
Abstract

Introduction:
VIPomas of the pancreas are very rare functional neuroendocrine tumors with a reported incidence of one person per 10 million people per year. 1 The autonomous secretion of vasoactive intestinal peptide (VIP) leads to a distinctive clinical syndrome of watery diarrhea, hypokalemia, and achlorhydria, referred to as the watery diarrhea, hypokalemia, and achlrohydria (WDHA) or Verner-Morrison syndrome. Diagnosis is confirmed with an elevated serum VIP level, and imaging is utilized for tumor localization. Approximately 60 to 80 percent of VIPoma patients have metastatic disease at initial presentation, often due to delayed diagnosis. 2 For nonmetastatic lesions of the pancreas, surgical resection remains the only potential cure. This video depicts laparoscopic distal pancreatectomy and splenectomy with cholecystectomy for an isolated VIPoma of the tail of the pancreas.
Materials and Methods:
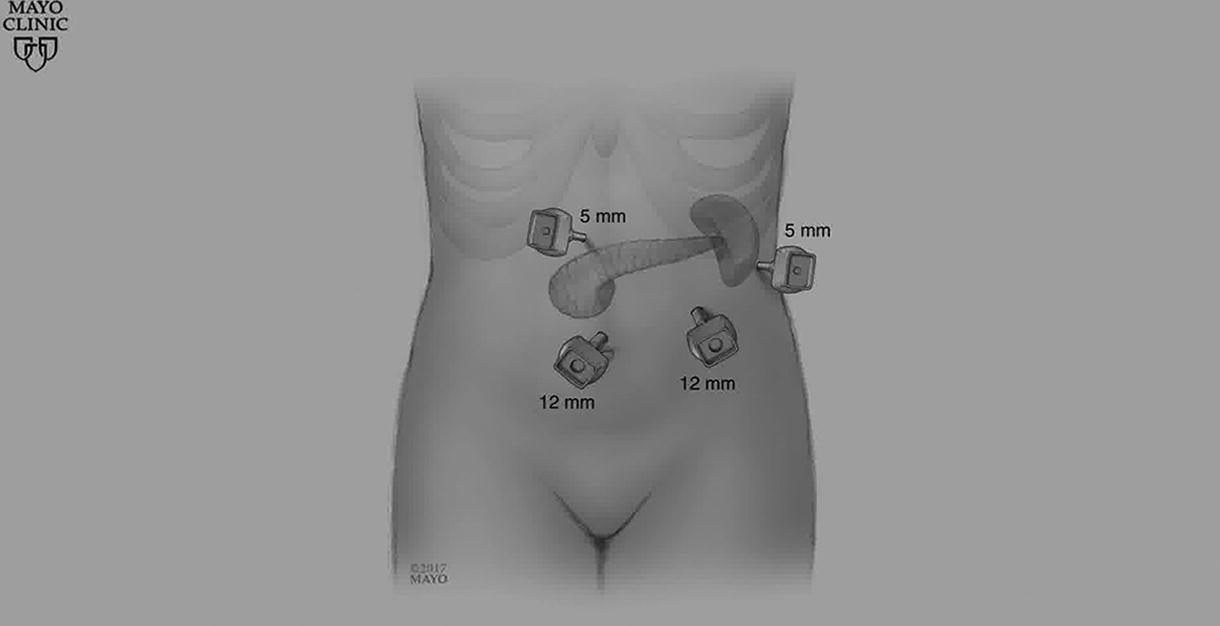
A 57-year-old female patient presented to the emergency department with worsening of a year-long intermittent diarrhea, nausea, vomiting, and an unintentional 4.5 kg weight loss. Initial laboratory findings revealed hypokalemia and anion gap metabolic acidosis. A CT scan of the abdomen and pelvis identified a pancreatic tail lesion, and an MRI showed no signs of pancreatic parenchymal atrophy or dilation of the main pancreatic duct. An endoscopic ultrasound-guided fine needle aspiration (EUS-FNA) biopsy of the lesion confirmed a well-differentiated neuroendocrine tumor. Neuroendocrine markers were obtained, including serum VIP, urine 5-HIAA, plasma chromogranin A, serum glucagon, serum gastrin, and serum somatostatin, and were significant for an elevated serum VIP level of 392 pg/mL (normal <75 pg/mL). A PET-CT with Gallium-68 dotatate showed intense tracer uptake by the pancreatic lesion. There was no evidence of metastatic disease on imaging, and a decision was made to proceed with surgery. Laparoscopic distal pancreatectomy was performed as per the caudad-to-cephalad clockwise technique with progressive stepwise compression and staple line reinforcement during pancreatic transection. 3 The splenic artery and vein were transected en bloc with the pancreatic parenchyma, and the spleen was removed. A prophylactic standard cholecystectomy concluded the operation.
Results:
The patient had an uneventful postoperative course and was discharged on postoperative day one. Surgical pathology confirmed a grade 2, well-differentiated neuroendocrine tumor measuring 4.5 cm. All 15 lymph nodes sampled were negative for metastasis, and all margins were clear. Immunohistochemistry showed a Ki-67 proliferative index of 4.9%, and the tumor was positive for synaptophysin, keratin, and VIP. Staining for chromogranin A, somatostatin, insulin, and glucagon were all negative. At 3 months’ follow-up, the patient’s serum VIP level normalized to below 50 pg/mL. She reported complete symptom relief, with no recurrence of diarrhea or unintentional weight loss, and she has started to gain weight. Ongoing surveillance, including MRI abdomen and CT chest at 6 months followed by every 12 months for 5 years, will continue to monitor for disease recurrence.
Conclusions:
Pancreatic VIPomas are very rare with the majority of patients presenting with metastases at the time of diagnosis. A high index of suspicion is needed to avoid delays in diagnosis. Surgical resection of localized lesions offers a potential cure, and the laparoscopic approach affords the benefits of minimally invasive surgery.
Patient Consent Statement:
The authors have received and archived patient consent for video recording/publication in advance of video recording of procedure.
Authors have no conflicts of interest to declare
.
Runtime of Video: 7 mins 41 secs
Get full access to this article
View all access options for this article.