
Abstract
Background/Aims:
Clinically relevant postoperative pancreatic fistula (CR-POPF) after distal pancreatectomy (DP) occurs in 20%–40% of patients and remains a leading cause of morbidity and increased healthcare cost in this patient group. Recently, several studies suggested decreased risk of CR-POPF with the use of peri-firing compression (PFC) technique. The aim of this report was to conduct a systematic review to get an overview of the current knowledge on the use of PFC in DP. In addition, our experience with PFC was presented.
Methods:
The systematic literature review was conducted according to the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) guidelines. Also, 19 patients undergoing DP with the use of PFC at Oslo University Hospital were studied. The primary endpoint was incidence of CR-POPF.
Results:
Seven articles reporting a total of 771 patients were ultimately included in the systematic review. Only two of these were case–control studies examining outcomes in patients with and without PFC, while the rest were case series. These were heterogeneous in terms of staplers used, cartridge selection policy, and PFC technique. Both case–control studies reported significantly reduced CR- POPF incidence with PFC. Eight (21%) of our patients developed CR-POPF after DP with PFC. Only one patient developed CR-POPF among those with pancreatic transection site thickness ⩽1.5 cm.
Conclusion:
Evidence on potential benefits of PFC in DP is limited in quantity and quality. Our findings suggest that the use of PFC does not lead to reduction in the incidence of CR-POPF. Yet, there might be a benefit from PFC when dealing with a thin pancreas.
Introduction
Despite perioperative advancements in pancreatic surgery, the incidence of clinically relevant postoperative pancreatic fistula (CR-POPF) following distal pancreatectomy (DP) has not significantly changed throughout the last decades ranging from 20% to 40%.1–4 CR-POPF is a well-known cause of postoperative morbidity, prolonged hospital stay, and increased healthcare costs. 5 Risk factors for CR-POPF have not been clearly defined in the literature, but both patient- and surgery-related factors seem to be important.1,2,6
Different preventive strategies have been proposed to decrease the incidence of CR-POPF following DP; however, there is no sound evidence in favor of or against any of these. 7 Randomized controlled trials (RCTs) have assessed various surgical techniques aiming to reduce the incidence of CR-POPF by investigating on pancreatic stump transection and closure methods. One of the recently suggested preventive methods is the use of prolonged peri-firing compression (PFC) at the pancreatic transection line prior to stapler firing and removal.8–10 Although comparative case–control studies reported significant reduction in CR-POPF with this method, it has not been validated in RCTs.
The aim of this study was to investigate the efficacy of PFC in prevention of CR-POPF after DP. To get an overview of the current knowledge on this topic, a systematic review of the literature was conducted. Furthermore, our experience based on prospective case-series with DP supplemented by PFC was presented.
Methods
Patients and study design
Patients undergoing DP for lesions in the body and tail of the pancreas at Oslo University Hospital, Rikshospitalet were included in this study. Procedures were performed via laparoscopic or open technique, either with or without spleen preservation. The exclusion criteria were patient age under 18 or over 90 years, American Society of Anesthesiologists (ASA) score ⩾ 5, procedures requiring bowel resections and/or anastomoses or stoma, acute necrotizing pancreatitis, immune suppression, pregnancy, and incapability of consent and contraindications for DP. Enrollment started on 1 February 2022, and all patients were followed-up for minimum 30 days after surgery. Data on patients undergoing DP with PFC were registered prospectively and maintained in the European consortium of Minimally Invasive Surgery (E-MIPS) registry. 11 The primary endpoint of this study was CR-POPF. Secondary endpoints were biochemical leak, postoperative complications, severe complications, postpancreatectomy hemorrhage, delayed gastric emptying, postoperative hospital stay, reoperation, and mortality. Written informed consent for data registration, collection, storage, and publication was obtained for all included patients. The consent form was approved by the local data protection officer at the hospital (21/14063) according to recommendations from the Regional Ethics Committee. Since PFC was a technique used prior to the initiated study in a non-standardized fashion, no specific ethical approval for this study was necessary.
Transection of the pancreas and PFC
Peripancreatic fatty tissue was dissected off the pancreas before the transection. Subsequently, the thickness of the pancreatic gland was measured at the transection site using intraoperative ultrasound. Based on the findings by Kondo et al., 12 ENDO-GIA black 60 mm cartridge was used for transection if the thickness exceeded 15 mm. If the transection site thickness was ⩽15 mm, ENDO-GIA purple 60 mm cartridge was applied. After placing the stapler, the transection site was manually compressed with the stapler intended to be used, for 3 and 2 min prior to and after firing, respectively. Addition of hemostatic agent or suture was at surgeon’s discretion when indicated to achieve hemostasis or an adequate pancreatic stump remnant.
