
Abstract
The significant gap in national information in New Zealand about the prevalence of mental disorders in Pacific people has been a longstanding problem [1]. This paper summarizes the main results of Te Rau Hinengaro: The New Zealand Mental Health Survey (NZMHS) with specific reference to Pacific people. It provides the first comprehensive analysis of the prevalence of major mental disorders among Pacific people in New Zealand.
Previous epidemiological studies in New Zealand have had too few Pacific people to generate reliable prevalence estimates for major mental disorders [2, 3]. What little was known about the prevalence of mental disorders among Pacific people in New Zealand had been drawn from the few prevalence studies performed in the Island nations [4] or from Pacific people's use of mental health services in New Zealand [5, 6]. In the absence of community data, admission rates to inpatient facilities were relied on to estimate the burden of mental disorder in the Pacific population [6]. As a result, in conjunction with the poor recording of ethnicity in official datasets, the widely held view that Pacific people experience lower rates of mental illness compared with other groups in New Zealand was propagated [6].
The international literature supported this supposition as it pointed towards migrants having a lower lifetime prevalence of mental disorders [7]. The Pacific population, however, is characterized by a history of staggered migration to New Zealand that has led to a heterogeneous group of people of varying degrees of acculturation. The NZMHS has provided data, which has not been previously available, on the prevalences of mental disorders and the associated patterns of health service use for Pacific people now resident in New Zealand.
Method
Sample
The NZMHS was a nationally representative household survey of people aged 16 years and over. Face-to-face interviews were carried out by professional interviewers from the National Research Bureau between October 2003 and December 2004. The survey was approved by all 14 regional health ethics committees, with the Auckland Y committee serving as the lead committee. Written informed consent was obtained from all respondents before the interview began. The methods are detailed elsewhere [8, 9].
Overall, the response rate was 73.3%. The interview consisted of two parts. Part 1 included core diagnostic sections and demographics and was administered to everyone (n = 12 992). Part 2 consisted of additional diagnostic sections and other measures of mental and physical health and was administered to a subsample (n = 7435), called the longform subsample. All participants who met certain criteria in the Part 1 diagnostic sections received the long form of the interview. A probability subsample of other participants also received the long form [8, figure 1].
Māori and Pacific people were oversampled. In total, 2457 Māori, 2236 Pacific people and 138 people of mixed Pacific and Māori ethnicity were interviewed. Unless otherwise stated, this paper includes all 2374 Pacific participants. However, in other papers from this survey, in which ethnic comparisons are made, those with both Pacific and Māori ethnicity are classified as Māori, using the standard New Zealand classification.
Diagnostic assessment
The interview included diagnostic sections from version 15 of the World Mental Health (WMH) Survey Initiative version of the Composite International Diagnostic Interview (WMH-CIDI) [10], now known as the CIDI 3.0. This is a fully structured lay interview that generates diagnoses according to ICD-10 [11] and DSM-IV [12]. Only DSM-IV diagnoses are reported here. The WMH diagnostic algorithms used were those current in January 2006. DSM-IV organic exclusions rules were used. Disorders were diagnosed with hierarchy rules except for substance abuse, which is reported whether or not there was dependence. Participants without any symptom ever of substance abuse (alcohol or drugs) skipped the associated dependence section, so dependence is really dependence with abuse at some time.
The CIDI 3.0, like most versions of the CIDI, asks if symptoms have ever occurred and then asks about recency. Twelve-month disorder is diagnosed if full criteria for disorder have ever been met and there have been symptoms or an episode in the past 12 months. Full criteria may not have been met in the past 12 months.
Severity
Severity for a case was based on all disorders experienced in the past 12 months. Definitions used in New Zealand were those developed for the first WMH cross-national paper [13] except for substance dependence for which the National Comorbidity Survey Replication (NCSR) [14] definition was used [8]. Participants were classified with serious disorder if any one of the following occurred in the past 12 months: an episode of bipolar I disorder; substance dependence with serious role impairment (two effects experienced ‘a lot’); a suicide attempt and any WMH-CIDI/DSM-IV disorder; at least two areas of severe role impairment because of a mental disorder in the Sheehan Disability Scale domains; overall functional impairment at a level found in the NCS-R to be consistent with a Global Assessment of Functioning [15] score of 50 or less in conjunction with a WMH-CIDI/DSM-IV disorder. Participants with disorder who were not classified as serious were classified as moderate if interference was reported as at least moderate in any Sheehan Disability Scale domain or if they had substance dependence without substantial impairment. All other participants with disorder were classified as mild.
Correlates
Sociodemographic correlates include age at interview and sex, in addition to educational qualifications, equivalized household income, migration, language and Island group assessed using 2001 Census of Population and Dwellings questions when possible. Educational qualifications were assessed using questions about school and post-school qualifications. Household income was missing for 13.0% of respondents and was imputed by linear regression. A modification of the revised Jensen equivalence scale for household income [16] was used to take account of the number of adults and the number of children in the household. Questions about age at arrival and years since migrating to New Zealand were asked of those who were born outside New Zealand. Ethnicity was determined by self-identification, according to the question in the 2001 census. This enables a breakdown to individual Island group for people of Pacific ethnicity.
Analyses
Data were weighted to account for different probabilities of selection that arose from oversampling Māori and Pacific people and the selection of one person per household, differential non-response, and residual differences in age, sex and ethnicity between the sample and the 2001 census population. Additional weights were used to account for selection into the long-form sections of the interview. Analyses were carried out in SUDAAN 9.0.1 with two strata (High Pacific and General) and census meshblocks as the primary sampling units. The sample design was preserved for analysis of subgroups by use of the subpopulation command in SUDAAN [17]. Taylor series linearization [18] was used to approximate the variance of estimates. For prevalences with less than 30 events in the numerator, confidence intervals were calculated according to a method by Korn and Graubard [17, 19].
Results
Profile of Pacific participants
A total of 2374 Pacific people were interviewed in the NZMHS. The ethnic breakdown by Pacific group, age and sex is shown in Table 1. Among these Pacific people, 21.2% spoke only English, 74.2% were multilingual and 4.4% spoke only their native language. The demographic characteristics of the Pacific sample closely reflect those of the Pacific groups in the wider New Zealand population.
