
Abstract
Suicide and attempted suicide are serious sources of mortality and morbidity in New Zealand [1]. Approximately 500 people die by suicide annually and there are almost 4500 hospital admissions for suicide attempt each year [2]. Suicide (after road traffic accidents) is the second most common reason for death among people aged 15–34 years [3].
Suicidal behaviours are strong risk factors for suicide and for further suicide attempts [4]. While males more often die by suicide, females make more suicide attempts [2]. Suicidal behaviours are thus a problem for both sexes. In terms of ethnic distribution, 16.9% of suicides in 2003 involved Māori (who constitute 14.1% of the population) (http://www.stats.govt.nz, accessed 14 April 2006), 4.3% involved Pacific people (6.4% of the population) and 5.4% involved Asian people (6.2% of the population). The majority (73.4%) were European (73.3% of the population) [5].
Previous New Zealand studies have examined suicidal behaviour in the Canterbury region, in a Dunedin-born cohort and in a Christchurch-born cohort, and in a national study of teenagers attending high schools [6–11]. Prevalence estimates varied by age, sex, study and population and ranged, for lifetime rates of suicidal ideation, from 13% to 29.2%, and for lifetime rates of suicide attempt from 1% to 10.6%. In general, higher lifetime rates of ideation and attempt were reported for younger people and for females.
These, and other, New Zealand studies have also examined the contribution of a series of risk factors to suicidal behaviour [4, 12]. Risk factors ranging from individual level factors (e.g. genes, personality, sexual orientation) to macrosocial factors (e.g. unemployment rates), and spanning exposure to trauma, family factors, mental disorders, life stresses, social supports, socioeconomic factors, cultural factors, and macrosocial and macroeconomic factors, have all been shown to contribute to suicidal behaviours [4, 12]. In addition, rates of suicide and attempted suicide are known to vary with age, sex and ethnicity [4]. This survey is the first nationally representative survey to examine the prevalence of, and sociodemographic and mental disorder correlates for, suicidal behaviours in New Zealand, and to have adequate numbers of Māori and Pacific participants to generate estimates of such behaviours with acceptable precision.
Method
Sample
Te Rau Hinengaro: The New Zealand Mental Health Survey was a nationally representative household survey of people aged 16 years and over. Face-to-face interviews were conducted by professional interviewers between October 2003 and December 2004. The survey was approved by all 14 regional health ethics committees. Written informed consent was obtained from all participants. Māori and Pacific people were oversampled. A detailed report of methods is given elsewhere [13]. The response rate was 73.3%. The interview consisted of two parts. Part 1 included core diagnostic sections (including the suicide questions) and demographics and was administered to everyone (n = 12 992). Part 2 consisted of additional diagnostic sections and other measures of mental and physical health and was administered to a subsample (n = 7435), called the long-form subsample. Participants who met certain criteria in the Part 1 diagnostic sections received the long form of the interview. A probability subsample of other participants also received the long form [13, figure 13.1].
Diagnostic assessment
The interview included diagnostic sections from version 15 of the World Mental Health Composite International Diagnostic Interview [14] (CIDI 3.0) which generates diagnoses according to ICD-10 [15] and DSM-IV [16]. Only DSM-IV diagnoses are reported here. Disorders were diagnosed with hierarchy rules except for substance abuse, which is reported whether or not there was dependence. Participants without any symptom ever of substance abuse (alcohol or drugs) skipped the associated dependence section, so dependence is dependence with abuse at some time.
The CIDI 3.0 asks if symptoms have ever occurred and then asks about recency. Twelve-month disorder is diagnosed if full criteria for disorder have ever been met and there have been symptoms or an episode in the past 12 months. Full criteria may not have been met in the past 12 months.
Sociodemographic correlates
Sociodemographic correlates included age at interview, sex, prioritized ethnicity, educational qualifications and equivalized household income. Multiple ethnicities were permitted. The standard New Zealand prioritization rule is to classify anyone who self-identifies as Māori (either solely or in addition to other ethnicities) as Māori, and anyone who mentions any Pacific ethnic group, but not Māori, as Pacific. Educational qualifications were assessed using questions about school and post-school qualifications from the 2001 Census of Population and Dwellings. Household income was missing for 13.0% of respondents and was imputed by linear regression. A modification of the revised Jensen equivalence scale for household income [17] was used to take account of the number of adults and number of children in the household.
