
Abstract
Measurement of global cerebral blood flow (CBF) using extracranial duplex sonography has been described, but normal values are still lacking. In 85 healthy adults (median age 43.4 years, range 20 to 80 years), CBF was determined by duplex sonographic examination of both internal carotid arteries and vertebral arteries. The mean global CBF was 630 ± 97 mL/min. Global CBF declined with age; sex did not influence the total CBF. When measurements were repeated, the intraindividual variability was low. This noninvasive sonographic measurement of CBF is reproducible, and values correspond closely to those obtained with positron emission tomography and magnetic resonance imaging.
Measurement of cerebral blood flow (CBF) volume is required in clinical neurology for the identification and quantification of focal or generalized perfusion disturbances in the course of cerebrovascular, traumatic, or neurodegenerative disorders. For the quantitative assessment of brain perfusion, nuclear medical techniques have been used up to now. These methods expose patients to radiation and are expensive and not widely available. Ultrasound techniques have advanced the noninvasive diagnosis of cerebrovascular diseases.
Recently, several groups have reported the measurement of CBF by ultrasound (Donis et al., 1988; Keller et al., 1976; Müller et al., 1987; Uematsu et al., 1983). Their research evaluated the flow volume of the common carotid artery (CCA) because of its ease of performance. These methods, however, may be less precise than separate measurements of the internal carotid (ICA) and external carotid (ECA) arteries (Schöning et al., 1994). The CCA vessel diameter substantially changes during a cardiac cycle, and it has been shown that the mean flow volume can be higher in the CCA than the sum of the flow volumes in the ICA and ECA (Donis et al., 1988; Schöning et al., 1994). In contrast, it has been reported that calculation of CBF by summing up the flow volumes of both the ICA and the vertebral artery (VA) is precise and reliable (Schöning et al., 1994). Age-adjusted normal values of this sonographic CBF measurement are still lacking. Therefore, we set out to reproduce findings reported earlier by the use of different techniques and to determine total CBF by the sonographic examination of the ICA and VA in different age groups of healthy volunteers.
SUBJECTS AND METHODS
Eighty-five healthy volunteers (46 women, 39 men) were enrolled in a prospective study. At least 10 subjects for each age decade were included (median age 43.5 years, range 20 to 80 years). None of the subjects had a history of cerebrovascular disorders or any neurological diseases or deficits, and none of them suffered from heart failure. Arteriosclerotic plaques or stenosis at the site of measurement were excluded by B-mode imaging. Cerebral blood flow measurements were performed according to the protocol proposed by Schöning et al. (1994). Sonographic examination was performed with a 5-MHz linear transducer of a color-coded ultrasound system (Sonoline Elegra; Siemens, Erlangen, Germany). The volunteers rested in a supine position with the head slightly tilted upward for at least 5 minutes before the first examination. The two-dimensional longitudinal vessel sections were depicted. Site of measurement of the ICA was 1.5 cm distal to the bifurcation to ascertain a circular lumen. The VA was examined in the V2 segment between the transverse processes of the vertebrae C4 and C5. Doppler recording was done using a Doppler frequency of 4.0 MHz and a sample volume covering the entire width of the vessel. Up to 4.0 mm, a sample volume size could be increased in steps of 0.5 mm. For larger vessel diameters, sample volumes of 5.0 and 7.5 mm could be selected. Special attention was given to ensure that no turbulent flow was identified at the site of Doppler recordings and that the angle of insonation was below 60°. Minimal vessel length required to perform a reliable angle correction was 2.0 cm. The blood flow volume (Q) of each artery was calculated from the time-averaged velocity (TAV) and the cross-sectional area (A) of the vessel (Q = TAV × A). Time-averaged velocities were measured over a minimum of three cardiac cycles, when the signal was stable. The cross-sectional area (A) was calculated from the inner vessel diameter (d) using the formula A = (d/2)2 · π. Total CBF was determined as the sum of flow volumes of the ICA and VA of both sides. The measurement was repeated 30 minutes later by the same examiner.
RESULTS
In 84 volunteers, the ICA and VA of both sides could be examined by color-coded duplex sonography. One volunteer had to be excluded because the bifurcation on both sides was localized high in the neck. Mean duration of the examination was ∼15 to 20 minutes.
