
Abstract
Background/Purpose:
Despite retrospective data indicating short-term superiority for laparoscopic distal pancreatectomy compared to open distal pancreatectomy, the implementation of the procedure has been slow. The aim of this study was to investigate whether patients operated with laparoscopic distal pancreatectomy during the early phase of introduction are at higher risk for complications than patients operated with open distal pancreatectomy.
Methods:
A retrospective single-center analysis of patients operated with laparoscopic distal pancreatectomy (n = 37) from the introduction of the procedure and comparison regarding demographic data, preoperative data, operative factors, and postoperative outcomes to patients operated with open distal pancreatectomy was done.
Results:
Operation duration shortened (195 vs 143 min, p = 0.04) and severe complications reduced (37% vs 6%, p = 0.02) significantly in the laparoscopic distal pancreatectomy group between the first half of the study and the second half. Blood loss was significantly (p < 0.001) lower in the laparoscopic distal pancreatectomy group (75 mL) than in the open distal pancreatectomy group (550 mL), while complication rate and hospital stay as well as the percentage of radical resections were the same.
Conclusion:
Laparoscopic distal pancreatectomy can be introduced without jeopardizing patient safety and well-being during the early learning curve. The procedures should be compared in a prospective randomized manner.
Introduction
Laparoscopic distal pancreatectomy (LDP) was introduced in the 1990s, and due to faster postoperative recovery, shorter hospital stay, and reduced bleeding, it successively became the golden standard for benign and low malignant lesions of the pancreatic body and tail (1–5). Despite initial concerns about the oncological safety of the procedure, it is being increasingly performed for adenocarcinoma of the pancreas as well (6). Unfortunately, published data are limited to selected cohorts, and no randomized controlled trial comparing LDP with open distal pancreatectomy (ODP) has been performed. Regarding hospital stay and blood loss, though, it is strongly suggested that LDP has advantages compared to ODP. Despite this, the implementation of this procedure has been slow. In the United States, only about 20% of distal pancreatectomies performed in 2003–2009 were done as LDPs, while in recent years some centers have advanced to performing majority of distal pancreatectomies as LDPs (7, 8). The situation in Sweden is even more discouraging, with vast majority of the distal pancreatectomy procedures found in the Swedish pancreatic surgery registry being ODPs. There may be many reasons for the reluctance to introduce new surgical techniques. Lack of equipment, lack of expertise, fear of bad outcomes, and economic limitations are some reasons brought forward. As with all other procedures, LDP has a learning curve, although research is limited. Results indicate that 20 cases are sufficient for climbing the learning curve for trained laparoscopic surgeons (9–11).
There may be an increased risk of severe complications during the introduction of new surgical procedures. If they are too harmful compared to the golden standard, the technique may fall into disrepute and be impossible to introduce.
The aim of this study was to analyze the safety of introduction of LDP at a pancreatic center in relation to open surgery in the same center.
Methods
A retrospective analysis of all attempted LDPs between September 2012 (first procedure performed at the department) and March 2015 at our institution as well as all ODPs performed during the same period and 20 months before was carried out. The total number of pancreatic resections performed at the institution during this 31-month period was 195. Patient demographics, preoperative assessment of indication for surgery, as well as reasons for choosing LDP or ODP, operative data, and postoperative outcome were analyzed. Complications were registered according to the Clavien–Dindo classification (12). The analysis was done when all patients had at least 3-month follow-up.
ODPs with multiorgan resection were included for completeness. LDPs (intention to treat) were compared to ODPs without multiorgan resection, and conversions as well as severe complications in the LDP group were analyzed. The first half of the LDP cases was compared to the second half regarding indications, tumor size and location, operation duration, and conversion rate.
The technique used for LDP was initial mobilization of the left colonic flexure along with division of the spleno-colic ligament. Next step was division of the gastrocolic ligament followed by exposure of the lower border of the pancreas. After localization of the tumor with laparoscopic ultrasound, the posterior border of the pancreas was dissected and then pancreas was divided using linear stapler. After this, the dissection was done in an antigrade manner including the splenic vessels when splenectomy was also planned. In cases of spleen-preserving surgery, the distal pancreatic tail was dissected from the splenic hilum while the resection was concluded by division of the spleno-renal ligament in other cases.
