
Abstract
Te Rau Hinengaro: The New Zealand Mental Health Survey (NZMHS) is the first population survey using standardized mental health diagnostic measures that has included a representative sample of Māori, the indigenous people of New Zealand, spanning all adult ages. A total of 2595 Māori participated in interviews as part of the study. This paper focuses on the prevalence and pattern of 12 month and lifetime disorder among Māori.
Māori comprise 15% of the New Zealand population. Over recent decades, there has been increasing concern about the mental health of Māori, particularly among young Māori [1–4]. Part of this concern stems from analysis of routinely collected hospitalization data, describing rates and patterns of hospitalization for psychiatric disorders. Analyses of hospital inpatient data show that before 1970, rates of admission to psychiatric hospitals were lower for Māori than for non-Māori [5]. However, patterns of admissions during the 1980s and 1990s show increased rates of psychiatric hospitalization for Māori, especially among young Māori, and particularly for substance use disorders, schizophrenia and bipolar disorder [3, 4, 6]. Analyses note differing patterns of sources of referral for admission, with Māori being more likely to be hospitalized through a ‘justice’ doorway than a primary care entry point.
More recent analyses of the Mental Health Information National Collection [7] and from the Mental Health Classification and Outcomes Study [8] are consistent with earlier analyses and show continued high rates of contact within the mental health sector (both inpatient and community) among Māori.
Although health service data provide important information, particularly about serious mental disorders, these data do not accurately reflect mental health need within a population. There has been limited research into the mental health of Māori within a community setting, including research on the prevalence and pattern of more common mental health problems that may not lead to hospitalization or secondary care. The Mental Health and General Practice Investigation study measured mental disorders in adults attending primary health care and found that Māori attendees, particularly Māori women, had higher rates of mental disorder than non-Māori. Rates were higher for all common mental disorders (anxiety, depression and substance abuse). These findings persisted even when differences in age and socioeconomic status were taken into account [9, 10]. Using standard diagnostic instruments, a Christchurch-based birth cohort study, the Christchurch Health and Development Study, found that the prevalence of mental disorders among a youth cohort at age 18 years was high. Fifty-five per cent of Māori included in the cohort study met criteria for at least one mental disorder within the previous 3 years compared with 41% of non-Māori youth in the cohort [11]. Rates for substance use disorders were especially high with over 33.9% of young Māori having a substance disorder.
The New Zealand National Prison Study was a study of 1287 prisoners conducted in 1997/98. It revealed high levels of mental disorder among both Māori and non-Māori inmates [12, 13]. A paper reporting ethnicity comparisons from the survey found no differences in the prevalence of individual mental disorders among Māori, Pacific and European/Other ethnic groups [14]. Despite a similar prevalence of mental disorders, treatment for mental disorders (past and current) was less common among Māori and Pacific inmates than among European/ Other inmates.
Rates of suicide provide further foundation for concern about Māori mental health. Before the 1980s, Māori suicide rates were lower than those for non-Māori. However, Māori suicide rates increased markedly over the 1980s and 1990s, and disparities between Māori and non-Māori have emerged, particularly among the young [15, 16].
The evidence thus suggests comparatively high levels of mental health need among Māori. However, many gaps in knowledge remain. The NZMHS thus provides information on the mental health of Māori from a population health perspective. This paper describes the 12 month and lifetime prevalence of mental disorders in Māori and the prevalence of comorbid and serious disorders. Disparity between ethnic groups is reported in other papers [17–19] and further analyses, including Māori contact with services for mental disorder, are planned for future papers.
Method
Sample
The NZMHS was a nationally representative household survey of people aged 16 years and over using face-to-face interviews, and was carried out between 2003 and 2004. Ethnicity was determined using the ethnicity question from the 2001 New Zealand census. Participants were asked to identify the ethnic group(s) they belonged to; this allowed reporting of multiple ethnicities. The Statistics New Zealand prioritization rule for ethnicity assignment was followed. This rule classifies those who identify solely as Māori along with those who identify Māori as one of their ethnic groups (when there are more than one) as Māori. Those who self-identify as any Pacific Island group, but not Māori, are defined as Pacific. To achieve reasonably precise estimates, Māori and Pacific populations were oversampled relative to their proportions within the population, using a mixture of targeting and screening. Using this method, the number of Māori doubled and the number of Pacific people quadrupled. The total sample consisted of 12 992 completed interviews, 2595 (20.0%) from Māori and 2236 (17.2%) from Pacific people (138 reported both Māori and Pacific ethnicity and were counted as Māori under standard prioritization rules).
The response rate was 73.3%. There is no straightforward way to calculate a Māori response rate. Although ethnicity was known for everyone interviewed, ethnicity was not known for non-participants in the High Pacific Stratum or the General Stratum main sample. Therefore, while the numerator for a Māori response rate was known, it was not possible to determine ethnic specific denominators.
The interview consisted of two parts. Part 1 included core diagnostic sections and sections on suicidal behaviour, health services use and demographics and was administered to everyone (n =12 992). Part 2 consisted of additional diagnostic sections and other measures of mental and physical health and was administered to a subsample (n =7435). All participants who met certain criteria in the Part 1 diagnostic sections received the long form of the interview. A probability subsample of other participants also received the long form [19, figure 1]. The survey methods are described in detail in [19, 20].