Pacific Island, sex and age of Pacific people in Te Rau Hinengaro: The New Zealand Mental Health Survey†
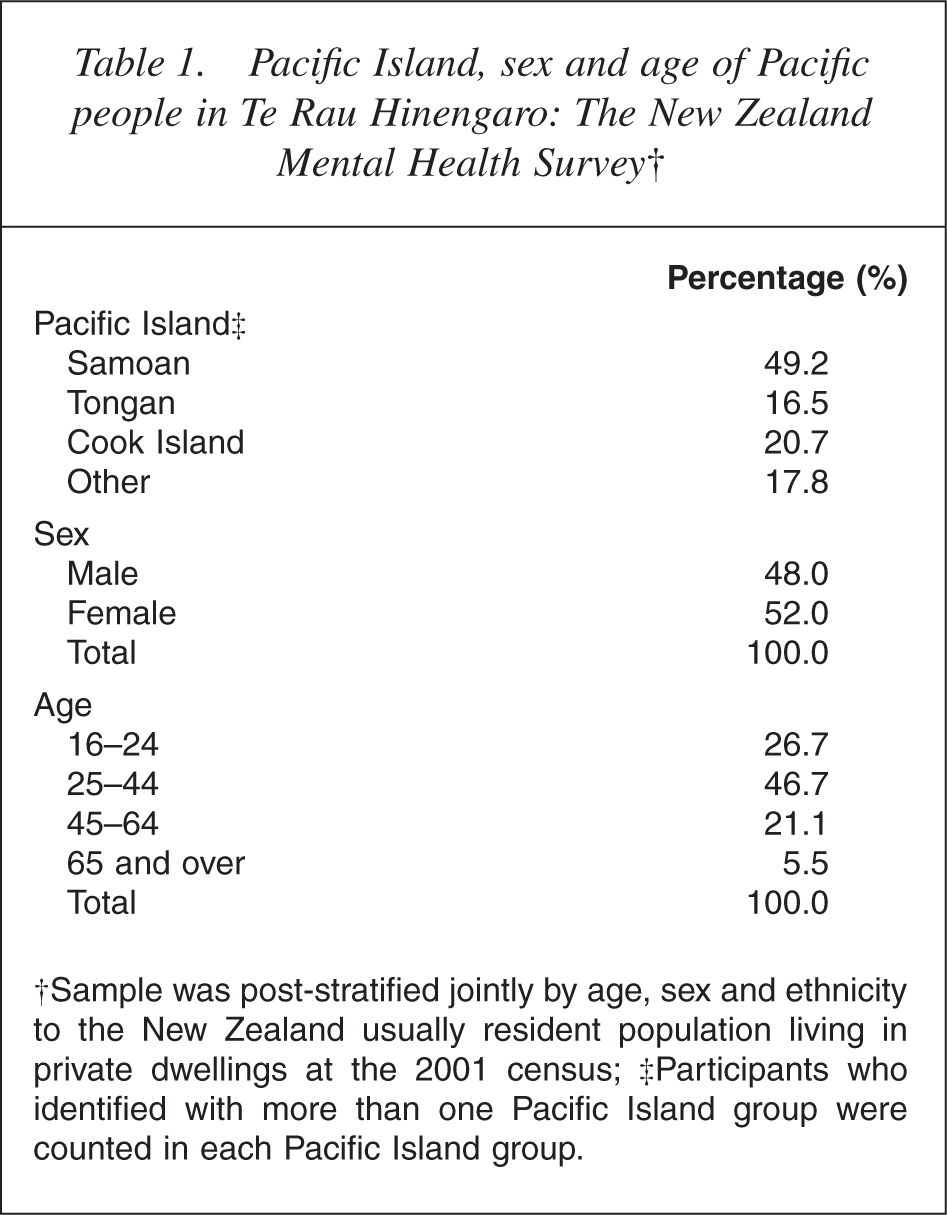
†Sample was post-stratified jointly by age, sex and ethnicity to the New Zealand usually resident population living in private dwellings at the 2001 census; ‡Participants who identified with more than one Pacific Island group were counted in each Pacific Island group.
The Pacific population was also younger than the total New Zealand population: 26.7% were aged 16–24 years (compared with 15.7% for the total New Zealand population). Of the Pacific sample, 42.1% were New Zealand-born and 11.8% were aged under 12 years when they immigrated to New Zealand. Less than half the median income was earned by 28.7% of Pacific people compared with 18.5% of the total New Zealand population. No educational qualification was held by 24.6% of Pacific people compared with 18.5% of the total New Zealand population. Conversely, 28.7% of Pacific people had both school and post-school qualifications compared with 44.4% of the total New Zealand population.
Pacific people tended to live in larger households than other participants. One quarter (23.8%) of Pacific households had more than seven people compared with 3.6% of all households. Pacific people surveyed lived in the areas designated as being of high deprivation according to the small area descriptor of socioeconomic deprivation, the New Zealand Index of Deprivation 2001 (NZDep2001). Fifty-nine per cent of Pacific people lived in the areas of high deprivation (i.e. NZDep2001 deciles 9 and 10) compared with 18.0% overall.
Period prevalences of mental disorders for Pacific people
Table 2 shows that 46.5% of Pacific people had experienced a DSMIV CIDI 3.0 mental disorder at some stage during their lifetime before being interviewed. The most commonly reported lifetime disorders were anxiety disorders (27.7%), followed by mood disorders (19.0%) and substance use disorders (17.7%). Eating disorders among Pacific people were much less common over their lifetime (4.4%).