Data are presented as median (range) unless otherwise stated. Statistical analyses were done using IBM SPSS Statistics version 22 (IBM Corporation, Armonk, NY, USA). The study protocol was accepted by the regional ethic board at Linköping University, Linköping, Sweden. A patient consent was not needed according to the ethical board.
Results
A total of 82 patients were included: 44 males and 38 females. Median age was 64 years (17–83 years). Table 1 shows the demographic data of LDP and ODP patients. LDPs were performed by two surgeons (A = 32, B = 5), while ODPs were performed by five surgeons (A = 22, B = 16, C = 5, D = 1, E = 1). Body mass index (BMI) was similar in the groups as was the percentage of patients earlier operated in the abdomen.
Demographic data for 82 patients operated with distal pancreatectomy.
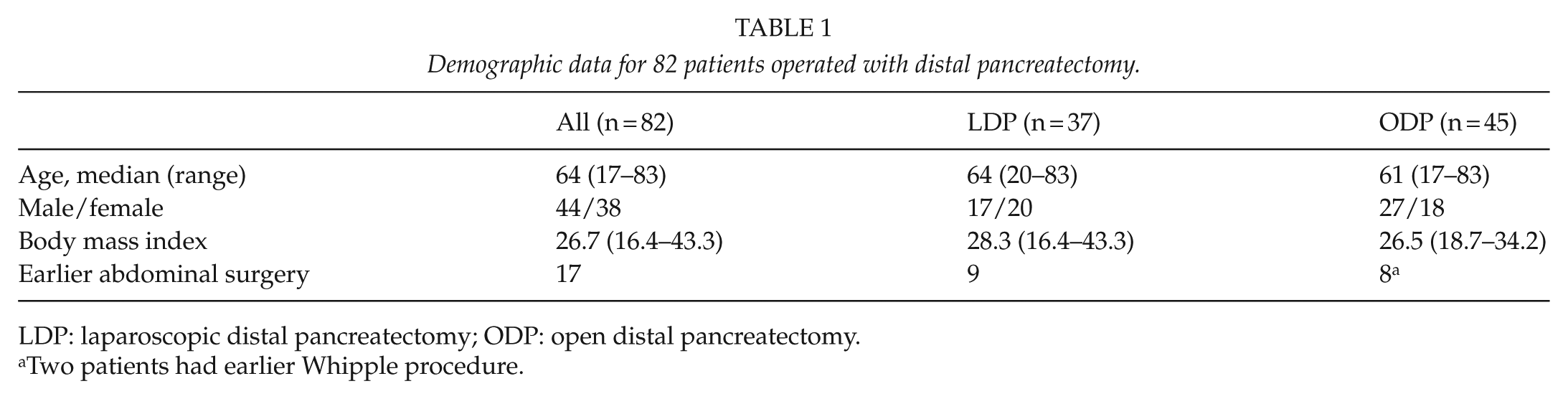
LDP: laparoscopic distal pancreatectomy; ODP: open distal pancreatectomy.
Two patients had earlier Whipple procedure.
Indications for surgery were suspicion or proven malignancy in 32 patients (39.0%), suspected pre-malignant or low malignant lesions in 48 (58.6%), and benign disease in 2 (2.4%). There were more overt malign indications in the ODP group (p = 0.013). Table 2 shows the preoperative disease data.
Pre-operative data for 82 patients operated with distal pancreatectomy.