Diagnostic assessment
The interview included diagnostic sections from version 15 of the World Mental Health Composite International Diagnostic Interview (WMH-CIDI) [21], the CIDI 3.0. This is a fully structured lay interview that generates diagnoses according to ICD-10 [22] and DSM-IV [23]. Only DSM-IV diagnoses are reported here. The CIDI 3.0 asks if symptoms have ever occurred and then asks about recency. Twelve-month disorder is diagnosed if full criteria for disorder have ever been met and there have been symptoms or an episode in the past 12 months. Full criteria may not have been met in the past 12 months.
The disorders groups measured include:
Anxiety disorders: panic disorder, agoraphobia without panic, specific phobia, social phobia, generalized anxiety disorder, posttraumatic stress disorder, obsessive-compulsive disorder
Mood disorders: major depressive disorder, dysthymia, bipolar disorder (I, II, and any with mania or hypomania)
Substance disorders: alcohol abuse, alcohol dependence, drug abuse, drug dependence, and within drug disorders
Eating disorders: anorexia, bulimia
Severity
Severity for a case was based on all disorders experienced in the past 12 months. Definitions used in New Zealand were those developed for the first WMH cross-national paper [24] except for substance dependence for which the National Comorbidity Survey Replication [25] definition was used [19]. Serious disorder was defined as one of the following: an episode of bipolar I disorder, substance dependence with serious role impairment (two effects experienced ‘a lot’), a suicide attempt and any WMH-CIDI/DSM-IV disorder, at least two areas of severe role impairment as a result of a mental disorder in the Sheehan Disability Scale domains, overall functional impairment at a level found in the National Comorbidity Survey Replication to be consistent with a Global Assessment of Functioning [26] score of 50 or less in conjunction with a WMH-CIDI/DSM-IV disorder. Participants with disorder who were not classified as serious were classified as moderate if interference was reported as at least moderate in any Sheehan Disability Scale domain or if they had substance dependence without substantial impairment. All other participants with disorder were classified as mild.
Correlates
Sociodemographic correlates include age at interview, sex, prioritized ethnicity, educational qualifications and equivalized household income. Educational qualifications were assessed using 2001 census questions about school and post-school qualifications. Household income was missing for 13.0% of respondents and was imputed by linear regression. A modification of the revised Jensen equivalence scale for household income [27] was used to take account of the number of adults and the number of children in the household.
Analyses
Data were weighted to account for different probabilities of selection that arose from oversampling Māori and Pacific people and the selection of one person per household, differential non-response, and residual differences in age, sex and ethnicity between the sample and the 2001 census population. Additional weights were used to account for selection into the long-form sections of the interview. Logistic regression analyses were carried out in SUDAAN 9.0.1, which takes account of the complex sample design.