Lifetime and 12 month prevalences of mental disorders for Pacific people
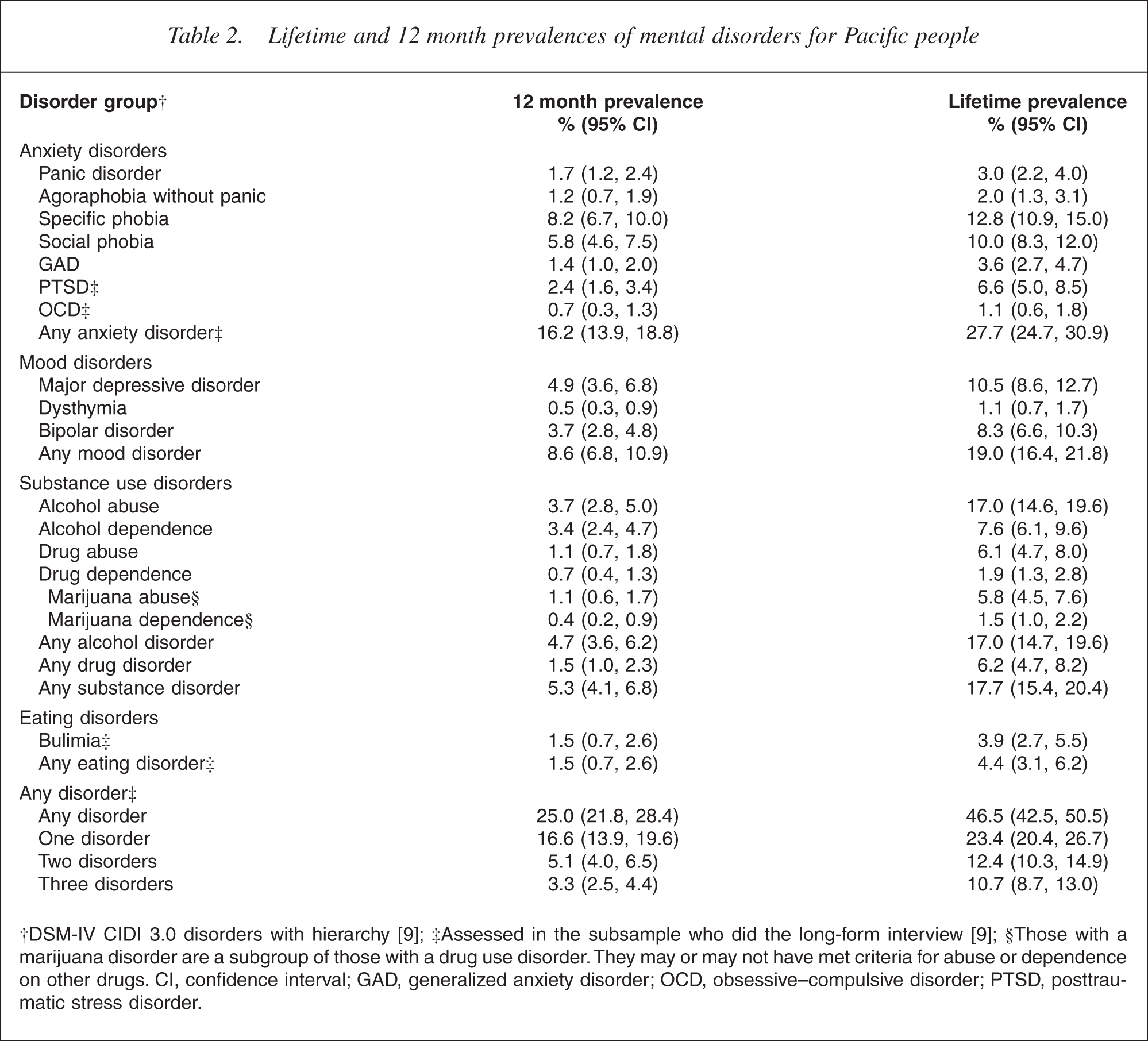
†DSM-IV CIDI 3.0 disorders with hierarchy [9]; ‡Assessed in the subsample who did the long-form interview [9]; §Those with a marijuana disorder are a subgroup of those with a drug use disorder. They may or may not have met criteria for abuse or dependence on other drugs. CI, confidence interval; GAD, generalized anxiety disorder; OCD, obsessive–compulsive disorder; PTSD, posttraumatic stress disorder.
Over the past 12 months, 25.0% of Pacific people experienced a disorder. In the 12 months leading up to the survey, 16.2% of Pacific people experienced an anxiety disorder, 8.6% experienced a mood disorder, 1.5% had an eating disorder and 5.3% had a substance use disorder.
In the 12 months before the survey, 16.6% of Pacific people had a single disorder, 5.1% had two disorders and 3.3% had three or more disorders. In the lifetime of Pacific people, 23.4% had experienced a single disorder, 12.4% had two disorders and 10.7% had three or more disorders.
In the 12 months before the survey, the proportions of Pacific people with single disorder, two disorders or three or more disorders were similar to those reported for New Zealand overall (13.0% [12.1, 14.0], 4.4% [3.9, 4.8] and 3.3% [2.9, 3.7], respectively) [20, 21].
A greater proportion of Pacific people had experienced a DSM-IV CIDI 3.0 mental disorder at some stage during their lifetime compared with the total New Zealand population (46.5% vs 39.5%; 37.9, 41.2) [22, 23]. In the previous 12 months, a greater proportion of Pacific people experienced a disorder compared with the total New Zealand population (25.0% vs 20.7%; 19.5, 21.9). Slightly over 5% (5.3%) of Pacific people had a substance use disorder compared with 3.5% (3.0, 4.0) of the total New Zealand population [20, 21].
When compared with Māori and Other (i.e. non-Māori non-Pacific) ethnic groups [24], Pacific people had a higher prevalence of any disorder and serious disorder. Adjustment for age and sex alone reduced all differences to non-significance and after further adjustment for education and income the prevalence for Pacific people was non-significantly lower than that for Others. This shows that while the burden of mental disorder is high among Pacific people as a population, the excess burden is attributable to the age and gender structure of the Pacific population and socioeconomic correlates.
Twelve-month prevalence and severity of disorders by age and sex
The NZMHS estimates that 25.0% of Pacific people will meet criteria for a DSM-IV mental disorder in a 12 month period. This is slightly higher than that for the total New Zealand population, but lower than some prevalence estimates in overseas communities [25].
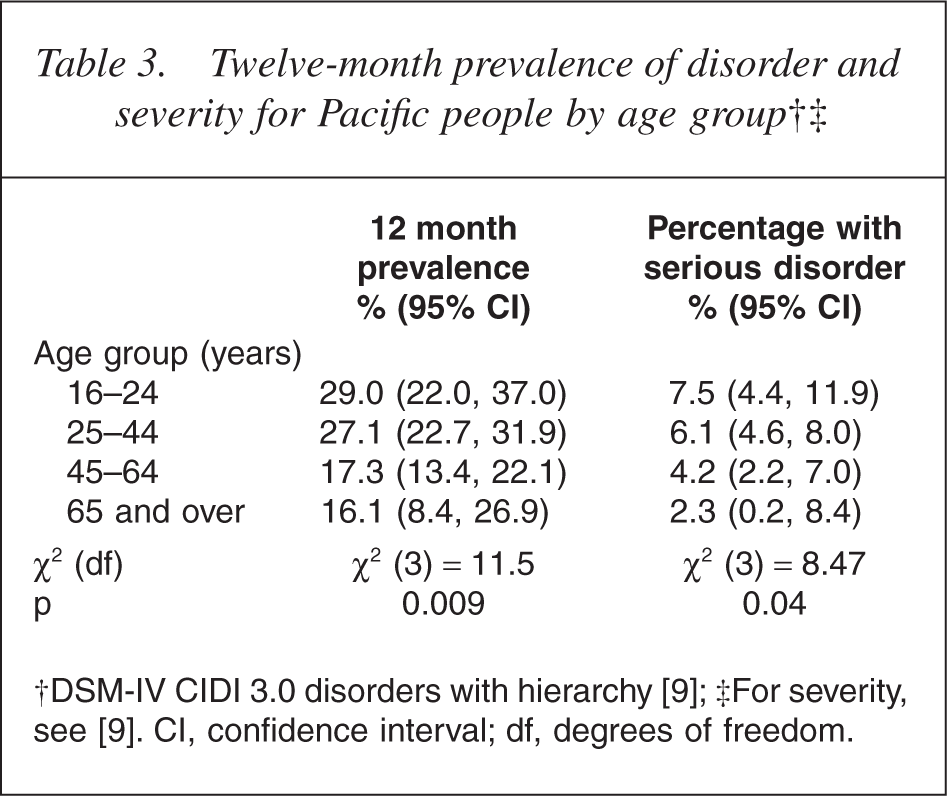
Table 3 indicates that younger Pacific people had a higher 12 month prevalence rate than older people (p = 0.009). Young Pacific people were also more likely to experience a mental disorder classified as serious than older Pacific people (p = 0.04). This is consistent with findings for the total New Zealand population.