Data and definitions
Data on patient demographics and perioperative characteristics were prospectively collected. The latter include body mass index (BMI), ASA score, comorbidities, previous abdominal surgery, neoadjuvant chemotherapy, diagnosis and location of lesion, type of approach and procedure, conversion, pancreatic texture, pancreatic duct diameter, pancreatic thickness at transection site, type of cartridge used, additional stump coverage used, operative time, estimated blood loss, postoperative complications, severe complications, reoperation, CR-POPF, postpancreatectomy hemorrhage, delayed gastric emptying, chyle leak, readmission, and length of stay.
CR-POPF was defined according to the 2016 update from the International Study Group of Pancreatic Surgery (ISGPS). 5 Conversion was defined as laparotomy during laparoscopic procedure not related to the specimen extraction. Postoperative complications were defined and graded according to the Clavien Dindo classification. 13 Grade ⩾IIIa complications were defined as severe. Delayed gastric emptying, postpancreatectomy hemorrhage, and chyle leak were defined and classified as suggested by the ISGPS.14,15 The 90 days from surgery definition was used for mortality and readmission. 16
Study selection strategy and data extraction
All the steps of systematic review were performed in accordance with the Cochrane handbook and Preferred Reporting Items for Systemic Reviews and Meta-Analyses (PRISMA).17,18 In January 2023, electronic databases such as PubMed, Cochrane CENTRAL, Scopus, Embase, and Web of Science were searched using the following query: “(Distal pancreatectomy OR Left pancreatectomy OR Pancreas resection OR Pancreatic resection) AND (Compression).” No language or year restrictions were used. The titles, abstracts, and full articles, if necessary, were screened for all citations retrieved from the searches and checked for eligibility. Studies that seemed to fulfill the eligibility criteria and those for which information in the abstract was not sufficient for exclusion were read in full. The bibliography of eligible studies was searched for any relevant articles. In case of studies with overlapping cohorts, those with the largest number of patients were included in this review.
The following data were extracted: study year, number of patients who received PFC during DP (cases), number of patients who did not receive PFC (controls), specific details on PFC (duration before and after firing), type of staplers and cartridges used, cartridge selection policy at the corresponding institution, and the incidence of CR-POPF. If a study reported the incidence of all types of pancreatic fistula, only grade B and C fistulae were included.
