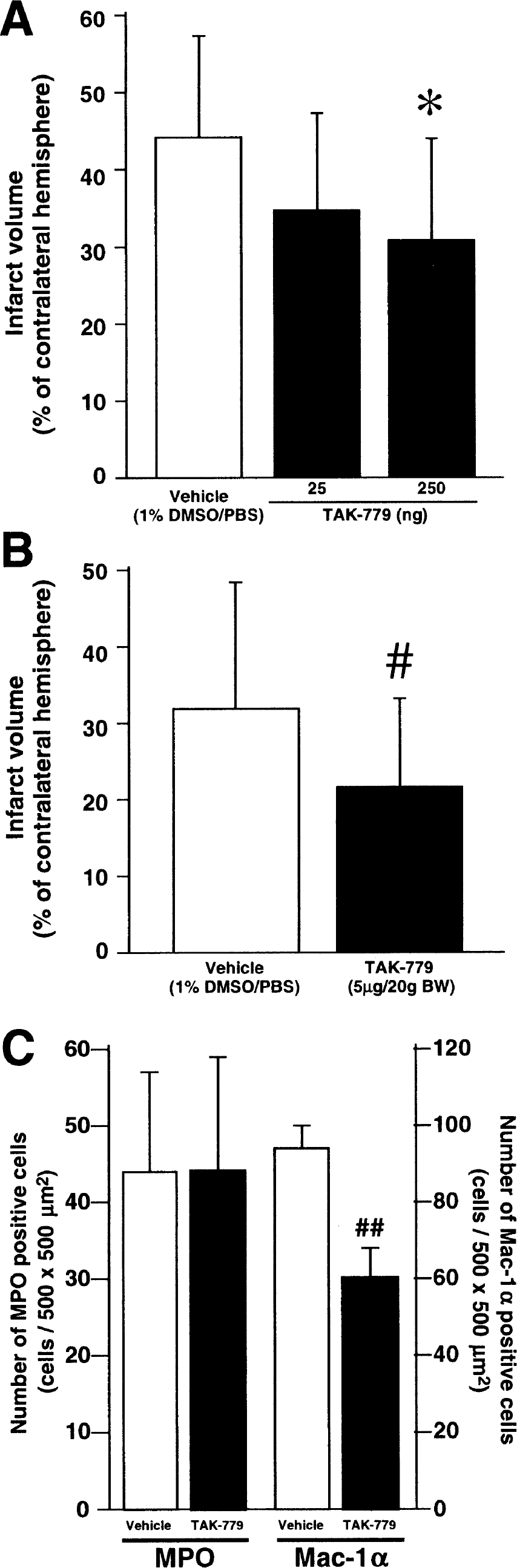
Second, the effect of an intravenous administration of TAK-779 was examined (Fig. 2B). In the vehicle-injected group, the infarct volume was 32.0 ± 16.1% of the contralateral hemispheric volume. Intravenous injection of TAK-779 at a dose of 5 μg/20 g body weight significantly decreased this value to 22.0 ± 10.5%. There were no significant differences in the temporal muscle and rectal temperatures between the groups. In the vehicle-and TAK-779–injected groups, the temporal muscle temperatures were 36.2 ± 0.8°C and 36.0 ± 0.9°C at the start of surgery, and 36.2 ± 0.8°C and 36.0 ± 1.0°C at the end of surgery, respectively. The rectal temperatures were 37.1 ± 0.6°C and 37.2 ± 0.3°C at the start of surgery, and 37.1 ± 0.6°C and 37.3 ± 0.4°C at the end of surgery, respectively. In five animals from each group injected with vehicle or TAK-779, the rectal temperatures were monitored 1, 2, and 3 hours after reperfusion. The temperatures were 37.3 ± 0.7°C, 36.6 ± 1.0°C, and 36.7 ± 1.3°C in the vehicle-injected group, and 37.0 ± 0.8°C, 36.9 ± 1.0°C, and 36.7 ± 1.0°C in the TAK-779–injected group.