Twelve-month prevalence of disorder and severity for Pacific people by age group†‡
The survey found that 26.7% (23.0, 31.7) of Pacific females met criteria for disorder in the past 12 months compared with 22.0% (18.1, 28.0) of Pacific males, but this was not statistically significant. No statistical difference existed between Pacific males and females who reported having a serious disorder (5.4% [3.8, 7.6] vs 6.4% [4.8, 8.4]).
Twelve-month prevalence of disorder by Pacific Island groups
Table 4 shows a breakdown of 12 month prevalence by disorder for the four main Island groups compared with the total Pacific population.
Twelve-month prevalence of disorders for Pacific people by Pacific Island group†
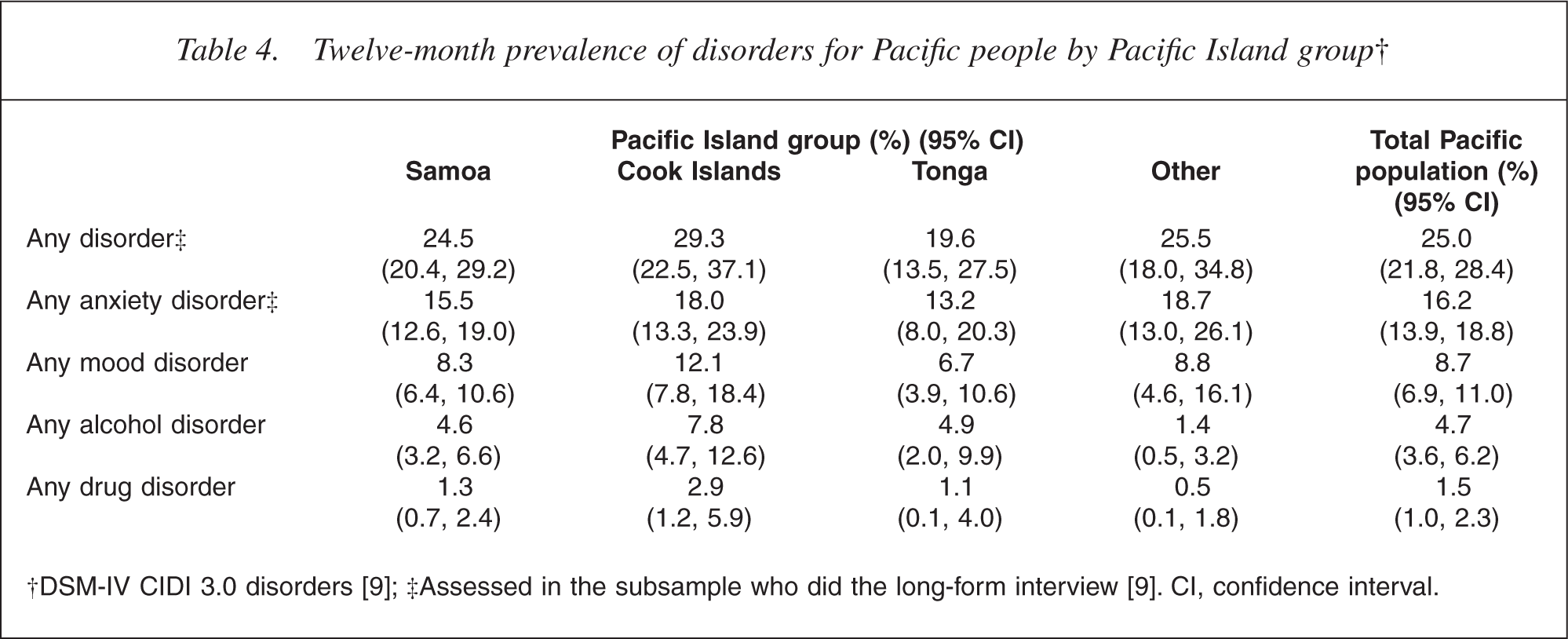
Cook Island Māori have the highest rate (29.3%) of any mental disorder, followed by Other Pacific people (25.5%), Samoans (24.5%) and Tongans (19.6%). The differences between these prevalences are not statistically significant. As many of the confidence intervals are wide and the estimates are imprecise, caution must be used when interpreting Pacific Island groups' prevalences.
Lifetime and 12 month prevalence of suicidal behaviour
The estimated lifetime prevalence of suicidal ideation for Pacific people was 16.9% (Table 5). Pacific females had higher rates of suicidal ideation than Pacific males (19.3% vs 14.3%, p = 0.03). Lifetime suicidal ideation decreases with age, with the group aged 16–24 years having the highest rates of suicidal ideation (p < 0.0001). Overall, the Pacific suicidal ideation rate is similar to that of the total New Zealand population (15.7%; 14.9, 16.6). The difference between the sexes and age is also consistent with the findings for the total New Zealand population [26, 27].