Statistics
Categorical data were presented as percentages and were compared using chi-square or Fisher’s exact tests. Continuous data were presented as mean values and standard deviations (SDs) or medians and interquartile ranges (IQRs) as appropriate. Two-sample Student’s t-test and Man–Whitney U-test were used to compare between-group differences for normally and non-normally distributed continuous data, respectively. Two-tailed p < 0.05 was considered statistically significant.
Results
Systematic review and analysis of studies
A total of 280 studies were identified after performing paper selection in accordance with PRISMA method (Fig. 1). Of these, 269 were excluded as they did not meet the inclusion criteria after reviewing the title or the abstract. Of the remaining 11 articles, 4 were discarded due to population overlapping or lack of relevance.
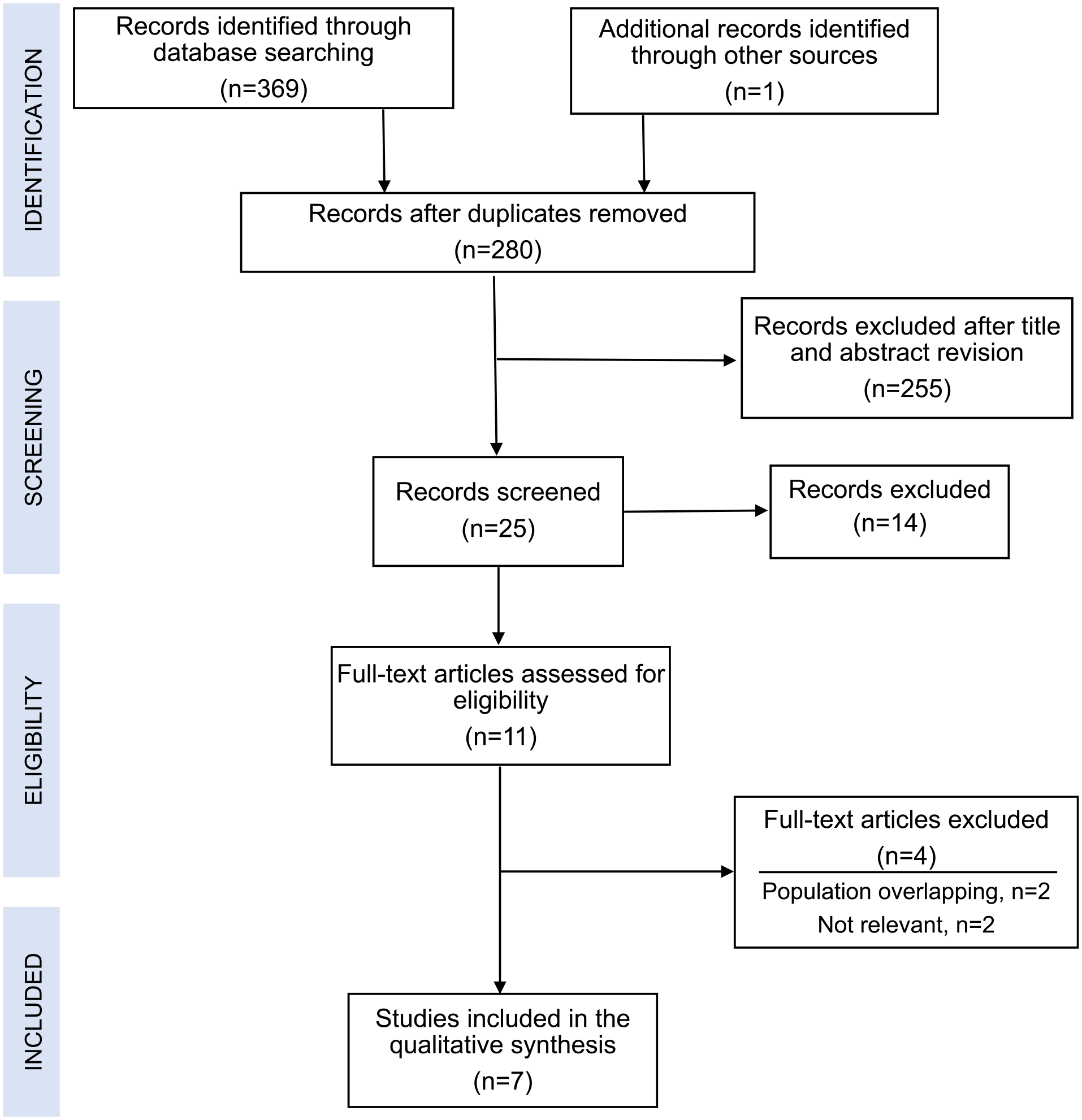
Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) diagram demonstrating selection of articles for review.
Seven articles reporting a total of 771 patients were ultimately included in this review (Table 1). Two of these were case–control studies examining outcomes in patients with and without PFC.9,10 Both reported significantly reduced CR-POPF incidence after PFC. In the meantime, compression techniques and its duration were different in these studies. Five studies reported case series with DP, where PFC was used routinely.8,19–22 The choice of staplers, cartridges, as well as PFC technique or duration, was different from study to study. Furthermore, the choice of staplers and cartridges was standard in some centers,19,21 while in the others, it was based upon surgeon’s judgment on pancreatic texture, closed length of the stapler, or possible presence of the splenic vessels in the stapling line.8,20,22 The rate of CR-POPF ranged from 0% to 22.6%, while various factors such as BMI, pancreatic parenchyma thickness, and compression ratio were found to be associated with CR-POPF. Aoki and co-workers compared the outcomes in patients with PFC and those with PFC supplemented by continuous suture of the pancreatic stump. 21 They reported 33% CR-POPF after DP with PFC but no such cases after PFC with continuous suture.
Review on literature discussing outcomes following distal pancreatectomy with peri-firing compression at the pancreatic transection site.