Definitions of suicidal behaviour
For the purposes of this paper, suicidal behaviour included the following behaviours, defined by the questions asked in the survey (http://www.hcp.med.harvard.edu/wmhcidi/) [18]:
Suicidal ideation: thinking seriously about committing suicide
Suicide plan: making a plan for committing suicide
Suicide attempt: making a suicide attempt
Analyses
Data were weighted to account for different probabilities of selection that arose from oversampling Māori and Pacific people and the selection of one person per household, differential non-response, and residual differences in age, sex and ethnicity between the sample and the 2001 census population. Additional weights were used to account for selection into the long-form sections of the interview. Analyses were carried out using SUDAAN 9.0.1 with two strata (High Pacific and General) and census meshblocks as the primary sampling units. The sample design was preserved for analysis of subgroups by use of the subpopulation command in SUDAAN [19]. Confidence intervals were calculated with appropriate methods [19–21].
Results
Lifetime and 12 month prevalences
Table 1 shows estimated 12 month and lifetime prevalences of suicidal ideation, plans and attempts for males, females and the total population. The more severe suicidal behaviours occurred less often. While lifetime suicidal ideation was relatively common (15.7%), plans (5.5%) and attempts (4.5%) were less common. Similarly, while 3.2% reported suicidal ideation in the past 12 months, only 1.0% reported making plans and 0.4% reported making an attempt.
Twelve-month and lifetime prevalence of suicidal ideation, suicide plan and suicide attempt, by sex
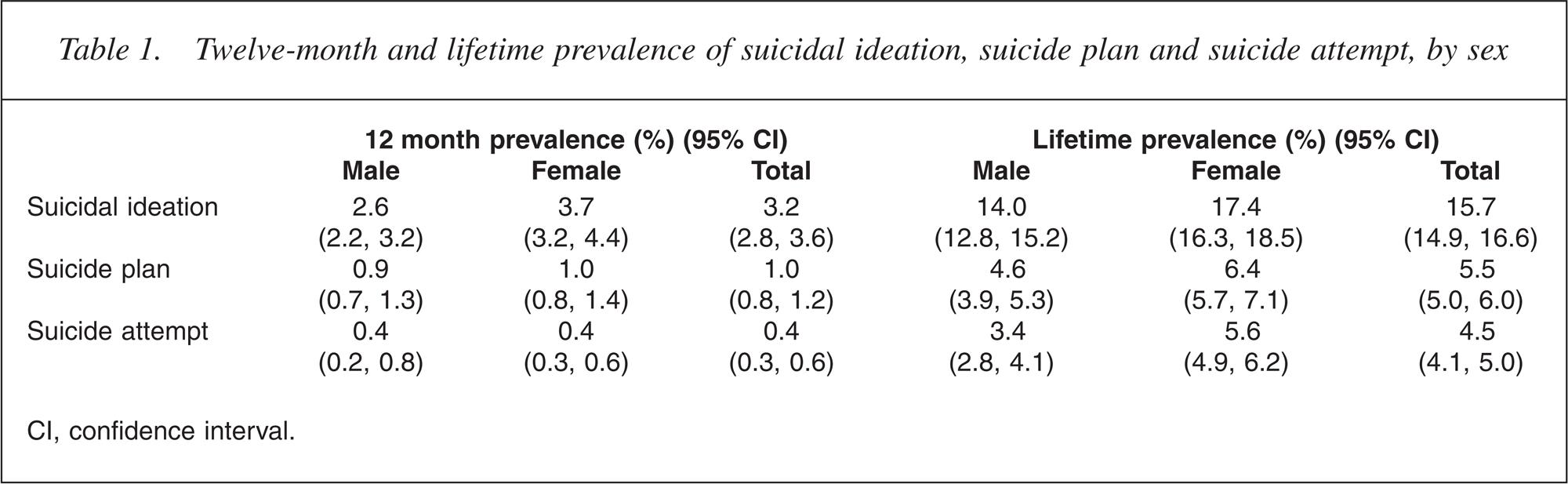
CI, confidence interval.
Females consistently reported higher lifetime rates of suicidal ideation (p < 0.0001), plan (p < 0.005) and attempt (p < 0.0001) than males. However, in the past 12 months, males and females were equally likely to have made plans and attempts, despite females significantly more often reporting suicidal ideation (p < 0.05).