Lifetime and 12 month prevalence of suicidal ideation and suicide attempt among Pacific people, by sex
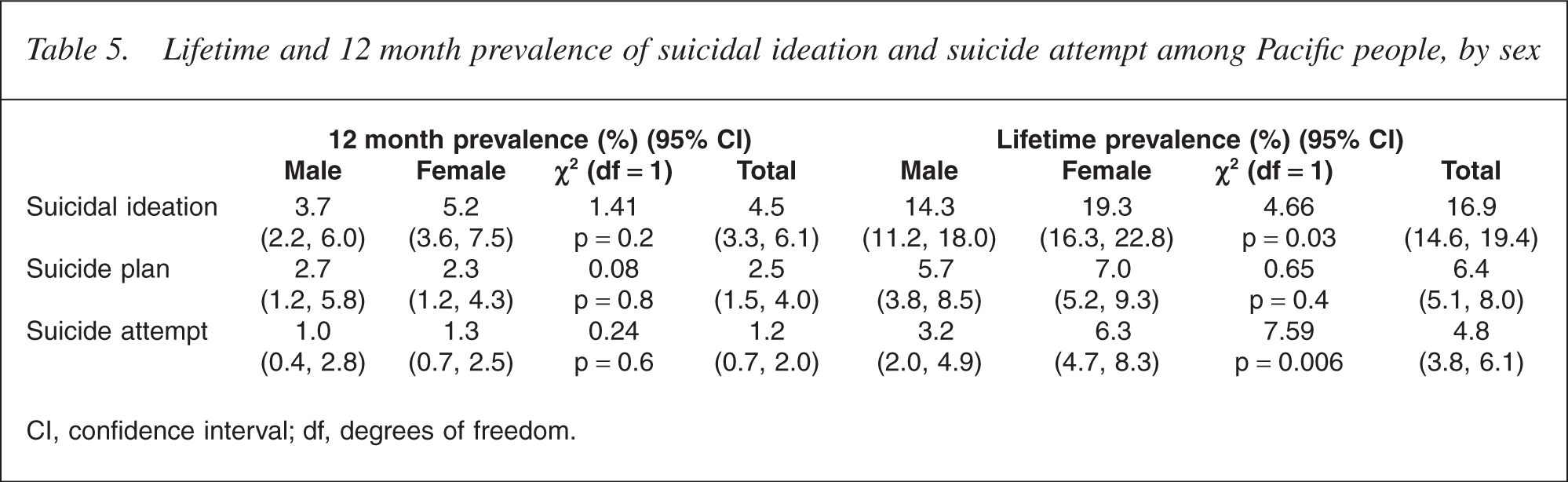
CI, confidence interval; df, degrees of freedom.
The estimated 12 month prevalence of suicidal ideation for Pacific people was 4.5%, with 1.2% having attempted suicide. Again, Pacific females had higher rates of suicidal ideation than Pacific males (5.2% vs 3.7%), although this result was not statistically significant. The highest rate of suicidal ideation was observed in the group aged 16–24 years, which had more than twice the rate of any other Pacific age group (p < 0.0004).
The estimated lifetime prevalence of suicide attempt for Pacific people was marginally higher than the prevalence for the total population (4.8% vs 4.5% [4.1, 5.0]). Consistent with both ideation patterns, Pacific females had a higher prevalence of suicide attempt than Pacific males (6.3% vs 3.2%; p = 0.006) [28].
The estimated 12 month prevalence for suicide attempts was 1.2% for Pacific people, which was three times the rate of the total New Zealand population (0.4%; 0.3, 0.6). The group aged 16–24 years had the highest prevalence of suicide attempt in the previous 12 months (3.1%; 1.5, 6.5), which was five times higher than the age cohort with the next highest rate (25–44 years, 0.6%; 0.32, 1.22). However, age was not shown to have a statistically significant effect on the 12 month prevalence of suicide because of the small numbers of participants who had attempted suicide and the consequent insufficient statistical power to show a statistically significant difference.
Comparisons between Pacific with Māori and Others show that Pacific participants reported significantly higher prevalence than Other (non-Māori) participants of ideation, plan and attempt. In addition, Māori had significantly higher prevalence of suicidal ideation than Pacific participants, whereas Pacific participants had significantly higher prevalence of plans and attempts than Māori participants. However, adjusted estimates suggest that some of these ethnic differences may be sociodemographic in origin. After adjustment for sociodemographic factors, there were no ethnic variations in suicidal ideation. However, Māori and Pacific participants had significantly higher prevalence of making plans and attempts after adjustment for sociodemographic factors [26].
Comorbidity among Pacific people
The term ‘comorbidity’ refers to the co-occurrence of two or more mental disorders, or a mental disorder and a physical disorder, within one individual.
Table 2 shows the proportion of Pacific people with one disorder (16.6%), two disorders (5.1%) and three or more disorders (3.3%) over the past 12 months. Table 6 shows further detail about mental comorbidity among Pacific people in New Zealand. Among those with any mood disorder, 34.9% experienced an anxiety disorder. Among those with any substance use disorder, 27.6% experienced a mood disorder and 41.8% experienced an anxiety disorder.
Percentage of comorbid mental disorder for Pacific people in the past 12 months
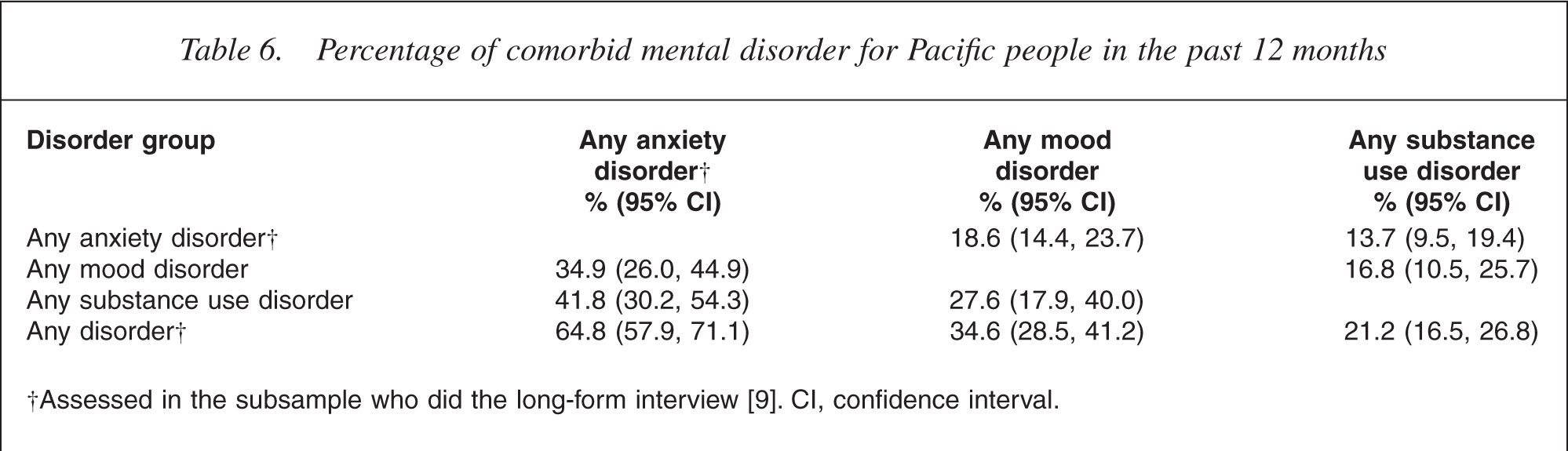
†Assessed in the subsample who did the long-form interview [9]. CI, confidence interval.