Cultural integrity
A team of Māori researchers from Auckland, Massey and Otago universities with experience in mental health research and Māori health research provided input into all phases of the research, including design, survey, analysis and report writing. In addition, the Māori research team oversaw those sections of the questionnaire that focused on Māori identity and Māori use of health services. An important methodological task was to ensure the research was consistent with both tikanga Māori (Maori culture and practice) and scientific paradigms.
A kaitiaki group (guardian group) was established to provide cultural guardianship over the research. It developed processes to safeguard the information collected and minimize any risks to participants.
While this survey adopted the ethnicity question from the 2001 census, it also included questions for those of Māori descent, so cultural identity could be investigated with greater levels of meaning. The key items in this Māori section of the survey included selfidentification, ancestry, tribal knowledge, marae participation, whānau (extended family) involvement, and te reo Māori (Māori language) proficiency. These questions were derived from three main sources: Te Hoe Nuku Roa (a longitudinal study of Māori households) [28]; the 2001 Health of the Māori Language Survey [29]; and consultations with various interest groups (e.g. representatives from the Ministry of Health, the Kaitiaki Group, Māori researchers and academics, and Māori language experts).
Results
Characteristics of Māori participants by sociodemographic correlates
Table 1 shows the characteristics of Māori participants, weighted and unweighted, across sociodemographic correlates including sex, age, social and economic measures, and locality variables.
Profile of Māori participants by sociodemographic correlates
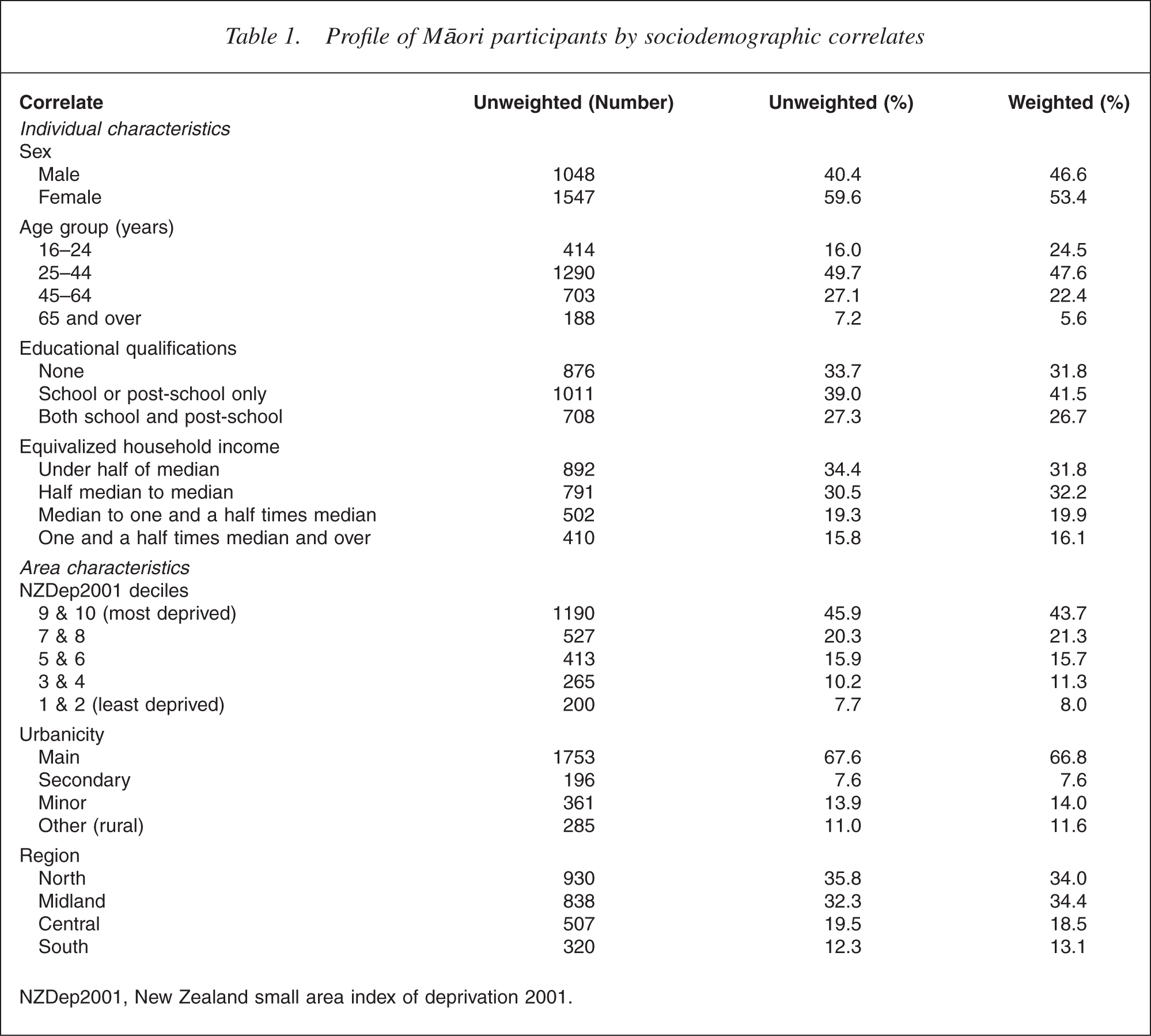
NZDep2001, New Zealand small area index of deprivation 2001.
A higher proportion of Māori participants were female, which is consistent with the overall survey profile where more females participated. A higher proportion of Māori participants were in the younger age groups. Māori were proportionately less likely to have post-school qualifications and were more likely to have low equivalized household income and be living in areas of high relative deprivation. Māori were also proportionately more likely to be urban and living in the north and midland regions. These are consistent with Māori population demographics.
Characteristics of Māori participants by Māori cultural and participation variables
Table 2 shows the profile of Māori based on selected Māori cultural and participation variables. Findings are described for the weighted sample.
Profile of Māori participants by selected cultural variables
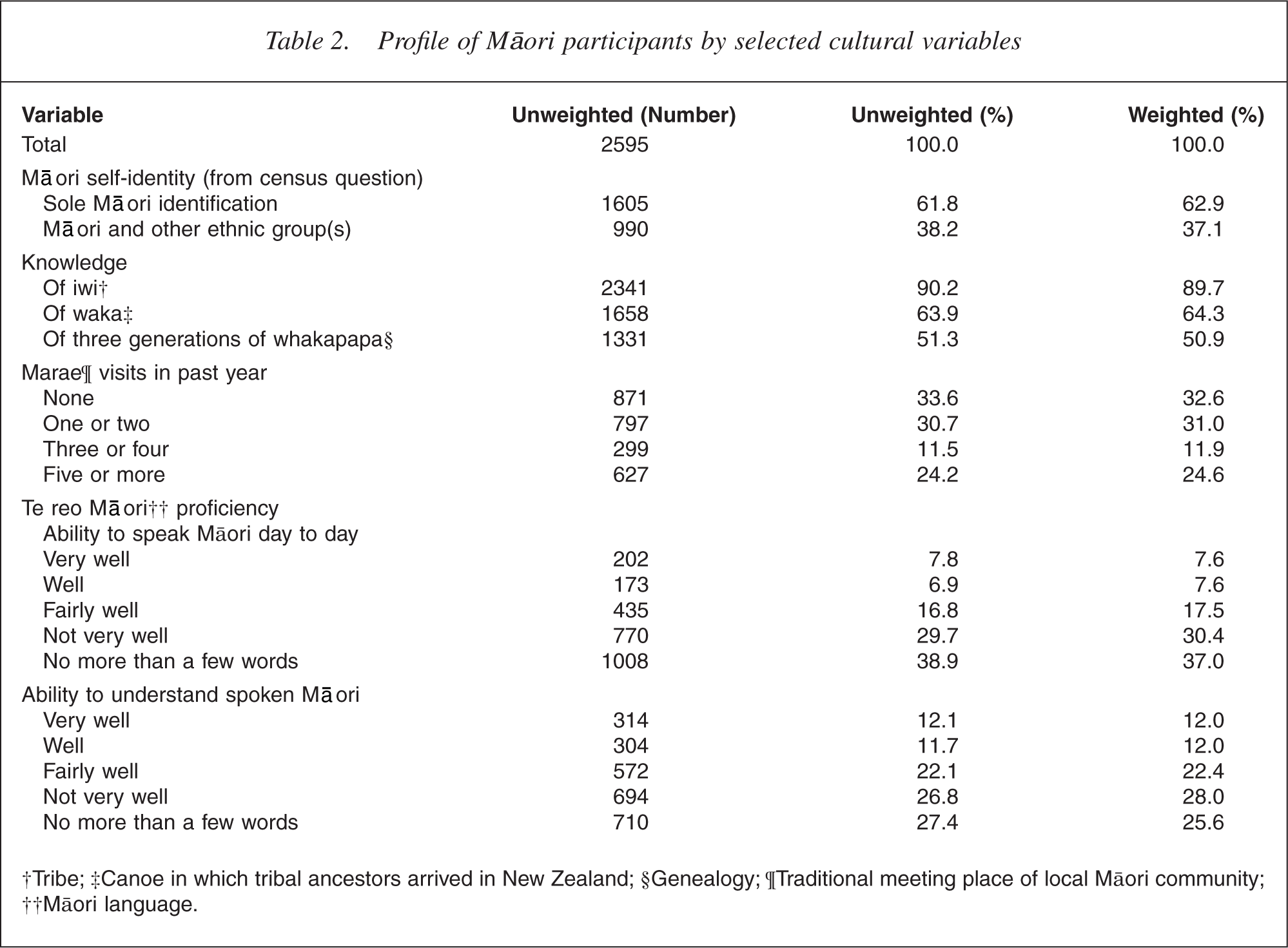
†Tribe; ‡Canoe in which tribal ancestors arrived in New Zealand; §Genealogy; ¶Traditional meeting place of local Māori community; ††Māori language.