Suicide attempts range in severity from the mildly injurious to the determinedly lethal. All those who made attempts were asked about the lethality and intent of their first and their most recent attempt. Almost half (46.5%) of those who made one or more attempts reported that their first attempt was a serious attempt to die and it was only by chance that they did not succeed; 37.0% reported that they did not intend to die in their first attempt and it was a ‘cry for help’; 16.5% reported that their first attempt was serious, but they were not certain that the method would kill them.
Levels of intent and lethality reported for the first attempt were strikingly similar to those reported for the most recent attempt (among those who reported more than one lifetime suicide attempt): 47.9% reported that their most recent attempt was a serious attempt to die; 15.1% reported that the attempt was serious, but they were not certain it would kill them; and 36.9% reported that they did not intend to die.
Onset distributions
Hazard functions were estimated to show the first onset of suicidal ideation, plan and attempt (Fig. 1) [22]. This analysis yielded the following results.
Median ages of onset for all three behaviours were in the 20s: 25 years for suicidal ideation and making a plan, and 21 years for an attempt.
Although the onset of suicidal ideation was most likely to occur in late adolescence, onset continued throughout adult life: 2.8% (2.4, 3.2) reported suicidal ideation by age 15 years, 10% (9.3, 10.8) by age 25 years, 17.5% (16.5, 18.5) by age 50 years and 20.2% (19.1, 21.3) by age 75 years.
A similar pattern emerged for suicide plans: 0.9% (0.7, 1.1) reported plans by age 15 years, 3.6% (3.1, 4.0) by age 25 years, 6.2% (5.6, 6.9) by age 50 years and 7.2% (6.5, 7.9) by age 75 years.
For suicide attempts, 0.8% (0.6, 1.0) reported attempts by age 15 years, 3.2% (2.9, 3.7) by age 25 years, 5.1% (4.6, 5.6) by age 50 years and 5.5% (5.0, 6.2) by age 75 years.
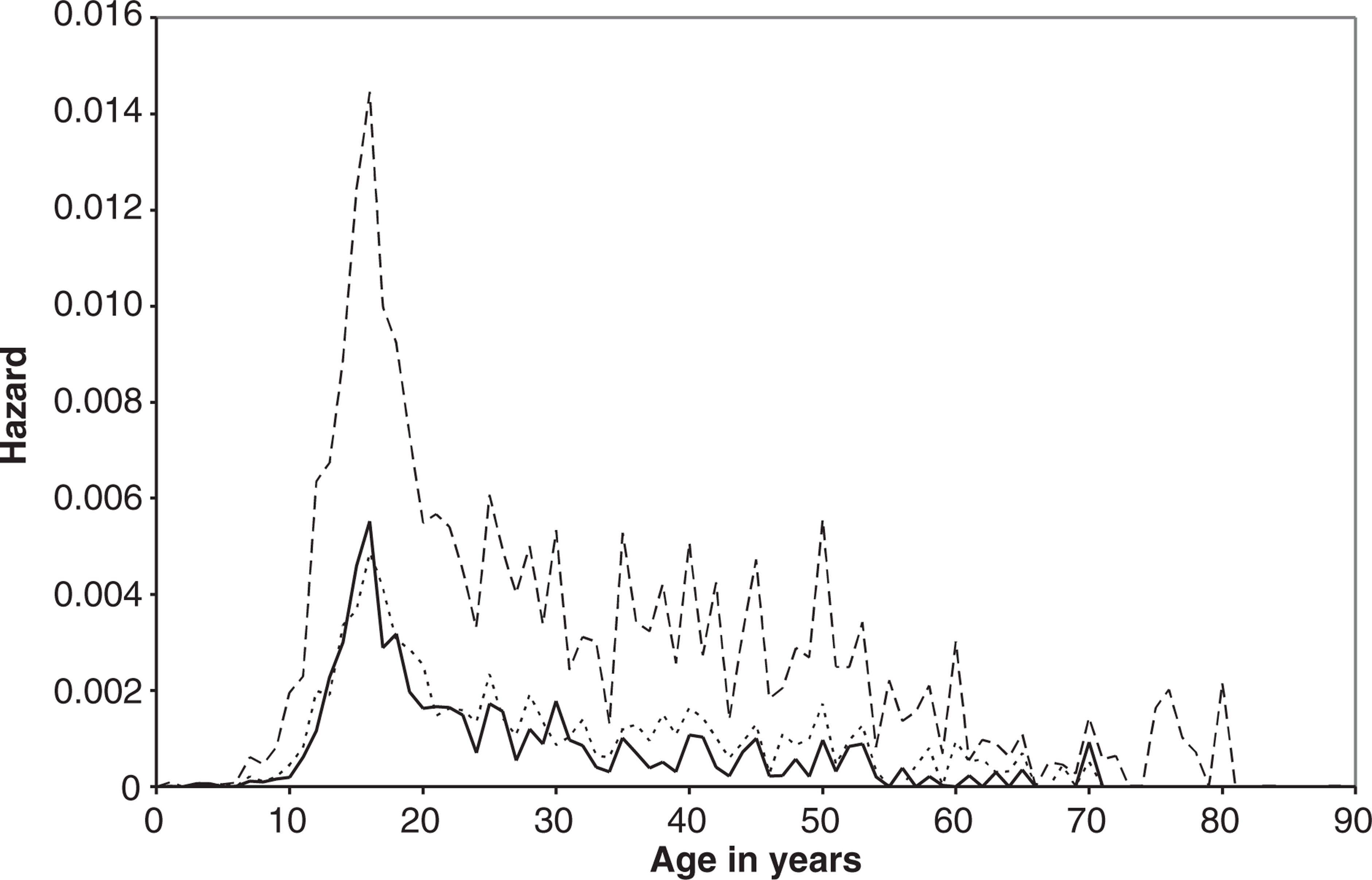
Hazard functions of first onset of suicidal ideation, suicide plan and suicide attempt. (— — —) Ideation; (– – –) Plan; (———) Attempt.
Sociodemographic correlates
Table 2 shows 12 month prevalences for suicidal ideation, plan and attempt classified by age, sex, educational qualifications and household income separately. (Correlates are not presented for lifetime suicide attempts because of the potential disjunction between currently measured sociodemographic variables and historically reported attempts.) Reports of odds ratios (OR) below are from a joint model of all four covariates.
Sociodemographic characteristics and prevalence of suicidal ideation, suicide plan and suicide attempt in the past 12 months