Correlates of mental illness
Education and income
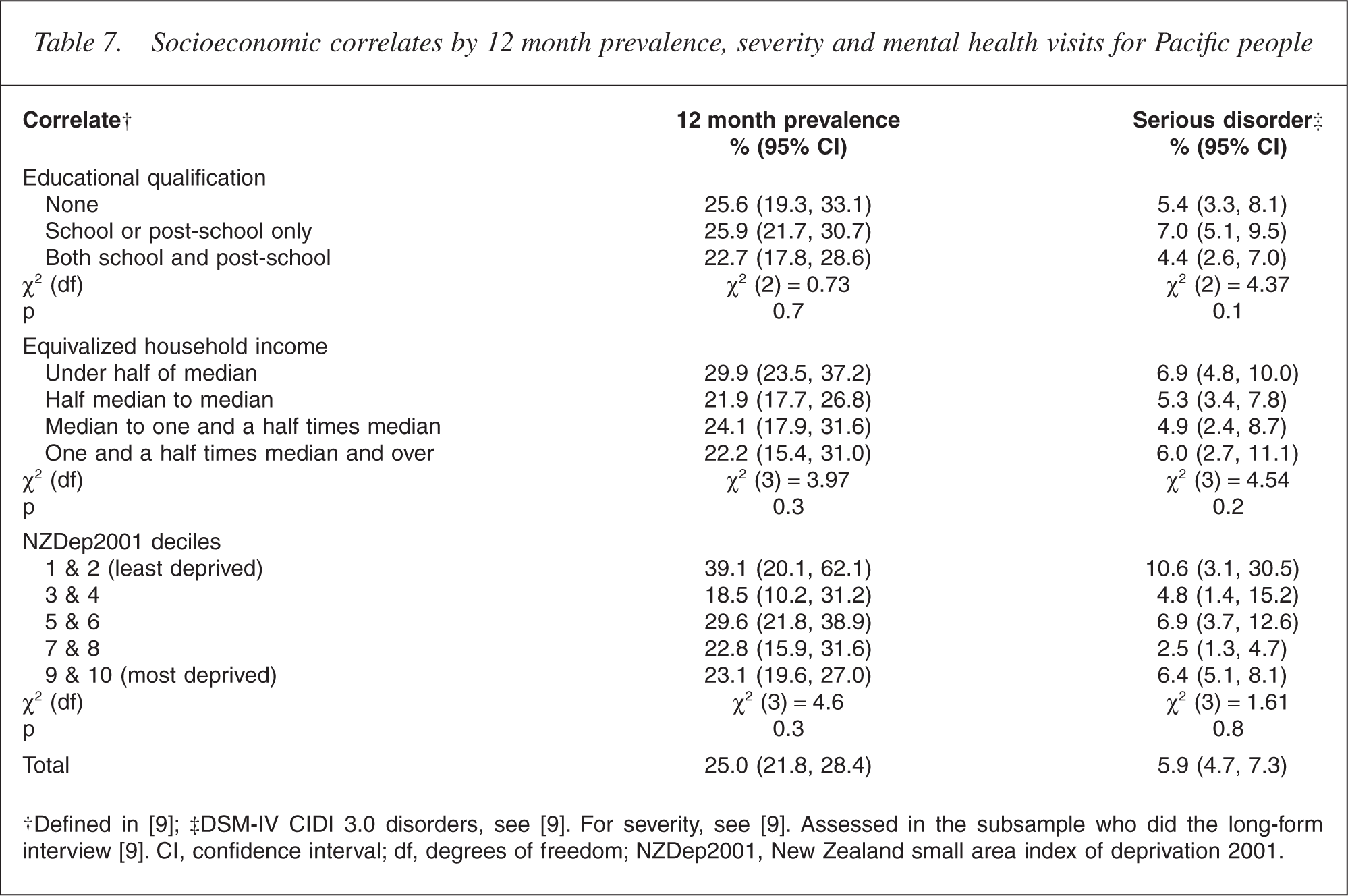
For Pacific people, neither educational qualifications nor equivalized household income had a significant impact on the prevalence (p = 0.4 and p = 0.5, respectively) or severity of mental disorder (p = 0.1 and p = 0.2, respectively) (Table 7). This contrasts with overseas studies that tend to support Australian findings that poorer groups in society experience higher prevalences of mental illness [29]. However, it is indirectly consistent with the results shown below by geographical deprivation.
Socioeconomic correlates by 12 month prevalence, severity and mental health visits for Pacific people
Deprivation
In New Zealand, the use of mental health services has been reported as higher among Pacific people who live in the areas with low NZDep2001 scores (i.e. in relatively less deprived areas). This differs from the total New Zealand population whereby people living in low NZDep2001 areas use fewer mental health services [5].
Table 7 shows that 12 month prevalence rates appear higher among Pacific people living in the areas of low deprivation compared with Pacific people living in the areas of high deprivation, although this result was not statistically significant (p = 0.3).
Migration
Table 8 shows a significant difference between 12 month prevalence rates of Pacific people depending on whether they were born in New Zealand or migrated from the Pacific as children or adults (p < 0.0001). Of New Zealand-born Pacific people, 31.4% had a mental disorder in the past 12 months compared with 15.1% of Pacific people who migrated at age 18 years and over. Age at the time of migration was significantly related to the prevalence of serious disorder; 6.7% of New Zealand-born Pacific people compared with 3.7% of Pacific people who migrated at age 18 years and over had a serious mental disorder (p = 0.01).