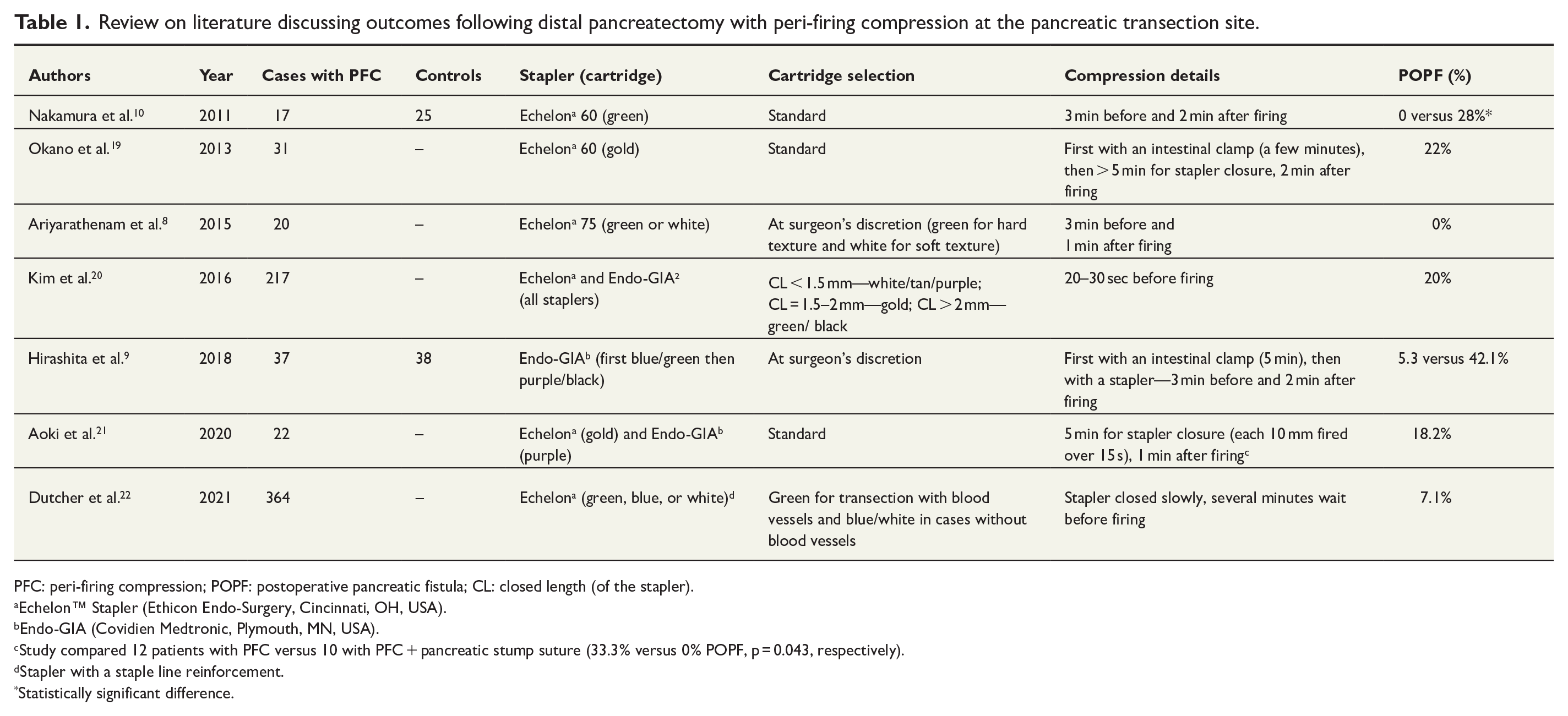
PFC: peri-firing compression; POPF: postoperative pancreatic fistula; CL: closed length (of the stapler).
Echelon™ Stapler (Ethicon Endo-Surgery, Cincinnati, OH, USA).
Endo-GIA (Covidien Medtronic, Plymouth, MN, USA).
Study compared 12 patients with PFC versus 10 with PFC + pancreatic stump suture (33.3% versus 0% POPF, p = 0.043, respectively).
Stapler with a staple line reinforcement.
Statistically significant difference.
Prospective case-series
Nineteen patients underwent DP with PFC at our institution. Demographics and patient characteristics are presented in Table 2. The most common indication for surgery was pancreatic neuroendocrine neoplasms (36.8%). Lesions were mostly located in the pancreatic tail and in the pancreatic neck/body region (36.8% each). All procedures except one were performed laparoscopically without preserving the spleen (Table 3). One patient required conversion (5.2%). Mean operative time was 207 (80) min, and median blood loss was 100 mL. Eight patients (21%) developed CR-POPF after surgery (Table 4). Median hospital stay was 4 days.
Demographics and preoperative characteristics in patients undergoing distal pancreatectomy with peri-firing compression at the pancreatic transection site.