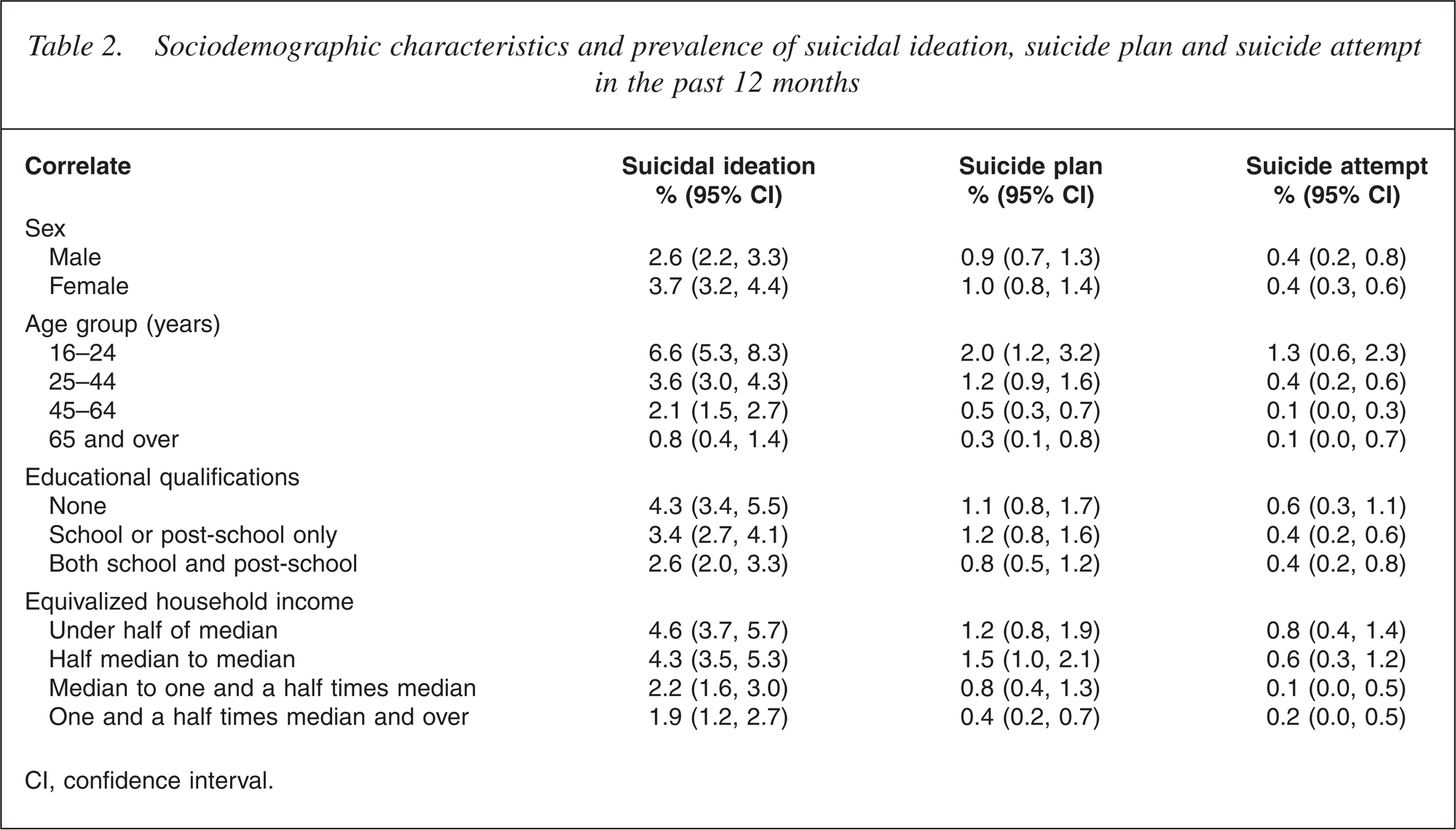
CI, confidence interval.
Population risk of ideation was significantly higher in females (OR = 1.4 [1.0, 1.8], p < 0.05) and in younger people (OR = 10.7 [5.8, 19.7], p < 0.0001), with risk decreasing with increasing age. Ideation was higher in people with fewer educational qualifications (OR = 1.6 [1.1, 2.3], p < 0.05) and in those with low household income (OR = 2.1 [1.3, 3.2], p < 0.0001).
The risk of making a plan for suicide was higher in younger people (OR = 6.1 [1.9, 101.5], p < 0.0001) with risk decreasing with increasing age, and in people with low household income (OR = 2.3 [1.1, 5.0], p < 0.005). Sex and educational qualifications made no contribution to the risk of making a suicide plan.
The risk of attempt was higher in younger people (OR = 10.9 [1.2, 101.5], p < 0.005) and in people from low-income households (OR = 3.7 [1.0, 13.2], p < 0.01). Sex and educational qualifications did not contribute to the 12 month risk of suicide attempt.
Ethnicity and prevalence of suicidal behaviours
Table 3 shows the rates of suicidal ideation, plan and attempt classified by ethnic group (Māori, Pacific and Other). The table shows:
unadjusted 12 month prevalences; 12 month prevalences adjusted for age and sex (to take account of the younger Māori and Pacific populations, compared with the Other population); 12 month prevalences adjusted for age, sex, educational qualifications and household income.