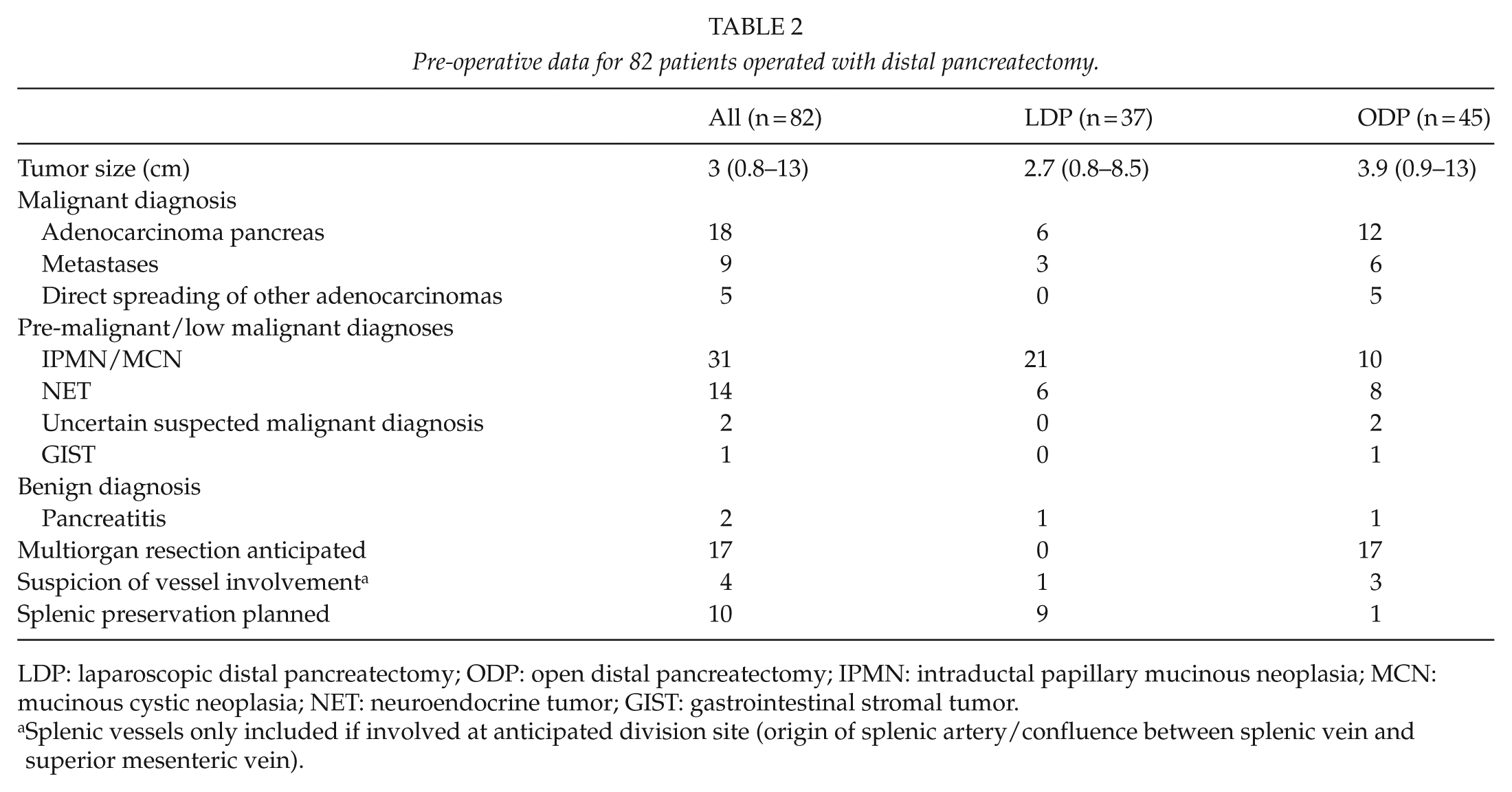
LDP: laparoscopic distal pancreatectomy; ODP: open distal pancreatectomy; IPMN: intraductal papillary mucinous neoplasia; MCN: mucinous cystic neoplasia; NET: neuroendocrine tumor; GIST: gastrointestinal stromal tumor.
Splenic vessels only included if involved at anticipated division site (origin of splenic artery/confluence between splenic vein and superior mesenteric vein).
There were significantly more anticipated multiorgan resections in the ODP group, and during the second half of the study period, this was the major reason for choosing ODP. During the first half, only two (11%) LDPs were planned as splenic preserving, while this figure was seven (37%) in the second half. In the ODP group, one spleen-preserving operation was planned, while in about half of the patients the diagnosis would not have demanded splenectomy (Table 2).
Main factors used to select patients for LDP at the beginning were absence of anticipated multiorgan resection, tumor site (tumors in close proximity to the superior mesenteric vein were considered contraindicating LDP), tumor type (suspected or confirmed adenocarcinoma of the pancreas was considered indication for ODP), tumor size (no formal cut-off was made, but larger tumors were more likely to be treated with ODP), and earlier abdominal surgery. During the latter part of the study period, earlier abdominal surgery, size, and tumor site were not considered contraindication for LDP. Neither was close proximity to the superior mesenteric vein considered as long as the anticipated site of pancreatic division was not on the right side of the vein. Anticipated multiorgan resections remained contraindications for LDP with the exception of minor gastric resections. After the start of LDPs, 10 ODPs without multiorgan resection were performed, making LDPs 79% of distal pancreatectomies without multiorgan resections.