Twelve-month prevalence, severity and treatment of disorders age at migration for Pacific people
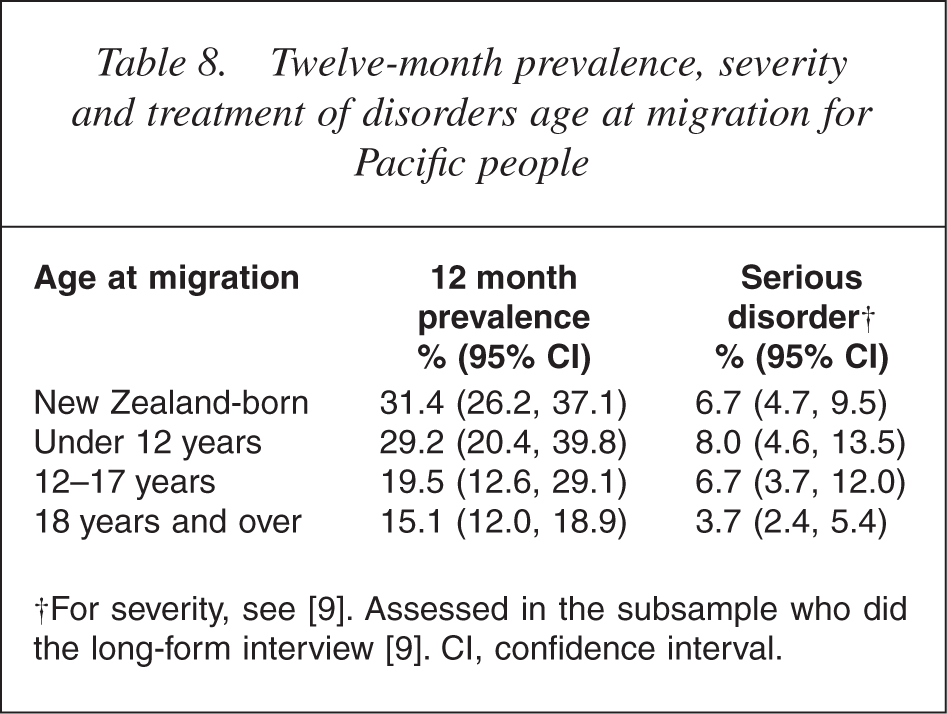
A strong relationship existed between age at interview and age at migration: almost all (93.6%) of the New Zealand-born population were aged under 45 years compared with 47.1% of those who had migrated at age 18 years and over. Nonetheless, adjustment for age and sex had little impact on the prevalences reported for age at migration [28, table 11.1] and no effect on the pattern of results. Age at migration and time since migration were also related and in a joint analysis of any disorder in the past 12 months, age at migration remained influential while time since migration did not. This indicates that age at migration is the more important correlate.
Health service use
Only small differences existed between Pacific people and the total New Zealand population with regard to the prevalence of serious mental disorder (5.9% vs 4.7% [4.2, 5.2])[28]. However, Pacific people with the most serious disorders were less likely to have a mental health visit, that is, they were less likely to visit any health service for a mental health reason.
Table 9 shows that 25.0% of Pacific people who had experienced a serious mental disorder had a mental health visit compared with 58.0% (53.3, 62.6) of the total New Zealand population [8, 9, 22, 30]. Of Pacific people who had experienced a moderate mental disorder, 26.5% had a mental health visit compared with 36.5% (32.9, 40.4) of the total New Zealand population.
Severity, days out of role and percentage with a mental health visit in the past 12 months for Pacific people
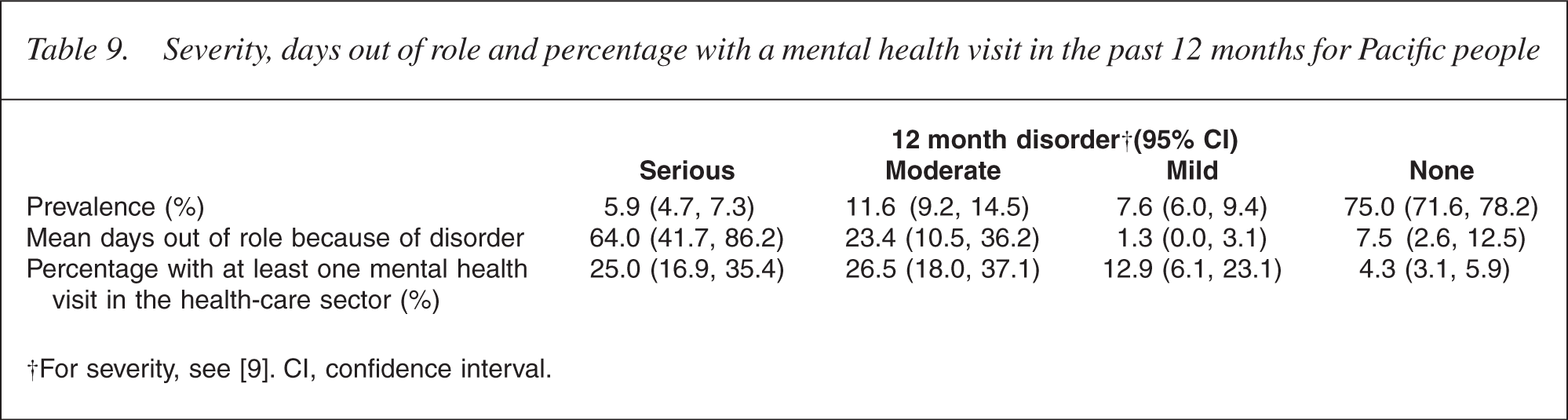
†For severity, see [9]. CI, confidence interval.
The lower estimates of Pacific people receiving treatment for severe and moderate mental disorders support documented evidence showing that the rate of Pacific people in New Zealand receiving treatment was 35% lower than the rate for the total New Zealand population [5].
When comparing across Pacific, Māori and Other (i.e. non-Māori non-Pacific) ethnic groups for any visit for a mental health reason, significant differences exist across the three ethnic groups [24]. Without adjustment, 25.4% (19.4, 31.4) of Pacific people with a disorder made a mental health visit compared with 32.5% (28.3, 36.7) of Māori and 41.1% (38.1, 44.1) of Others. Adjustment by age and sex alone or by age, sex, educational qualification and equivalized household income leads to minimal changes in these percentages and no change in the significance of the difference between them. This means that, unlike the pattern for prevalence, some reason exists for Pacific people not using health services for mental health reasons that is not accounted for by the Pacific population structure.
Table 10 compares the services used by Pacific people with and without a disorder. It also shows that Pacific people with a serious disorder, in spite of having almost three times the number of days lost because of a disorder, were no more likely to use health services than Pacific people with a moderate disorder.