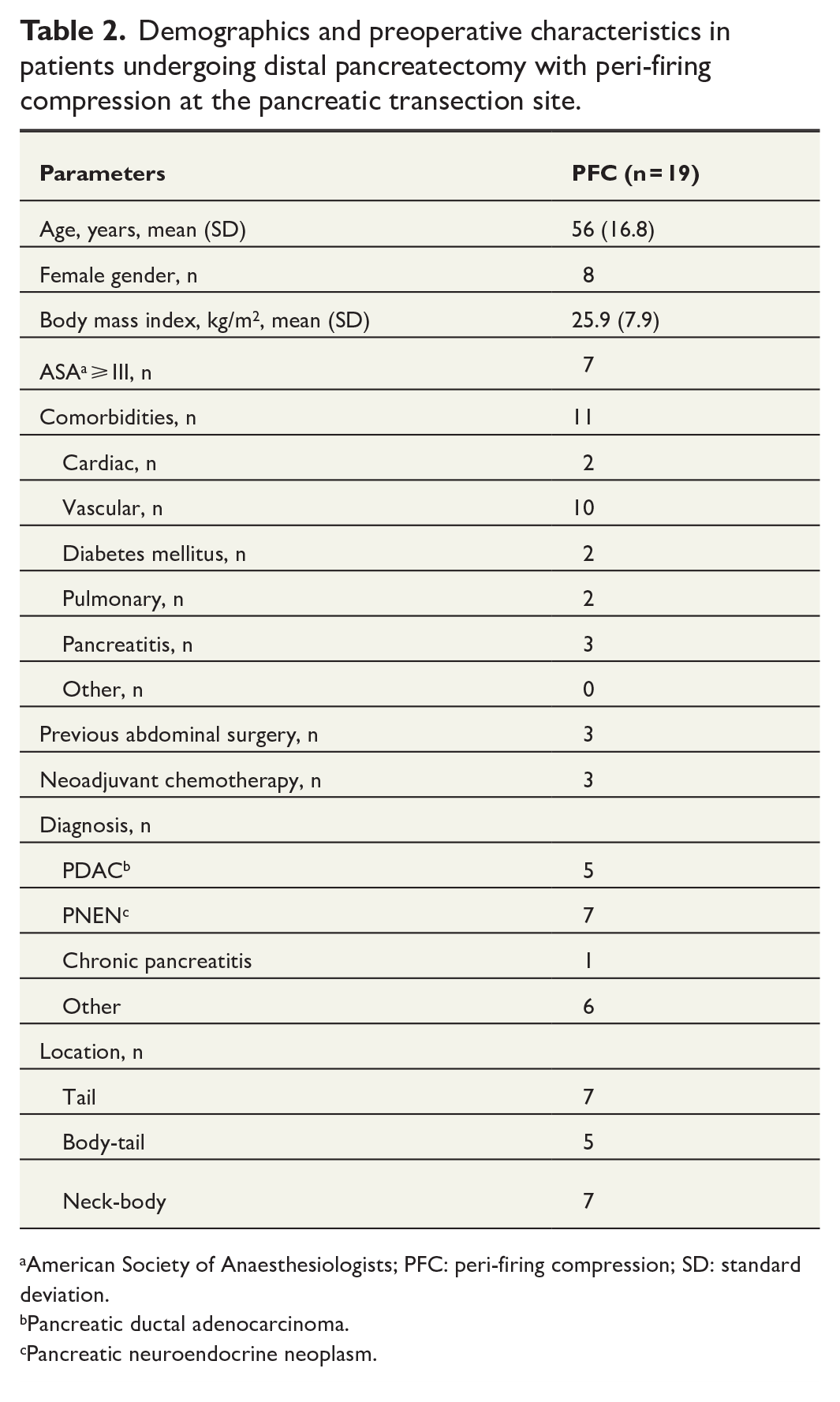
American Society of Anaesthesiologists; PFC: peri-firing compression; SD: standard deviation.
Pancreatic ductal adenocarcinoma.
Pancreatic neuroendocrine neoplasm.
Intraoperative data in patients undergoing distal pancreatectomy with peri-firing compression at the pancreatic transection site.
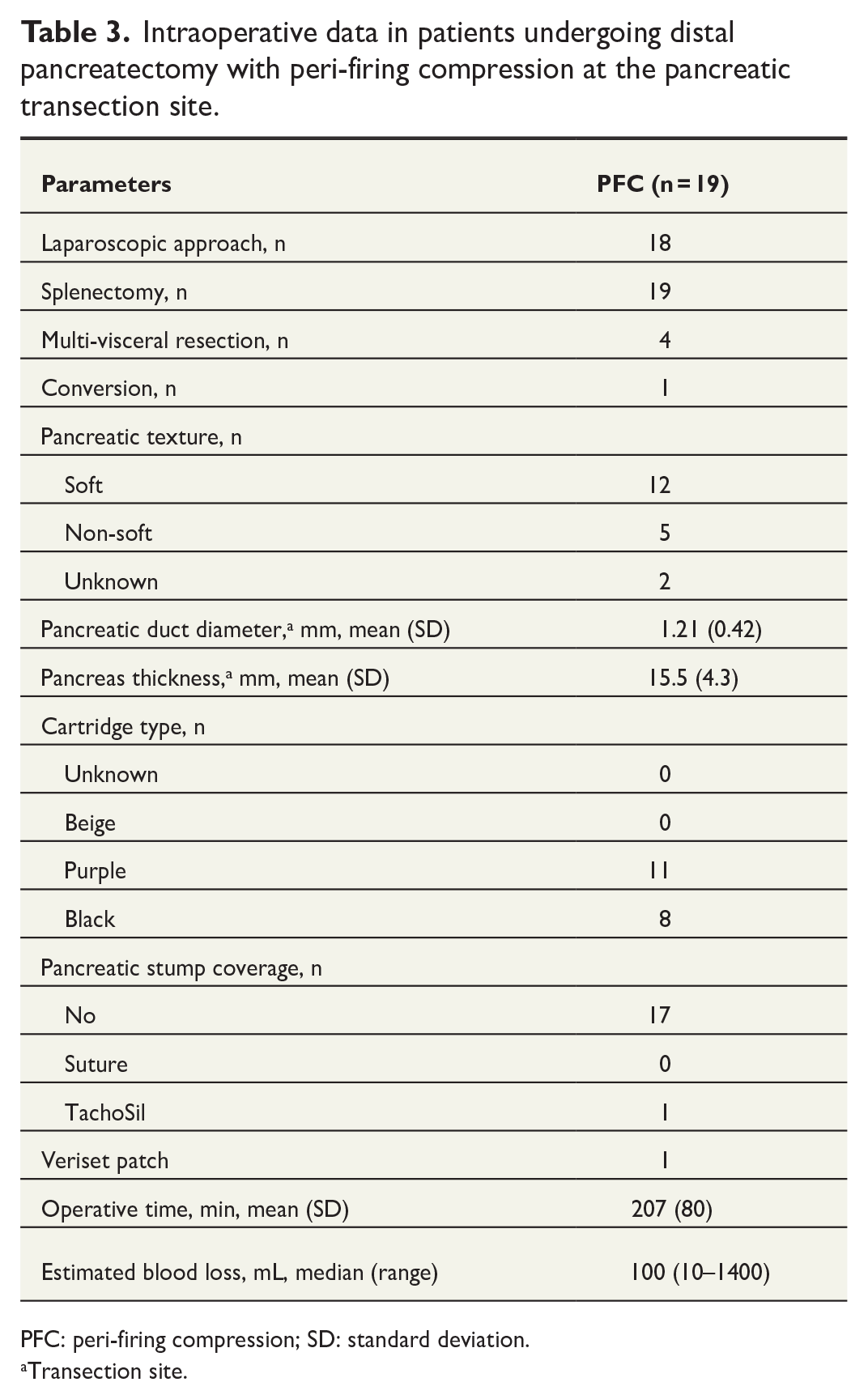
PFC: peri-firing compression; SD: standard deviation.
Transection site.
Postoperative results in patients undergoing distal pancreatectomy with peri-firing compression at the pancreatic transection site.
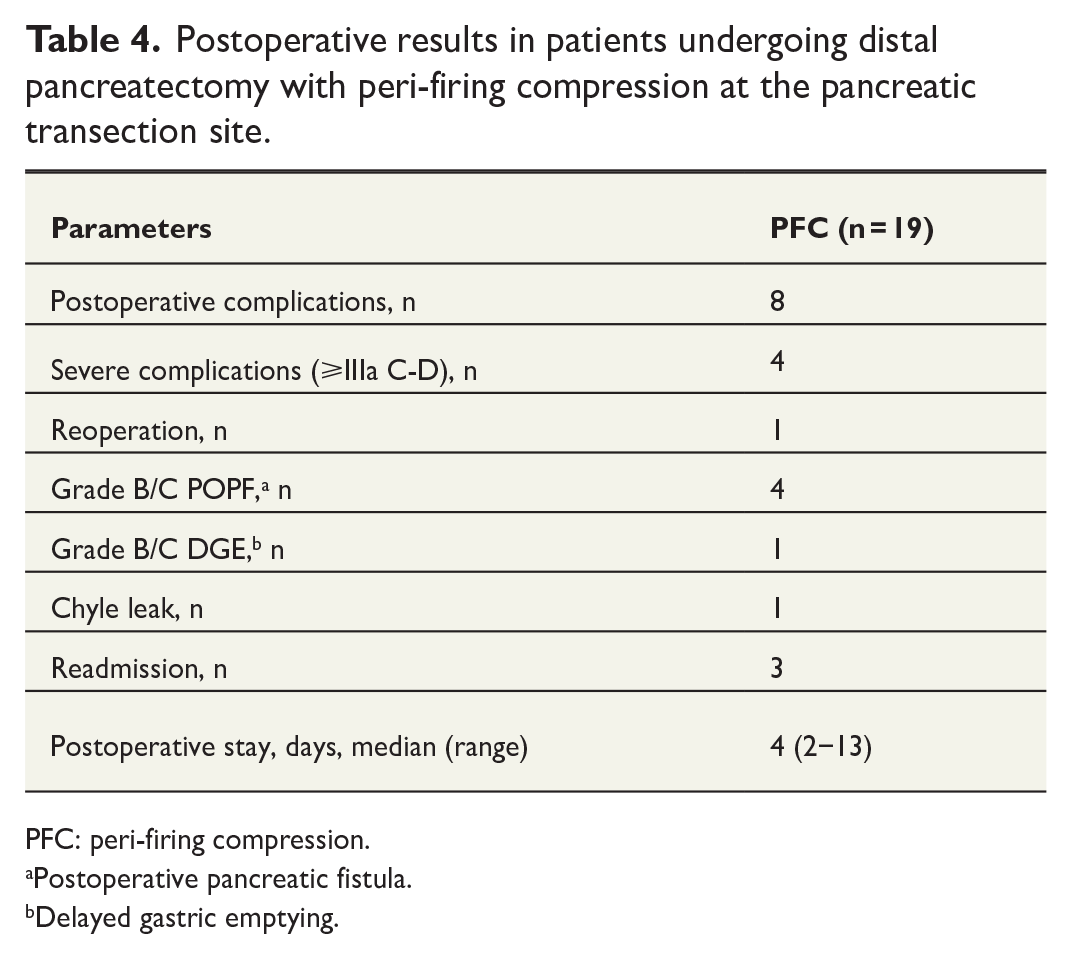
PFC: peri-firing compression.
Postoperative pancreatic fistula.
Delayed gastric emptying.
Subgroup analyses were performed to assess the outcomes for different cartridges used. The proportion of patients with soft pancreas texture was greater and mean gland thickness at the transection site was smaller when purple cartridges were used (Table 5). The latter was associated with the lower incidence of postoperative complications. Only one patient experienced CR-POPF after using purple cartridge with PFC. However, the difference between the groups was not statistically significant.
Postoperative results in patients undergoing distal pancreatectomy with peri-firing compression at the pancreatic transection site stratified by the type of stapler cartridge used.