Ethnicity and 12 month prevalence of suicidal behaviours
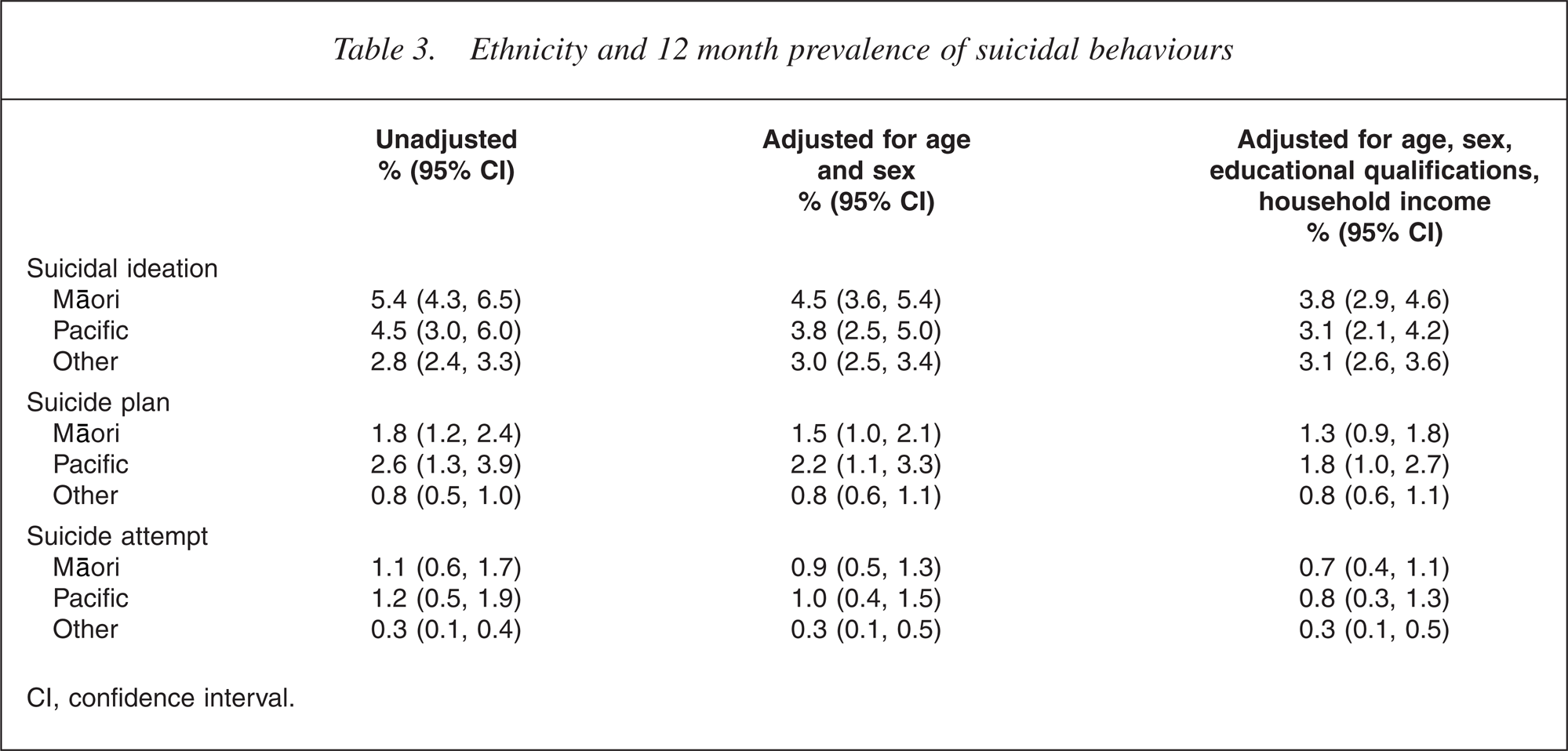
CI, confidence interval.
Māori and Pacific participants reported significantly higher rates than Other participants of ideation (p < 0.0001), plan (p < 0.0001) and attempt (p < 0.0002). In addition, Māori had significantly higher rates of suicidal ideation than Pacific participants, whereas Pacific participants had significantly higher rates of plans and attempts than Māori participants. However, adjusted estimates suggest that some of these ethnic differences may be sociodemographic in origin. After adjustment for sociodemographic factors, there were no ethnic variations in suicidal ideation. However, Māori and Pacific participants had significantly higher rates of making plans (p < 0.006) and attempts (p < 0.01) after adjustment for sociodemographic factors.
Mental disorder correlates
Percentages of suicidal behaviour by mental disorder in the past 12 months were estimated for a series of DSM-IV mental disorders (Table 4). Compared with the overall 12 month prevalences of suicidal ideation (3.2%), plan (1.0%) and attempt (0.4%), individuals with any mental disorder had elevated risks of ideation (11.8%), plan (4.1%) and attempt (1.6%).
