
Abstract
Abstract
Introduction:
Vascular malformation of the thyroid gland extending into the endolarynx is a rare disorder. We present the case of a patient with a complex recurrent high-flow arteriovenous malformation on the right side of the neck involving a remnant thyroid gland and extending into the right endolarynx. This report concentrates on the laryngoscopic features and preoperative embolization of the lesion.
Case:
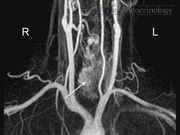
A 42-year-old physiotherapist presented to our department with symptoms of increasing hoarseness, dyspnea on exertion, laryngeal globus sensation and dysphagia, a nagging impulse to clear her throat, tussive irritation, and a feeling of mucous obstruction. A nontender, soft vibrating mass was palpable on the right side of the neck with a hardly visible scar after subtotal hemithyroidectomy. The medical history included embolization and subtotal right hemithyroidectomy for a high-flow arteriovenous malformation of the thyroid gland in 1993 (for details, see case report in Thyroid 1 ). The actual laryngoscopy revealed a right vocal fold with reduced mobility and a mass on her right Morgagni fossa. A repeat magnetic resonance imaging (MRI) demonstrated growth of a recurrent vascular malformation and compression of the larynx. Consecutively, re-embolization of the lesion was offered, but the patient opted for a combined embolization and surgical excision. Assessment before embolization included MRI angiography (Magnetom Aera 1.5 T; Siemens, Forchheim, Germany) for demonstration of the flow characteristics, pathoanatomical location, and extension of the hemangioma. For embolization, a digital subtraction angiography (Artis Zee; Siemens) was carried out with a 4F (1F = 0.3 mm) multipurpose catheter and a 5F 90-cm sheath in a coaxial technique in the right common carotid artery, confirming vascular supply of the cervical angioma by the superior thyroid artery corresponding to the MRI. Superselective angiography was obtained in a triaxial technique with a 5F sheath in the common carotid artery, a 4F multipurpose catheter in the superior thyroid artery, and a 2F microcatheter in the peripheral portions of the superior thyroid artery. As a first step, superselective embolization treatment was started in the lateral extralaryngeal part of the angioma. Complete occlusion was achieved using Onyx 18 (Onyx™ Liquid Embolic System; ev3™, Plymouth, MN). A more medial vessel was selectively intubated using an Apollo 2.7/1.5F with a 15-mm detachable tip. After injection of 40% glucose, the vascular malformation was occluded in the laryngeal and pharyngeal portions up to the jugular fossa by careful injection of n-butyl-cyanoacrylate glue (Glubran 2; GEM, Viareggio, Italy) mixed with a contrast agent (Lipiodol UltraFluid; Guerbet, Villepinte, France). Postinterventional X-ray visualized the effectively treated areas of the large cervical angioma. Completion hemithyroidectomy on the right was carried out the day after embolization. Postoperative laryngeal assessment on day 2 was largely unremarkable, but later on revealed a complete still stand of her right vocal fold, edema, and inflammation of the endolarynx. She underwent an intensive rehabilitation program. Thereafter, she continued to have a high-grade voice handicap of 39 points on the Voice Handicap Index (VHI)-12.2,3 Two months after surgery, the bulging mass of the right endolarynx started to decrease in size. One year after surgery, there was no inflammation of the larynx. Right vocal fold still stand and position of the arytenoid indicate definitive impairment/paralysis. Her voice improved to a degree that allowed her to continue working as a physiotherapist. Embolization followed by excision is an accepted treatment standard for arteriovenous malformations of the head and neck. 4 Moreover, treatment options for vascular lesions in other body compartments or organs increasingly include the use of interventional techniques.5,6 Follow-up revealed persistence of the endolaryngeal hemangioma till 2 months after the operation. Eighteen months after re-embolization and completion of hemithyroidectomy, there was no recurrence of the endolaryngeal hemangioma. Preoperative assessment demonstrated partial immobility of the right vocal fold, with a postoperative diagnosis of definitive paralysis. Whether this is a result of a combination of pre-, intra-, and postoperative damage or surgical recurrent laryngeal nerve damage during surgery remains unknown. Despite this fact, her phonation improved.
Conclusion:
This is the first report of a recurrent high-flow arteriovenous malformation of the thyroid gland extending into the endolarynx. Embolization followed by excision is an accepted treatment standard. The interventional technique offers safe treatment of arteriovenous malformations of the head and neck. We suggest using this technique in future cases only to prevent possible recurrent laryngeal nerve damage with completion hemithyroidectomy.
Authorship:
Drs. Massmann and Bader share first authorship.
Acknowledgments:
We thank Mr. Andreas Pohl at Saarland University Hospitals for kindly providing assistance in producing the video. We thank Marco Blechschmidt from Radio Homburg for speech recording and Mr. Samuel Somers-Heslam, Cambridge, United Kingdom, for grammar revision. We also thank the patient for consenting to this publication.
No competing financial interests exist.
Runtime of video: 5 mins 52 secs


Keywords
Get full access to this article
View all access options for this article.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.