The global CBF and the flow volumes of the ICA and VA (mean ± SD) of each age group are given in Table 1. The mean ± SD of total CBF of all subjects was 630 ± 97 mL/min, corresponding to 48.5 mL/100 g/min, assuming a brain weight of 1,300 g (Ho et al., 1980). There was a significant age-related decline (Spearman's rank correlation, r = −0.35, P < 0.001), as shown in Fig. 1. Mean total CBF ranged from 668 ± 84 mL/min in young adults (20 to 30 years) to 567 ± 125 mL/min in elderly people (71 to 80 years). Sex had no influence on total CBF.
Global cerebral blood flow volumes and blood flow volumes of the internal carotid and vertebral arteries for several age-groups in milliliters per minute (mean ± SD)
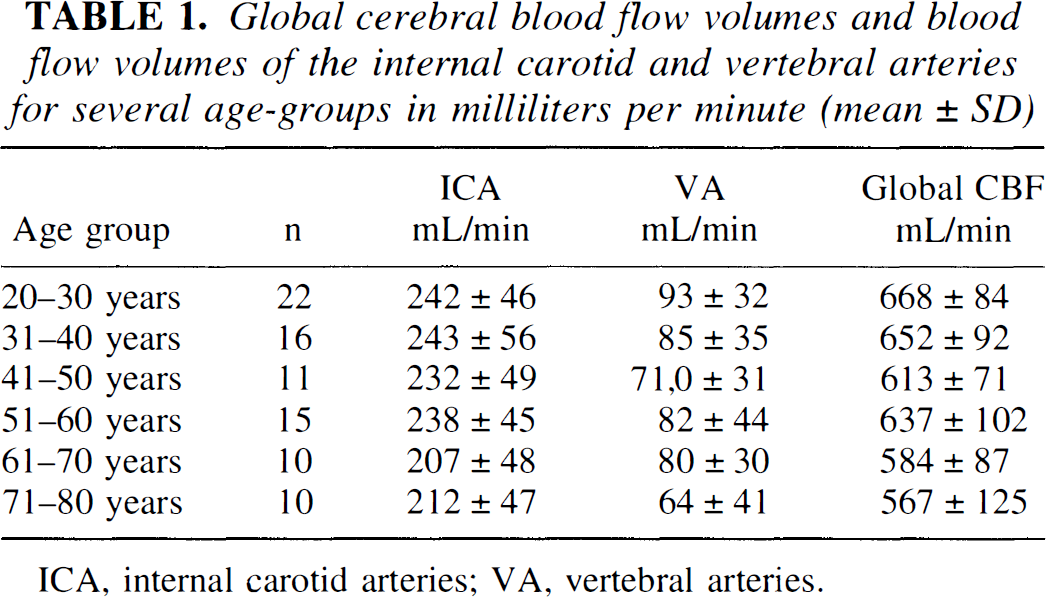
ICA, internal carotid arteries; VA, vertebral arteries.
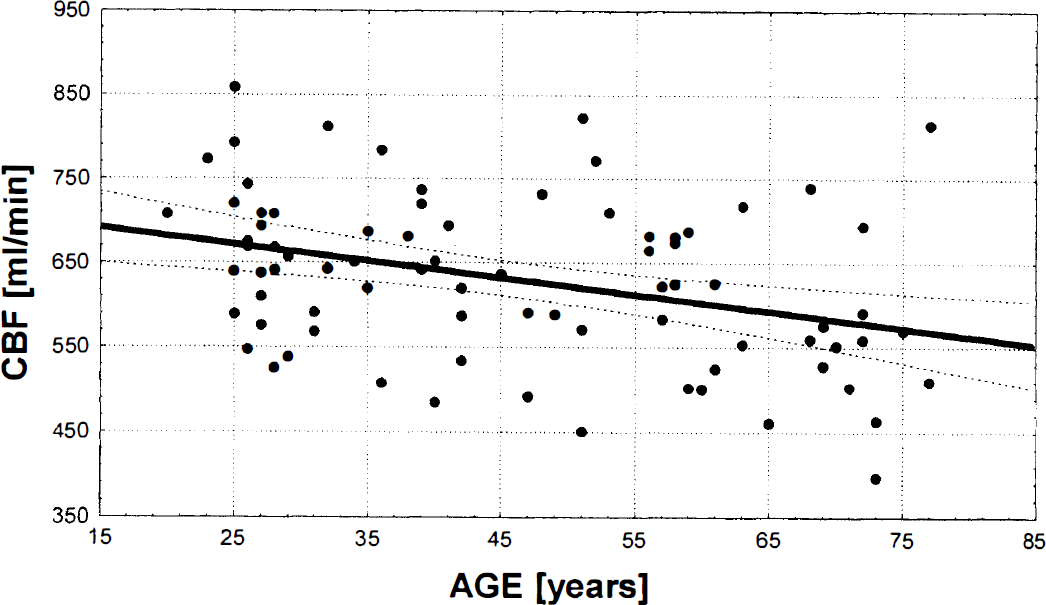
Age-dependent decline of total cerebral blood flow (Spearman's rank correlation, r = 0.35) in 84 healthy volunteers.