Operation duration was 168 min (80–280 min) in the LDP group compared to 210 min (65–457 min) in the ODP group (p = 0.06), and estimated blood loss was 75 mL (0–7700 mL) and 1500 mL (25–3800 mL), respectively (p < 0.001). In the ODP group, multiorgan resections were done in 23 (51%) of the cases, while the remaining 22 (49%) involved only pancreas and the spleen (Table 3).
Operative and postoperative data for 82 patients operated with distal pancreatectomy.
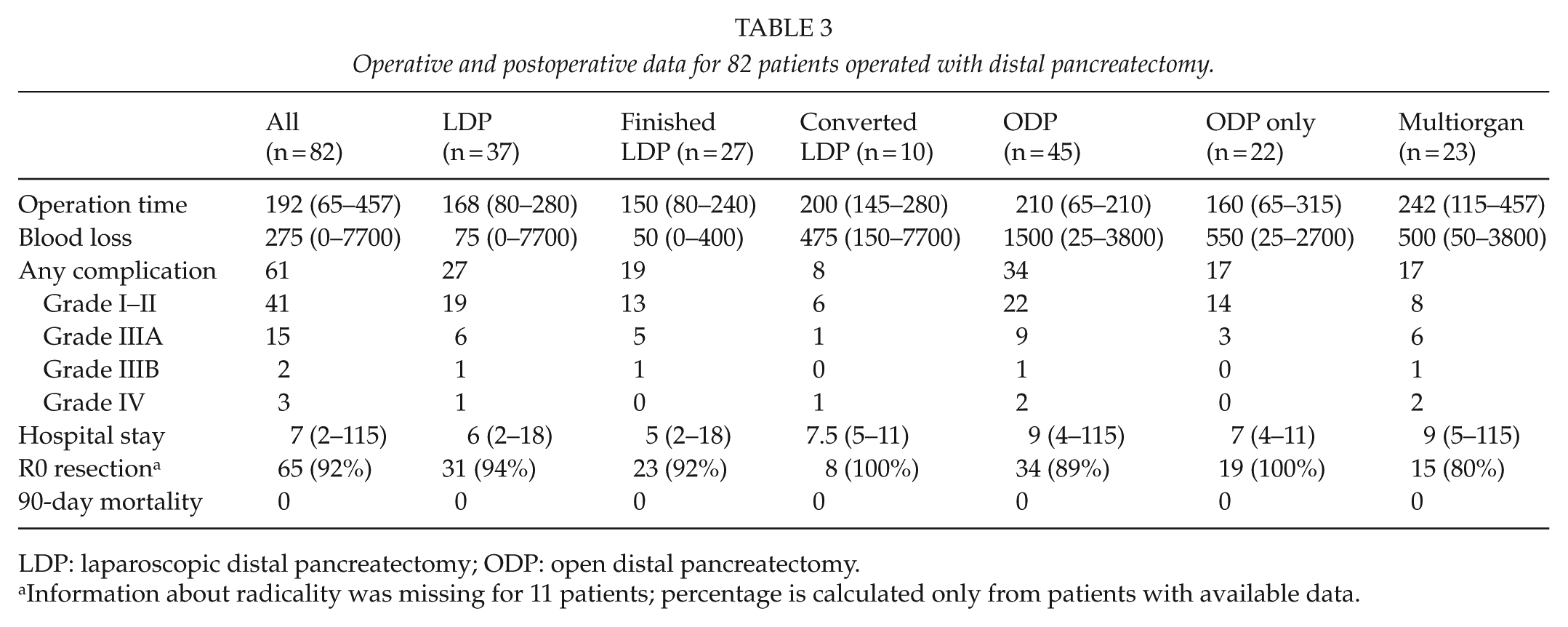
LDP: laparoscopic distal pancreatectomy; ODP: open distal pancreatectomy.
Information about radicality was missing for 11 patients; percentage is calculated only from patients with available data.