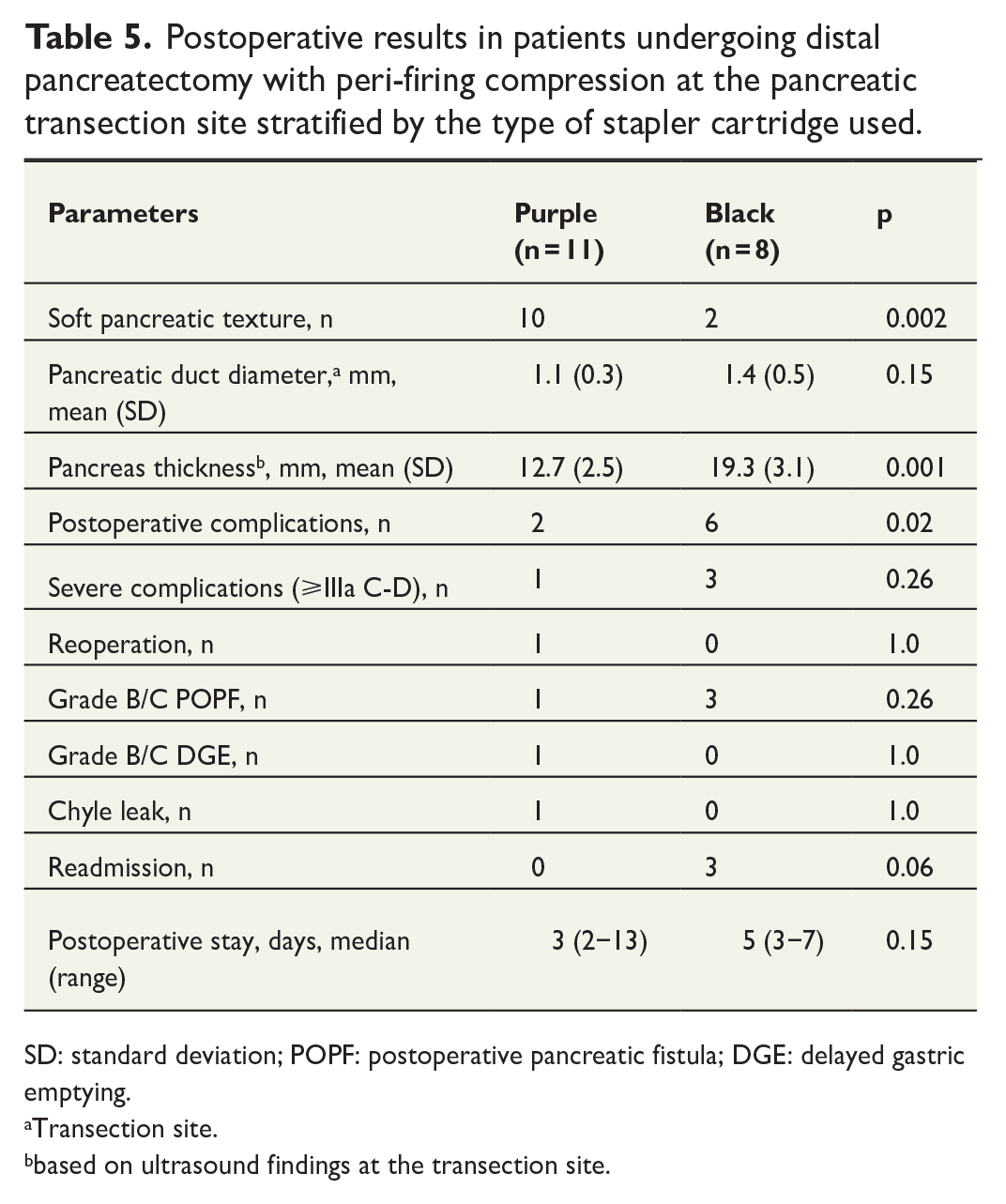
SD: standard deviation; POPF: postoperative pancreatic fistula; DGE: delayed gastric emptying.
Transection site.
based on ultrasound findings at the transection site.
Discussion
We observed no reduction in the incidence of CR-POPF with PFC during DP. In fact, CR-POPF rate was similar to that previously reported for DP without PFC. 23 Other postoperative outcomes were also comparable. Our findings contradict previously published literature on this topic. In 2011, Nakamura et al. 10 found a significant reduction in postoperative pancreatic fistula following DP when using the PFC technique. In 2015, Ariyarathenam et al. 8 presented similar results when using a variant of the technique (3 + 1 min compression pre- and post-firing, respectively), although this study had no control group. In 2018, Hirashita et al. 9 demonstrated a lower rate of CR-POPF using a PFC technique.
Systematic review of the literature revealed several interesting findings when comparing with our results. First, studies on PFC are mostly case series, while only two case–control studies have been published to date. Although reporting significant reduction in CR-POPF with PFC, these include relatively small number of patients. Second, some of these studies report 