Side-to-side differences of the ICA flow volumes ranged from 0 to 53.2% (median 13.4%) and for the VA from 0 to 94.9% (median 34.4%). Higher side-to-side differences in VA flow volumes reflect that asymmetry is more frequent for the VA than for the ICA. Vertebral artery hypoplasia was present in three of our subjects, assuming a threshold diameter of 2.0 mm (Delcker and Diener, 1992).
Reproducibility of measurement was high when performed by the same examiner 30 minutes later (Spearman's rank correlation, r = 0.87).
DISCUSSION
Our findings reproduce those reported by Schöning et al. (1994, 1996), who determined a mean total CBF of 701 ± 104 mL/min in a group of 48 subjects aged 20 to 63 years (mean 35 ± 12 years). In accordance with the initial description of Schöning and Scheel (1996), we found that sonographic CBF measurements are reproducible and that the intraobserver variability is quite low. Sonographic CBF values are well in the range of normal values obtained with other techniques. Many studies have been published using different techniques yielding varying normal values for global CBF in resting healthy adults, ranging from ∼35 to ∼75 mL/100 g/min (Lassen, 1985). The Kety-Schmidt technique was developed first to quantitate global average CBF by the nitrous oxide method. Cerebral blood flow was estimated to be 54 mL/100 g/min (Kety and Schmidt, 1945). A systematic error, however, might have led to an overestimation (Madsen et al., 1993). According to the results of these investigators, true average values of CBF in healthy young adults are very close to 46 mL/100 g/min. Matthew et al. (1993) carried out two consecutive measurements of resting CBF in 25 normal volunteers using H215O positron emission tomography. The CBF was determined to be 40.3 ± 6.4 mL/100 g/min for the first measurement and 39.3 ± 6.5 mL/100 g/min for the second measurement. Herscovitch et al. (1987) reported that average global CBF was significantly greater when measured with [11C]butanol (53 mL/100 g/min) than with H215O (44 mL/100 g/min), because the use of a diffusion-limited tracer such as H215O may lead to an underestimation. Lassen (1985) proposed that the total CBF in healthy adults is close to 50 mL/100 g/min and values out of the range of 45 to 55 mL/100 g/min are regarded to be an over- or underestimation of the “true” CBF. The CBF values reported in our study (48.5 mL/100 g/min) are very close to these reference values. In accordance with other groups, we found a significant age-related decline of CBF (Buijs et al., 1998; Leenders et al., 1990; Martin et al., 1991; Naritomi et al., 1979; Shirahata et al., 1985). We and other groups identified no sex differences in global CBF (Buijs et al., 1998; Melamed et al., 1980; Schöning et al., 1994; Shirahata et al., 1985). However, some authors reported higher total CBF levels in women (Daniel et al., 1989; Esposito et al., 1996; Rodriguez et al., 1988).
The limitations of sonographic CBF measurements should be mentioned: Although we found an excellent intraobserver reproducibility, the reliability of sonographic examination depends highly on the skills and the experience of the examiner. Sonographic CBF measurements cannot be performed in patients with a high carotid artery bifurcation, ICA plaques, or stenosis or in patients with an abnormal course of the ICA (kinking or tortuosity). In addition, Doppler recordings require a cooperative patient able to lie supine in an immobilized position for ∼20 minutes. Snoring and respiratory sounds interfere with Doppler recordings. Further studies will have to elucidate whether ultrasound CBF measurements are dependent on the ultrasound equipment and probe frequency.
In summary, color-coded duplex sonography provides a reliable method for the evaluation of CBF volume. Ultrasound is a widely available, cost-effective technique. Because of its mobility, bedside examination of a critically ill patient is feasible. The absence of biological side effects in diagnostic ultrasound allows repeated follow-up examinations without any risk for the patient. According to these data and findings reported by Schöning et al. (1994, 1996), we conclude that sonographic CBF measurements are reliable and may become a valuable completion of the sonographic workup in patients with cerebrovascular disorders.
Footnotes
Abbreviations used
Acknowledgements
The authors gratefully acknowledge Ilse Becker and Wayne Ellsworth for their continuous support and their help in the preparation of the manuscript.