Changes in LDP
The LDP patients operated during the first half of the study period were compared to the second ones operated during the second half. Operation duration was 195 min (80–240 min) during the first half compared to 143 min (90–280 min) during the second half (p = 0.04). Bleeding, tumor size, conversion rate, and hospital stay were the same in the groups. In the early group, 37% experienced complications ⩾3A according to the Clavien–Dindo classification compared to 6% in the second half (p = 0.02).
Comparison of LDP (Attempted and Completed) and ODP without Multiorgan Resection
LDP (attempted and completed) was associated with less blood loss than ODP (p < 0.001), while operation duration, hospital stay, and complications ⩾3A according to the Clavien–Dindo classification were the same in the groups (Table 3).
Analysis of Conversions and Severe Complications
The reasons for conversion from LDP to ODP were bleeding from vasa brevia (n = 1), uncertain radicality (n = 1), bleeding from splenic vessels (n = 3), tumor growth on stomach/colon (n = 2), or difficult dissection posterior to the pancreas (n = 3). Two patients experienced complications ⩾3A according to the Clavien–Dindo classification, one sub-phrenic abscess, and one extensive bleeding from the left kidney vein occurring after conversion to ODP requiring intensive care unit (ICU) care (4B).
In the group of patients with completed LDPs, six (22%) patients experienced complications ⩾3A. Of those, five had percutaneous drainage of the abdomen or pleural cavity, while one patient was reoperated due to bleeding from the stapler line in pancreas. In the group of ODPs without multiorgan resection, three (14%) of the patients experienced complication of the same grades (not significant (ns); Table 3).
Discussion
This study focused on the safety of LDP during an introduction period for the procedure. The main drawback of this study besides the limited number of patients included the selection bias created with introduction of LDPs in selected cases. Although severe complications were more common during the first half, these were mainly of grade 3A, and no 90-day mortality was found. Despite convincing evidence for short-term benefit of LDP compared to ODP, implementation of LDP is slow (2, 3, 5). This study has investigated one of the possible explanations for this, namely, the risk of adverse outcomes for patients during the introduction of a new procedure at the institution. Although conversion rate was considerably higher than in recent reports from centers with experience of the procedure, the rate of conversion was comparable to early reports (13). This study shows, in line with many other studies, that LDP reduces blood loss while duration of hospital stay did not reach statistical significance (2, 3, 5). It has to be kept in mind that evaluating blood loss in laparoscopic procedure compared to an open one may be difficult; in addition, these results may partly be due to selection bias. Nevertheless, the difference found in this study, between all intended LDPs and ODPs without multiorgan resection, still supports earlier findings that LDP is associated with reduced bleeding compared to ODP. In contrast to earlier reports, operation time was similar in the groups despite the fact that this cohort represents the start of a learning curve at a pancreatic center with annual number of 75 pancreatic resections. Although the LDPs were operated by two surgeons compared to five surgeons performing the ODPs, 96% of the ODPs were performed by three pancreatic surgeons and the remaining two procedures were done as a part of resections for advanced gastric cancer and are therefore not included in the comparison between LDPs and ODPs without multiorgan resections. Patients undergoing LDPs that were converted to ODPs could be expected to have worse outcomes than patients undergoing planned ODP due to the acuteness of some conversions. In this study, the subgroup of patients demanding conversion to open surgery, although limited in number, did not have more adverse outcomes than patients undergoing open surgery directly. This is an important finding as conversion to open surgery can be expected during the introduction of LDP (13). The overall rate of complications in this study was similar in the groups as was the occurrence of severe complications. This finding is similar to earlier studies and suggests that the introduction of LDP does not carry increased risk for the patients treated during the early learning curve.
The vast majority of pancreatic resections is performed for malignant or pre-malignant lesions. Therefore, the oncological completeness of LDPs is of great importance. Although not studied in a prospective randomized manner, published data suggest that LDP in carefully selected material is not inferior to ODPs in the settings of pancreatic adenocarcinoma (14). In this study, no difference was found in the proportion of radical resections (R0) as this could be confirmed in 94% of LDPs compared to 100% of ODPs without multiorgan resection.
Conclusion
LDP can be introduced with acceptable results without jeopardizing patient safety and well-being. The procedures need to be compared in prospective randomized settings.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.