
Abstract
Abstract
Introduction:
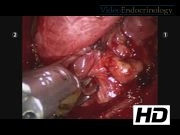
Recently, indocyanine green fluorescence imaging (ICG-FI) using an intravenous technique has been described for various procedures, such as cholecystectomy, liver surgery, and nephrectomy.1,2 To the best of our knowledge, the use of ICG during thyroid surgery has not been described. The aim of this video is to show the use of intraoperative ICG-FI during robotic total thyroidectomy and describe the differential ICG fluorescence staining characteristics of various anatomical structures.
Case Presentation:
A 35-year-old woman was found to have multinodular goiter when she presented with neck pain. Fine-needle aspiration biopsy of a right thyroid nodule measuring 1.6 cm showed atypical cells without being able to exclude papillary thyroid cancer. When recommended total thyroidectomy, the patient expressed interest for a robotic transaxillary approach. Our robotic technique has been described in detail previously. 3 In brief, after positioning, a 5–6 cm incision was made along the lateral border of pectoralis major muscle and a flap was created anterior to the pectoralis fascia. The thyroid gland was exposed and the robot was docked. The right lower and upper pole vessels were initially divided. On this side, intravenous (IV) ICG dye (2.5 mg/mL) was administrated in two separate injections, 1.5 and 2.5 mL, respectively, within an interval of 90 minutes. The thyroid gland demonstrated significance fluorescence in 2 minutes, and this persisted for 30 minutes with each injection. The parathyroid glands showed a more intense uptake that persisted beyond the fluorescence of the thyroid. The recurrent laryngeal nerve, by not taking up the ICG, was visible very clearly in between the fluorescent thyroid and parathyroid tissue. On the left side, two separate dosages of IV ICG, 2.5 and 1.5 mL, respectively, were given within an interval of 60 minutes. By performing a medial to lateral dissection, total thyroidectomy was completed. The recurrent laryngeal nerve on both sides was identified. The parathyroid glands were seen to light up more avidly with the dye, for about 40 minutes, which persisted beyond visualization of the thyroid, and this helped with their identification and preservation. The patient was discharged home on postoperative day 1 uneventfully. Her follow-up examination at 2 weeks was unremarkable (calcium: 8.3 mg/dL, phosphorus: 4.2 mg/dL, parathyroid hormone: 16 pg/mL). Final pathology revealed multicentric papillary thyroid carcinoma, without capsular or extrathyroidal extension.
Conclusion:
In summary, we demonstrated the use of intraoperative ICG-FI during robotic thyroidectomy, with suggestions on dosage and timing, as well as a description of what fluorescence patterns are exhibited by the thyroid, parathyroid, and recurrent laryngeal nerve. As experience on this imaging accumulates, potential practical applications in endocrine surgery could evolve.
All authors declare no conflicts of interest.
Runtime of video: 6 mins 41 secs


Keywords
Get full access to this article
View all access options for this article.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.