Leukocytic infiltration was examined in intravenously injected mice at 48 hours after reperfusion. The brain sections were immunohistochemically investigated using antimyeloperoxidase (a marker for neutrophils) and anti—Mac-1α (a marker for activated macrophages/microglia) antibodies (Fig. 2C). There was no significant difference in the number of myeloperoxidase-positive cells between vehicle-and TAK-779 (5 μg/20 g body weight)–injected groups. The numbers were 43.8 ± 12.8 and 44.0 ± 14.6 cells in an area 500 × 500 μm2, respectively. On the other hand, the number of Mac-1α–positive cells was significantly decreased by the treatment with TAK-779. The numbers were 94.2 ± 6.1 and 60.8 ± 6.8 cells in an area 500 × 500 μm2 in the vehicle-and TAK-779–injected groups, respectively.
DISCUSSION
We previously reported that the intracerebroventricular administration of a broad-spectrum chemokine receptor antagonist, vMIP-II, protected the brain against ischemic injury induced by MCA occlusion, suggesting that chemokines and their receptors expressed in the brain play a crucial role in ischemic injury (Takami et al., 2001). The present study showed a protective effect of intracerebroventricularly administered TAK-779 under the same ischemic condition. This result suggests the involvement of CCR5 and/or CCR2 chemokine receptors in ischemic brain injury, because TAK-779 selectively binds CCR5 chemokine receptors, having a 20-fold lower affinity for CCR2 receptors (Baba et al., 1999). This idea is supported by the findings that the expression of mRNA for MIP-1α (an endogenous agonist for CCR1 and CCR5) and monocyte chemoattractant protein-1 (that for CCR2) is induced in the ischemic brain (Takami et al., 1997; Wang et al., 1995; Kim et al., 1995). Furthermore, it has been reported that excitotoxic injury induces expression of CCR5 (Galasso et al., 1998) and CCR2 (Galasso et al., 2000) receptors in the neonatal rat brain.
The site at which intravenously administered TAK-779 acts to produce a protective effect remains to be elucidated. It has been reported that intravenous administration of a broad-spectrum chemokine receptor antagonist peptide (Beech et al., 2001) or an antibody against interleukin-8 (Matsumoto et al., 1997) or cytokine-induced neutrophil chemoattractant (Yamasaki et al., 1997) attenuated brain infarction resulting from focal cerebral ischemia. These findings suggest that peripheral chemokines and their receptors could be targets for the protective effects on ischemic brain, because peptides or macromolecules such as antibodies are usually unable to pass through the blood—brain barrier. Alternatively, it is possible that a dysfunction of the blood—brain barrier due to ischemia enables these antichemokine drugs to pass through. It has been reported that transient brain ischemia damages the blood—brain barrier to allow serum macromolecules such as albumin and immunoglobulin to extravasate into the brain parenchyma (Nishino, et al., 1994). Under such a pathophysiologic condition, intravenously administered TAK-779 may enter the brain parenchyma to act on the chemokine receptors expressed in neuronal and/or glial cells.
Chemokines play crucial roles in the transendothelial migration of leukocytes such as neutrophils, monocytes/macrophages, and lymphocytes (Mackay, 2001). In the present study, intravenous injection of TAK-779 decreased the number of activated macrophages/microglia, but not that of neutrophils, in the ischemic penumbra. These results can be explained by the subtype selectivity of TAK-779 and the receptor subtypes expressed in macrophages/microglia and neutrophils. Namely, TAK-779 is a selective antagonist for CCR5 and CCR2 receptors, and macrophages/microglia express these two receptors plus CCR1 and CX3CR receptors for the regulation of migration and/or activation (Luster, 1998). In contrast, neutrophils express CXCR2 receptors, but not CCR5 and CCR2 receptors.
In this study, we demonstrated that the intracerebroventricular or intravenous administration of a chemokine antagonist TAK-779, which is selective for CCR5 and CCR2 chemokine receptors, attenuated brain infarction after transient focal cerebral ischemia. This is the first evidence that a nonpeptide chemokine receptor antagonist has a protective effect on ischemic brain. Nonpeptide chemokine receptor antagonists have been shown to be potential candidates for drugs to treat stroke.