The table shows that almost two-thirds of Māori (62.9%) identified their ethnicity solely as Māori and just over one-third (37.1%) identi-fied as Māori in addition to another ethnic group or groups. Most (89.7%) Māori knew their iwi (tribe), almost two-thirds (64.3%) knew their waka (the canoe in which tribal ancestors arrived in New Zealand) and half (50.9%) could name three generations of whakapapa (genealogy).
The degree of contact with marae varied from one-third of Māori (32.6%) having no visits to a marae in the past year to one quarter (24.6%) having five or more visits. Te reo Māori (Māori language) was spoken very well by 7.6%, well by 7.6%, fairly well by 17.5%, and not very well by 30.4%, with no more than a few words spoken by 37.0%. A greater proportion of Māori could understand te reo Māori.
Prevalence of mental disorders in Māori
Period prevalence of mental disorders and multiple disorders across aggregated data
Table 3 shows the prevalence of mental disorders and multiple disorder in Māori, across their lifetime, within the past 12 months and over the past month.
Lifetime, 12 month and 1 month prevalences of mental disorder groups and multiple disorders among Māori
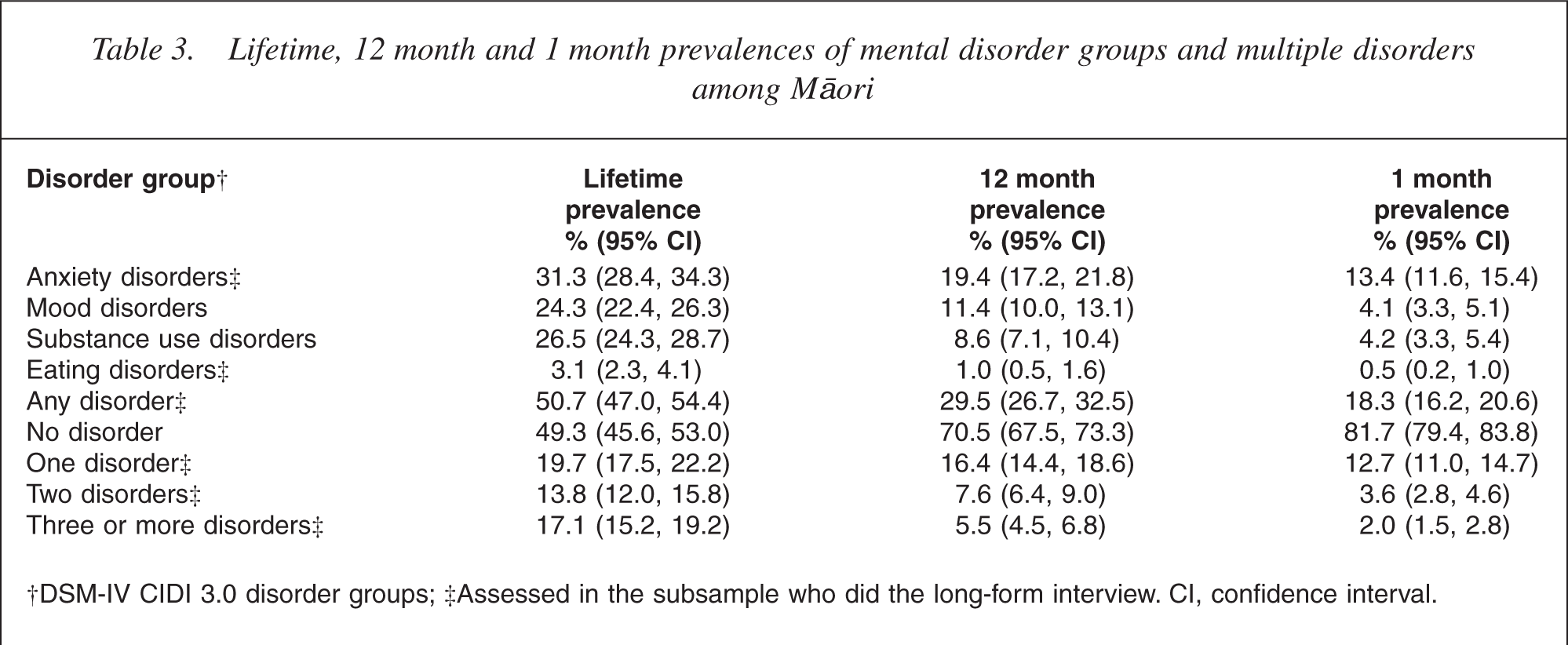
†DSM-IV CIDI 3.0 disorder groups; ‡Assessed in the subsample who did the long-form interview. CI, confidence interval.