Mental disorder in the past 12 months and risk of suicidal ideation, suicide plan and suicide attempt in the past 12 months
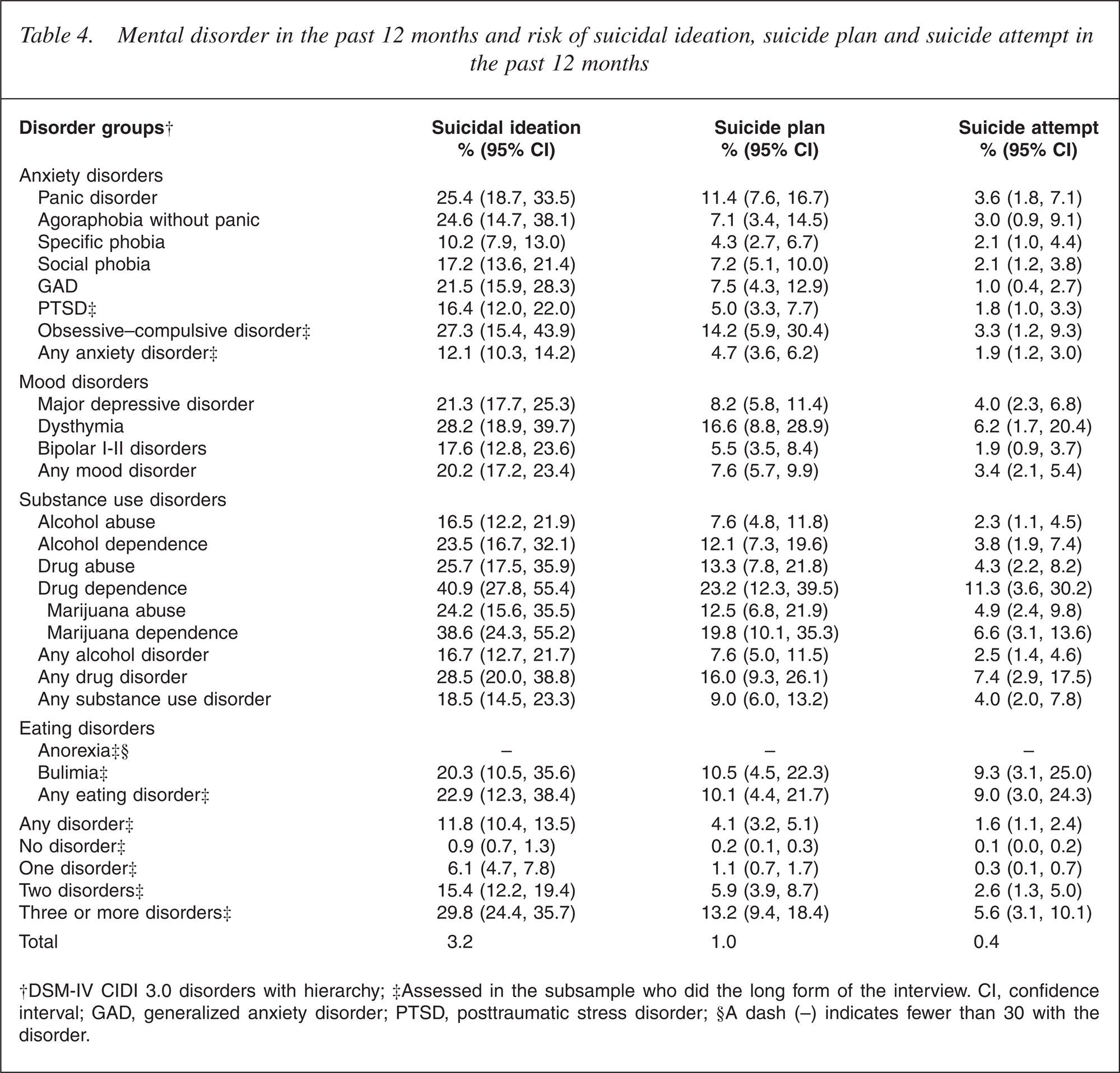
†DSM-IV CIDI 3.0 disorders with hierarchy; ‡Assessed in the subsample who did the long form of the interview. CI, confidence interval; GAD, generalized anxiety disorder; PTSD, posttraumatic stress disorder; §A dash (–) indicates fewer than 30 with the disorder.
The following classes of disorders were associated with suicidal ideation: mood disorder (OR = 7.0 [5.0, 9.7], p < 0.0001), anxiety disorder (OR = 4.0 [2.8, 5.5], p < 0.0001) and substance use disorder (OR = 3.8 [2.6, 5.7], p < 0.0001).
These disorders were also associated with risk of making a plan for suicide: mood disorder (OR = 7.3 [4.6, 11.7], p < 0.0001), anxiety disorder (OR = 6.0 [3.6, 10.2], p < 0.0001) and substance use disorder (OR = 5.4 [3.1, 9.2], p < 0.0001).
The risk of suicide attempt was associated with mood disorder (OR = 8.6 [4.3, 17.0], p < 0.0001), substance use disorder (OR = 4.8 [1.9, 12.1], p < 0.0008) and anxiety disorder (OR = 3.8 [1.9, 7.6], p < 0.0002).
Of all individual mental disorders, major depressive disorder was most strongly associated with ideation (OR = 7.2 [4.9, 10.8], p < 0.0001), plan (OR = 7.2 [3.7, 14.0], p < 0.0001) and attempt (OR = 14.3 [6.2, 32.7], p < 0.0001).