Prevalence of 12 month mental health service use in separate service sectors by 12 month anxiety, mood, substance use and eating disorders for Pacific people
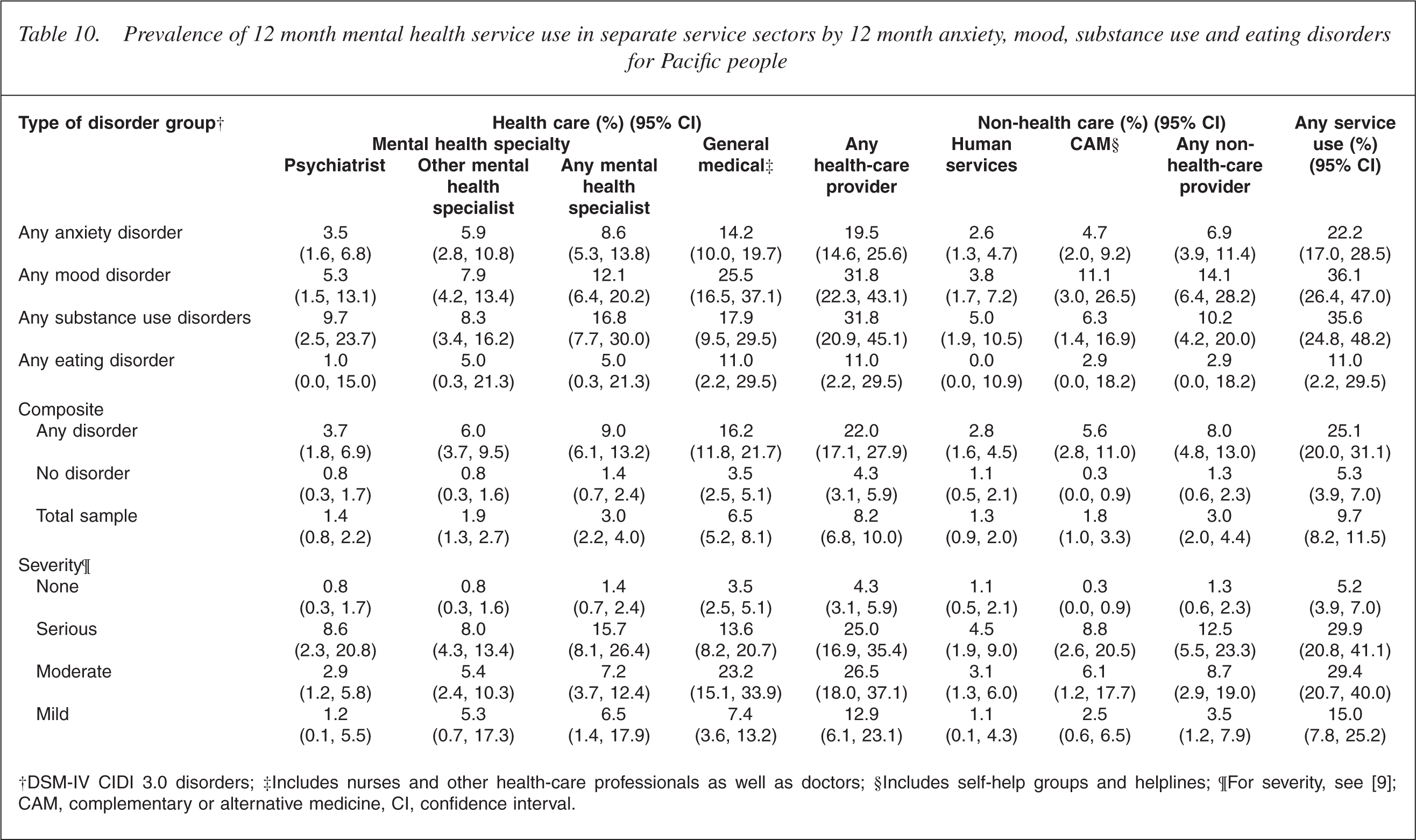
†DSM-IV CIDI 3.0 disorders; ‡Includes nurses and other health-care professionals as well as doctors; §Includes self-help groups and helplines; ¶For severity, see [9]; CAM, complementary or alternative medicine, CI, confidence interval.
Discussion
The NZMHS is the first major epidemiological survey able to generate specific information about the mental health of Pacific people in New Zealand. The survey incorporated a high level of Pacific involvement in the study design and implementation. Importantly, it also oversampled Pacific participants, which enabled the participation of sufficient numbers of Pacific people to provide estimates of acceptable precision.
Before this survey, very little information existed about the prevalence of mental disorders among Pacific peoples. The NZMHS has provided some landmark findings for Pacific people.
First, the NZMHS has demonstrated that Pacific people experience some mental disorders at higher levels than the general population. This is particularly signifi-cant as it is contrary to previously held beliefs that Pacific people experience relatively low levels of mental illness. As reported, the unadjusted 12 month prevalence for Pacific people was 23.9% compared with 19.2% for the Other composite ethnic group [28, 31]. The large number of Pacific young people, however, has a marked influence on the increased prevalence of mental disorder in Pacific people.
In addition, the NZMHS has provided evidence that Pacific people have higher prevalences of suicidal ideation, suicide plans and suicide attempts than the Other composite ethnic group. The difference remains for plans and for attempts, although not for ideation, after adjusting for sociodemographic correlates.
The NZMHS showed that Pacific people classified as experiencing a serious disorder significantly underutilize health services for a mental health reason (25.0% of Pacific vs 58.0% for the total New Zealand population). Underutilization of existing services, especially by those Pacific people with serious mental disorders, has significant implications for the mental health sector. The acceptability of existing mental health services, availability of appropriate services, provider fit with need and other issues of accessibility for Pacific people are a few of the possible explanations. However, further studies are required to explore the reasons behind this significant finding.
The NZMHS raises interesting questions about the position of New Zealand-born Pacific people in relation to migrant Pacific people. The results suggest that early exposure to the New Zealand environment may be associated with higher levels of mental disorder among Pacific people. There is generally a need for better understanding of the underlying protective and risk factors for mental health and mental illness among Pacific populations.
The NZMHS did not support, for Pacific people, the international literature's finding that social adversity (associated with migration) is linked to increased risk for mental disorder. Analysis of the effects of migration showed that older migrants tended to have lower rates of mental illness compared with New Zealand-born Pacific people.
In conclusion, the NZMHS provides previously unavailable information about mental disorder in relation to Pacific people in New Zealand. This information may be used to inform policy development and provides a platform for further research.
Footnotes
Acknowledgements
Te Rau Hinengaro: The New Zealand Mental Health Survey was funded by the Ministry of Health, Alcohol Advisory Council and Health Research Council of New Zealand. The survey was carried out in conjunction with the World Health Organization World Mental Health Survey Initiative. We thank the WMH staff for assistance with instrumentation, fieldwork and data analysis. These activities were supported by the US National Institute of Mental Health (R01MH070884), the John D and Catherine T MacArthur Foundation, the Pfizer Foundation, the US Public Health Service (R13-MH066849, R01-MH069864, and R01 DA016558), the Fogarty International Center (FIRCA R01-TW006481), the Pan American Health Organization, Eli Lilly and Company, Ortho-McNeil Pharmaceutical, Inc., GlaxoSmithKline, and Bristol-Myers Squibb. The WMH publications are listed at ![]() .
.
Other members of the Te Rau Hinengaro Research Team are M Oakley-Browne, JE Wells, M McGee, J Baxter, TK Kingi, R Tapsell, MH Durie, KM Scott and C Gale.
We particularly acknowledge the input by the Pacific Advisory Group: Fuimaono Karl Pulotu-Endemann, Francis Agnew, Vito Malo, Reverend Feiloaiga Tauleale-ausumai, Hemiquaver Lesatele, Lina-Jodi Vaine Samu Tuiloma and Sefita Hao'uli.
We thank the Kaitiaki Group for their input and support for this survey and we thank all the participants.