Half (50.7%) of Māori experienced at least one disorder in their life before the interview. At least one disorder was experienced by 29.5% of Māori in the past 12 months and 18.3% of Māori in the past month. The most common lifetime disorders were anxiety (31.3%), substance use (26.5%) and mood (24.3%) disorders. Anxiety disorders (19.4%) were also the most common 12 months disorders, followed by mood (11.4%) and substance use (8.6%) disorders. Over the past month, the most common disorders were anxiety (13.4%), substance (4.2%) and mood (4.1%) disorders.
Levels of lifetime comorbidity were high, with 19.7% of Māori with one disorder, 13.8% with two disorders and 17.1% with three or more disorders. Over the past 12 months, 16.4% of Māori had one disorder, 7.6% had two disorders and 5.5% had three or more disorders.
Eating disorders were not common (a lifetime prevalence of 3.1%).
Prevalence of individual disorders: lifetime and 12 month prevalences
Table 4 shows the prevalence of individual mental disorders in Māori over their life until the interview and in the 12 months before the interview.
Lifetime and 12 month prevalence of individual disorders for Māori
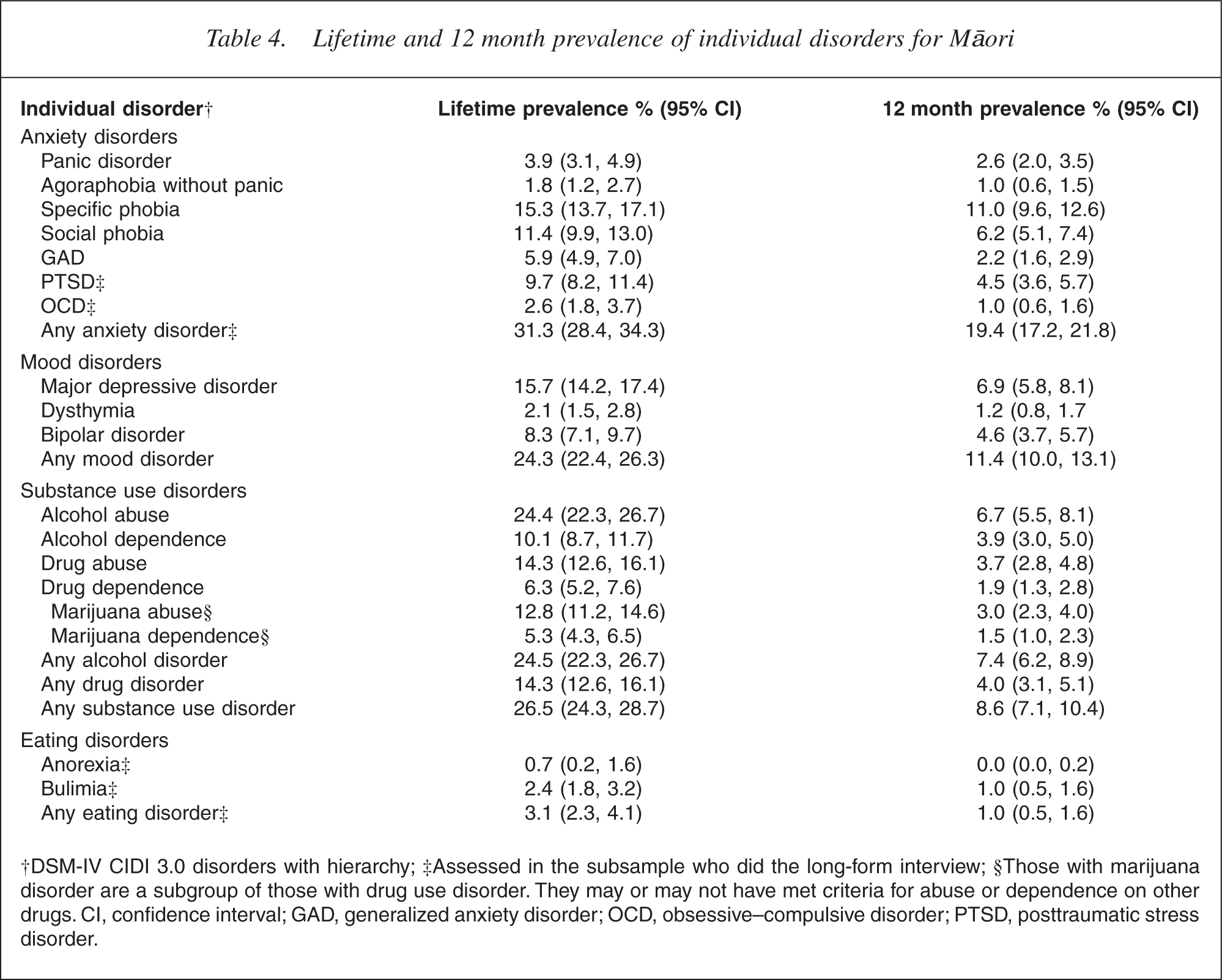
†DSM-IV CIDI 3.0 disorders with hierarchy; ‡Assessed in the subsample who did the long-form interview; §Those with marijuana disorder are a subgroup of those with drug use disorder. They may or may not have met criteria for abuse or dependence on other drugs. CI, confidence interval; GAD, generalized anxiety disorder; OCD, obsessive–compulsive disorder; PTSD, posttraumatic stress disorder.