18%–22% CR-POPF after PFC, which is in agreement with our experience with CR-POPF occurring in roughly 19% of DP without PFC. 23 Third, different type of stapler was used in most of the studies (Echelon™ Stapler, Ethicon Endo-Surgery, Cincinnati, OH, USA). Furthermore, cartridge selection policy and specifics of PFC varied from study to study. Fourth, study population reported in the literature is different from ours as all of them, except one, originate from Asia.
In the subgroup analysis, we found significantly more complications in patients where the pancreas was divided with a black cartridge rather than a purple, but still no difference in CR-POPF. Although not significant, there was a tendency toward a lower incidence of CR-POPF among the patients where the parenchyma was divided with a purple rather than a black cartridge. The type of magazine used is a surrogate for the thickness of the pancreas, and our results may suggest a benefit from PFC when dealing with a thin pancreas. Importantly, a recently published consensus article suggested that a stapling technique cannot be used in all cases of left pancreatectomy because of variations in pancreatic size and texture. 7 Surely, the lower rate of CR-POPF may also be a result of a thin pancreas itself and not the PFC technique.
There are several limitations with this study. An obvious weakness is the low sample size. That said, this study was conducted to get an overview and identify areas for further research, as well as for validating results from previous studies. A valuable addition to our study would be calculation and incorporation of distal-fistula risk score (D-FRS) 24 or DISPAIR score. 25 Unfortunately, the data needed for doing this calculation were not available to us.
In conclusion, current evidence on potential benefits of PFC in DP is limited in quantity and quality. Furthermore, literature data are vastly heterogeneous. In our experience, PFC per se did not reduce the incidence of CR-POPF. Yet there might be a slight reduction in CR-POPF with the use of PFC-technique in patients with a thin pancreas. These findings should be investigated in future studies.
Footnotes
Author contributions
D.K., M.A.S., T.K., S.Y., and B.E. contributed to study design. D.K., M.A.S., and T.K. contributed to data acquisition and analysis. D.K., M.A.S., and T.K. contributed to data interpretation. T.K. and M.A.S. contributed to manuscript drafting. D.K., S.Y., and B.E. contributed to critical revision. D.K., M.A.S., T.K., S.Y., and B.E. contributed to final approval. D.K., M.A.S., T.K., S.Y., and B.E. had agreement to be accountable.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.