
Abstract
Abstract
Introduction:
Paragangliomas are rare tumors that can be sporadic or familial. They are located along the sympathetic or parasympathetic chain with an incidence from 0.005% to 0.1% in the general population. 1 About 85% of paragangliomas are below the diaphragm in difficult anatomic locations. Majority are functional. 2 The retroperitoneoscopic approach has been used to resect these tumors with certain advantages over the transperitoneal method, including a shorter operative time, reduced pain, a shorter recovery, and subsequently earlier hospital discharge. 3
Materials and Methods:
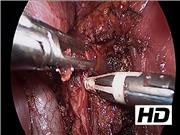
The aim of this video is to present a resection of a recurrent paraganglioma in a difficult anatomic location.
Results:
A 45-year-old lady was investigated for hypertension and palpitations in 2010. She was found to have a 4.1 cm left extra-adrenal pheochromocytoma/paraganglioma distorting the left renal vessels with markedly raised normetanephrine excretion. The patient underwent an open left excision histology, which confirmed a paraganglioma. In 2014, the patient was demonstrated to have a recurrence, with a 1.5 cm soft tissue nodule in the resection bed and raised normetanephrines. She had a transabdominal laparoscopic left adrenalectomy, which removed a normal left adrenal gland but failed to find the recurrence. The patient was referred for genetic testing. She was subsequently referred to the Surgical Endocrine Department. Diagnosis of a recurrent paraganglioma was verified by biochemistry (elevated normetanephrine levels) and imaging (computed tomography, magnetic resonance imaging adrenals, and positron emission tomography-fluorodeoxyglucose scan). The patient had a further operation to remove the recurrence by a laparoscopic retroperitoneal approach. The patient was placed in the ventral decubitus position with three ports sited in the left lumbar region: 5 mm lateral, 12 mm balloon port, and a 10 mm medial port. The retroperitoneal space was developed by blunt dissection and CO2 insufflation to 25 mmHg. Dissection was difficult because of previous adhesions. The superior pole of the kidney and renal hilum were identified and recognition of metal clips from the previous surgery helped to find the tumor. The recurrent paraganglioma was lying behind the left renal artery and in proximity with the aorta. A combination of blunt and sharp dissection (using the Ligasure device) was used to dissect the tumor from the surrounding structures. The tumor was removed in an Endocatch bag and Floseal was used at the end of the procedure to ensure hemostasis.
Conclusions:
The posterior retroperitoneoscopic approach for resection of retroperitoneal paragangliomas is safe and has good outcomes. It can be considered for patients with previous abdominal surgery and in cases difficult to access by a transabdominal approach. Reviewing imaging before and during surgery facilitates the dissection especially in scar tissue.
No competing financial interests exist.
Runtime of video: 9 mins 3 secs


Get full access to this article
View all access options for this article.