Anxiety disorders were the most prevalent disorder group in Māori (lifetime prevalence 31.3%; 12 month prevalence 19.4%). Specific phobia, social phobia and posttraumatic stress disorder were the most common anxiety disorders in Māori over both periods.
Around one in four Māori (24.3%) had a lifetime mood disorder, the most common lifetime mood disorders being major depressive disorder (15.7%) followed by bipolar disorder (8.3%). Over the 12 months before interview, mood disorder were experienced by over one in 10 Māori (11.4%), with major depressive disorder the most common (6.9%) followed by bipolar disorder (4.6%). Dysthymia was less common.
Over one in four (26.5%) Māori experienced a substance disorder in their life before the interview. Alcohol disorders were most prevalent (24.5%) followed by drug disorders (14.3%). Findings suggest that marijuana disorders (which are a subgroup of drug disorders) contribute strongly to the overall drug disorder prevalence in Māori, with lifetime marijuana abuse in 12.8% of Māori and marijuana dependence in 5.3%. The 12 month prevalence of substance disorder among Māori was 8.6%, with alcohol disorders most prevalent (7.4%), followed by drug disorders (4.0%). Marijuana abuse was prevalent in 3.0% and marijuana dependence in 1.5%.
Twelve-month disorders: prevalence by sociodemographic correlates
Table 5 describes findings for the prevalence of 12 month disorder in Māori, by demographic, social and economic variables. Mental disorders were more common among Māori females, with mental disorders prevalent in one-third of Māori females (33.6%) and one quarter of Māori males (24.8%). Mental disorders were also more common in younger age groups, with one in three (33.2%) aged 16–24 years and one in three (32.9%) aged 25–44 years experiencing a 12 month disorder compared with one in four (23.7%) aged 45–64 years and one in eight (7.9%) aged 65 years and over.
Sociodemographic correlates of 12 month prevalence of mental disorders in Māori
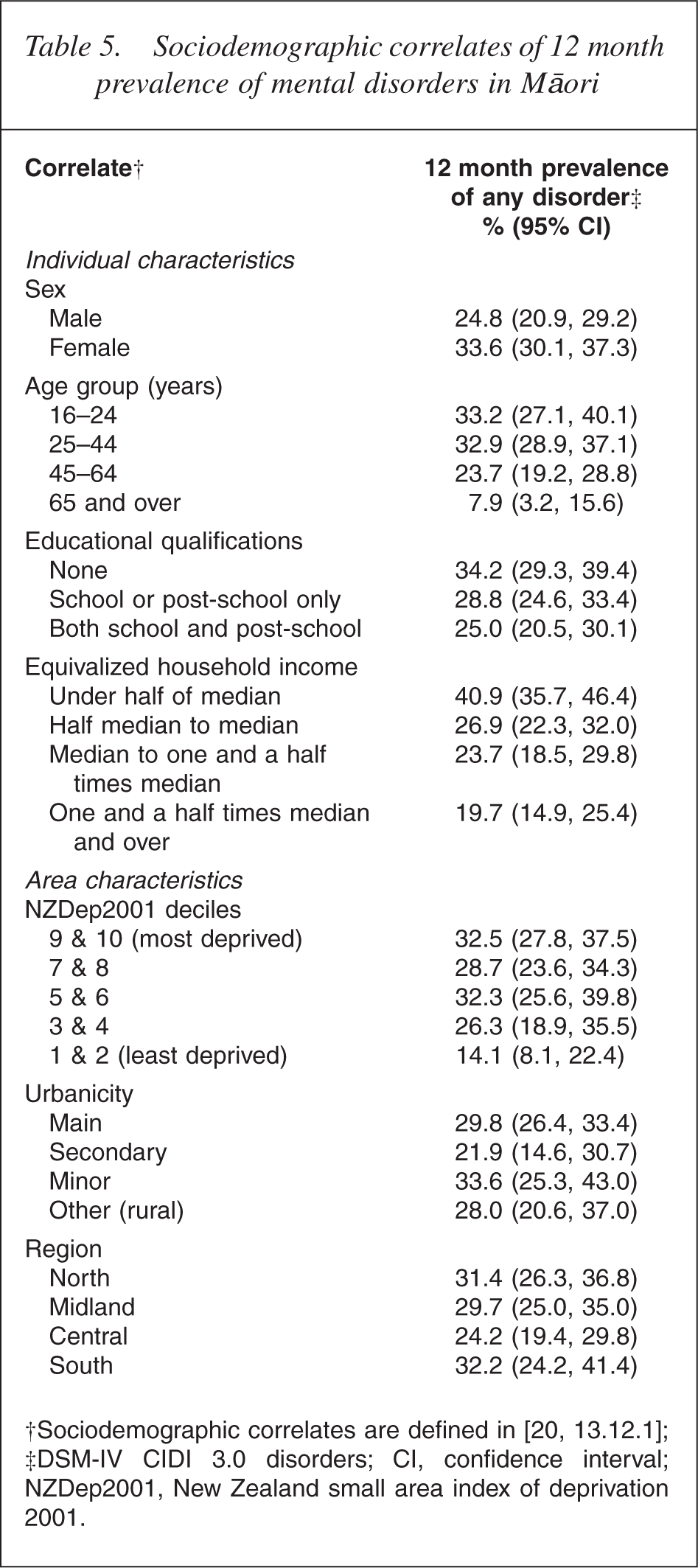
†Sociodemographic correlates are defined in [20, 13.12.1]; ‡DSM-IV CIDI 3.0 disorders; CI, confidence interval; NZDep2001, New Zealand small area index of deprivation 2001.
The prevalence of disorder was highest in Māori with an equivalized household income under half of median (40.9%) and lowest in Māori with an equivalized household income one and a half times median and over (19.7%). Māori living in least deprived areas (deciles 1 and 2 of the New Zealand small area index of deprivation) had the lowest rates of disorder, but only a small difference existed in rates between those in deprivation deciles 3–10. Minor differences exist for disorders based on the level of urbanicity. However, these differences are not significant statistically. This is true also for region. Findings show that the 12 month prevalence of disorder was highest among Māori in the southern region (32.2%) and lowest among Māori in the central region (24.2%). However, the overlap of confidence intervals indicates that differences are not significant statistically.
Severity of aggregated disorders in Māori
Table 6 shows the prevalence of 12 month disorders by their severity (serious, moderate or mild). Of Māori with any mental disorder, 29.6% had serious disorders, 42.6% had moderate disorders and 27.8% had mild disorders. This pattern of severity was similar for anxiety and substance use disorders. Of Māori with anxiety disorders, 33.3% had a serious disorder and 40.9% had a moderate disorder. For substance use disorders, 33.5% of Māori with a substance use disorder had a serious disorder and a slightly higher proportion (40.6%) had a moderate disorder. The pattern differed for mood disorder with 51.4% of all Māori with a mood disorder having a serious disorder. Eleven per cent of Māori with a mood disorder were considered to have a mild disorder.
Twelve-month prevalence of mental disorders among Māori, by severity
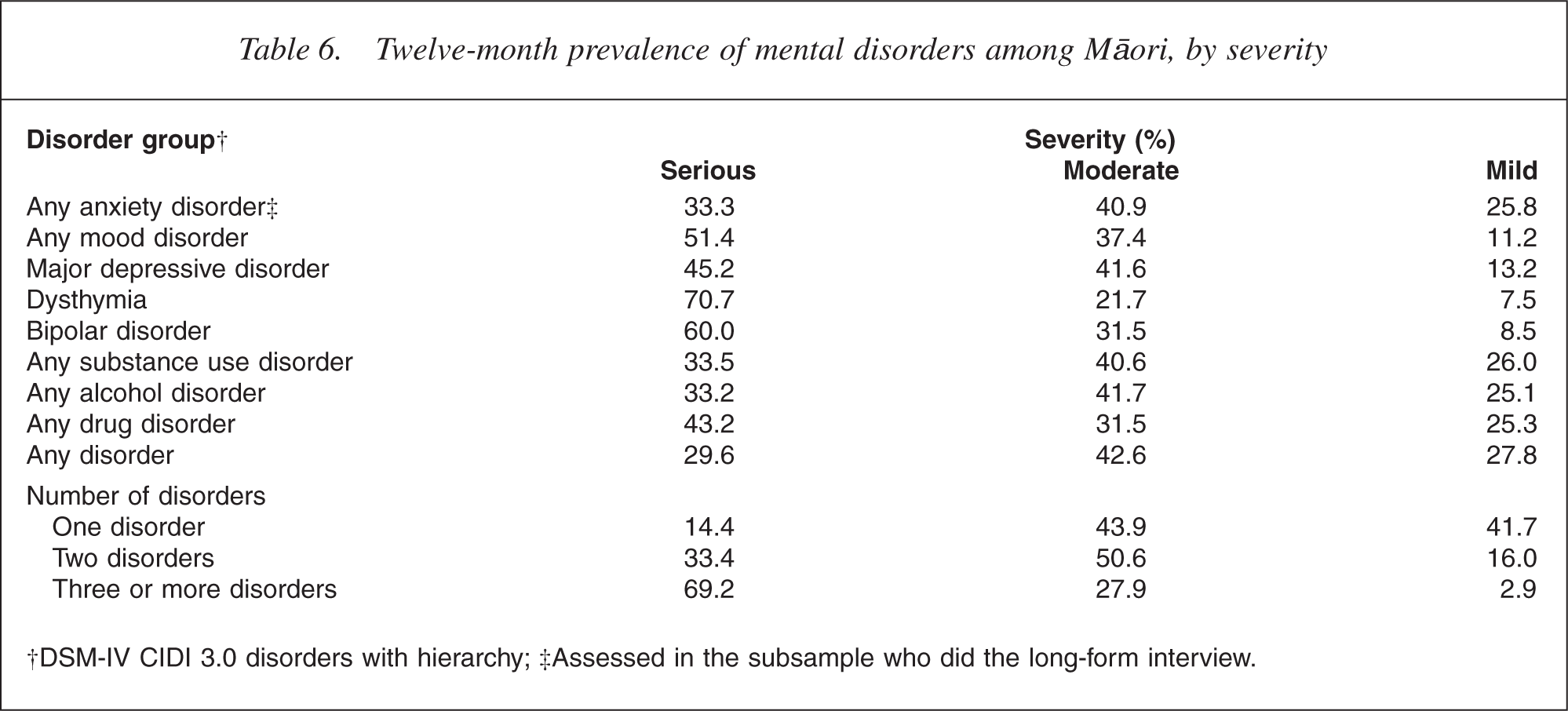
†DSM-IV CIDI 3.0 disorders with hierarchy; ‡Assessed in the subsample who did the long-form interview.
The severity of disorder is strongly associated with the number of disorders. Of Māori with three or more disorders, 69.2% were considered serious, whereas 14.4% with one disorder were considered serious.
Discussion
The NZMHS is the first population survey of mental disorders in a representative population of Māori adults aged 16 years and over. This paper presents results from the NZMHS for the prevalence of mental disorder among Māori. Further results for Māori are presented in the report of the survey [30] and additional findings will be presented in future papers. A description of ethnicity comparisons for the 12 month prevalence of disorder and health service contact is presented in [17].
Mental disorders, as defined and measured in the NZMHS, are common, with at least half (50.7%) of Māori experiencing at least one disorder over their life before interview and almost one-third (29.5%) of Māori with at least one disorder in the previous 12 months. These findings are consistent with evidence from the Mental Health and General Practice Investigation study of relatively high prevalence of common mental disorders among Māori general practice attendees.
Anxiety disorders were the most common in Māori (lifetime 31.3%; 12 month 19.4%). Three disorders (specific phobias, social phobias and posttraumatic stress disorder) made up most of this prevalence. Findings for severity (Table 6) show that among Māori with 12 month anxiety disorders, 33.3% were considered serious and 40.9% were moderate, suggesting anxiety disorders are not only common but have considerable impact. There is little research investigating the nature and extent or impact of anxiety disorders in Māori adults. Further attention to anxiety disorders among Māori is needed within research and within the health sector response to Māori mental health.
Mood and substance disorders were also common. Although depression was most common (lifetime 15.7%; 12 month 8.3%), the prevalence of bipolar disorder was unexpectedly high (lifetime 8.3%; 12 month 6.9%). This finding is concerning and warrants more investigations. Further analyses of bipolar disorder are planned for future papers.
Findings for substance use disorders among Māori align with background evidence. Among substance use disorders, alcohol disorders were the most prevalent (lifetime 24.5%; 12 month 8.6%). Drug disorders were also common (lifetime 14.3%; 12 month 4.0%) and consisted predominantly of marijuana abuse and dependence disorders. Alcohol and drug disorders (particularly marijuana abuse and dependence) remain important physical and mental health concerns among Māori, and findings show that a high proportion of Māori with substance disorders were serious (33.5%) or moderate (40.6%) in severity.
Although eating disorders were not common, they are occurring in Māori.
Results for severity show that many Māori with 12 month disorder were considered serious (29.6%) or moderate (42.6%). Analyses of comorbidity found multiple disorders were also common. Having multiple disorders is clearly associated with increased severity (see Table 6) and knowledge of both the prevalence of disorders and patterns of comorbidity are important. These findings provide evidence that high prevalence rates among Māori are not primarily mild disorders; among many Māori who have disorder, the disorders are likely to have a considerable impact.
As a cross-sectional survey, it is not possible to determine the factors causing mental disorders among Māori. However, the NZMHS investigated some associations with mental disorder. Findings for demographic correlates are consistent with findings for the total population, with higher rates of disorder in Māori women compared with Māori men (33.6% vs 24.8%). This is contributed to by an increased rate of anxiety and mood disorders in women [31]. Prevalence was highest among younger age groups, with 12 month disorder occurring in one-third (33.2%) of Māori aged 15–24 years and one-third (32.9%) of Māori aged 25–44 years. Mental health is thus also an important health issue among Māori aged 25–44 years as well as among Māori youth.
The relationship between equivalized household income and mental disorder is evidence that socioeconomic position likely plays a role in contributing to mental disorders among Māori. In contrast, the 12 month prevalence of disorder across urbanicity (rural, semirural, provincial and urban) and region shows a non-significant variation between differing areas and suggests a fairly similar prevalence across localities.
Overall, results for the prevalence among Māori are consistent with concerns raised over recent decades and reinforce commentary that defines mental health as a significant public health issue for Māori. Common mental disorders (anxiety, mood and substance disorders) are prevalent among Māori and findings for severity and comorbidity indicate that the high Māori prevalence is not made up of primarily mild disorder.
These findings have implications for mental health promotion and prevention, the primary and secondary care sectors, Māori health providers and mental health policy-makers. Knowing the pattern and prevalence of disorder provides a platform to describe Māori mental health problems and need and informs strategies to address disparities. Further research focusing on causes of mental disorder and on effective interventions to meet Māori needs is required.
Footnotes
Acknowledgements
Te Rau Hinengaro: The New Zealand Mental Health Survey was funded by the Ministry of Health, Alcohol Advisory Council and Health Research Council of New Zealand. The survey was carried out in conjunction with the World Health Organization World Mental Health Survey Initiative. We thank the WMH staff for assistance with instrumentation, fieldwork and data analysis. These activities were supported by the US National Institute of Mental Health (R01MH070884), the John D and Catherine T MacArthur Foundation, the Pfizer Foundation, the US Public Health Service (R13-MH066849, R01-MH069864, and R01 DA016558), the Fogarty International Center (FIRCA R01-TW006481), the Pan American Health Organization, Eli Lilly and Company, Ortho-McNeil Pharmaceutical, Inc, GlaxoSmithKline, and Bristol-Myers Squibb. The WMH publications are listed at ![]() .
.
Other members of the NZMHS research team are MA Oakley Browne, JE Wells, KM Scott, J Kokaua, S Foliaki, D Schaaf, C Tukuitonga and C Gale.
We thank Will Edwards, the Kaitiaki Group and Pacific Advisory Group for their input and support for this survey and we thank all the participants.