The risk of suicidal ideation, plan and attempt increased with increasing number of disorders. Among individuals with three or more disorders, 29.8% reported suicidal ideation (compared with 6.1% of those with only one disorder), 13.2% reported making a plan (compared with 1.1% of those with one disorder) and 5.6% reported an attempt (compared with 0.3% of those with one disorder) [23].
Health services use
The extent to which those who reported 12 month suicidal ideation, plans and attempts made visits to health service providers for mental health problems in the past 12 months was explored. While available data do not give precise information about the timing of these visits in relation to suicidal behaviour, or whether the visit was specifically for suicidal behaviour, it is useful to know the fraction of those with suicidal behaviour within the past 12 months who also made visits for mental health problems.
Almost half of those with a 12 month history of suicidal ideation (42.8%), plan (45.0%) or attempt (44.7%) did not make any general medical or specialist mental health visits within the same 12 month period in which they were suicidal. More specifically, of those with suicidal ideation, 16.7% reported that they had made visits to a psychiatrist within the past 12 months, 34.5% had made visits to a psychiatrist and/or another mental health professional, and 53.6% had made any visit for a mental health problem. Of those who made a plan for suicide, 25.8% had made visits to a psychiatrist within the past 12 months, 41.7% had made visits to a psychiatrist and/or another mental health professional and 54.5% had made visits to any health professional. Of those who made an attempt, 31.5% had made visits to a psychiatrist within the past 12 months, 45.2% had made visits to a psychiatrist and/ or another mental health professional and 53.7% had made visits to any health professional.
Discussion
The findings of this survey have implications for the following major themes relating to the prevalence, correlates and the management of suicidal behaviours in New Zealand:
Prevalence of suicidal behaviours
Suicidal ideation was common, with 15.7% of participants acknowledging a lifetime history of suicidal ideation while rates of suicide plans (5.5%) and attempts (4.5%) were lower. Reports of suicidal behaviours were more common among the young and decreased with increasing age. Lifetime rates of suicidal behaviours were consistently significantly higher in females than in males.
The findings in this survey are broadly consistent with estimates of suicidal ideation and attempt obtained in previous New Zealand studies [6–10] (with the exception of the National Secondary School Youth Health Survey [11], which reported rates of suicidal behaviour in the year before interview that were higher than the findings from other New Zealand studies) and with findings from national surveys conducted in comparable Organization for Economic Co-operation and Development countries. These studies have reported lifetime prevalence of suicidal ideation ranging from 11.3% to 16.5% and of attempt ranging from 3.1% to 4.9% [7, 24, 25], and 12 month prevalence of ideation ranging from 3.3% to 3.4% and of attempt ranging from 0.4% to 0.6% [24, 26], close to the New Zealand prevalences of 3.2% and 0.4%, respectively. The findings in this survey are consistent with previous studies in suggesting that suicidal behaviours are a problem for both sexes: while males are more likely to die by suicide, morbidity is dominated by females [2].
It should be noted that the observed prevalences for suicidal behaviours are likely to be underestimates, because of participant reluctance to admit to stigmatized suicidal behaviours or because of non-participation in the survey. It is also likely that the observations of decreasing suicidal behaviours with increasing age may reflect, in part, recall bias or forgetting: with age, historical events become overlaid with more recent life experiences. However, these limitations are likely to apply to a similar degree to comparable surveys.
Sociodemographic correlates of suicidal behaviours
Suicidal ideation in the past 12 months was associated with sociodemographic factors including female sex, youth, few educational qualifications and low household income, while 12 month plans and attempts were linked with youth and low household income. These findings are consistent with a large body of New Zealand and international evidence that has shown consistent links between a range of social and demographic factors and suicidal behaviours [4, 12, 27, 28].
Ethnicity and suicidal behaviour
Māori and Pacific participants reported significantly higher rates of suicidal ideation, plan and attempt than Other participants. Some of these ethnic differences in suicidal behaviours were explained by social and demographic factors. These findings are consistent with a large body of international and New Zealand evidence that has found elevated rates of suicidal behaviour among aboriginal and ethnic minority populations, with these higher rates accounted for, in part, by higher rates of social deprivation and disadvantage and, in part, by acculturative stress [4,29–34].
Mental disorders and suicidal behaviours
Individuals with mental disorder had elevated rates of suicidal behaviour, with 11.8% of those with any disorder reporting suicidal ideation, 4.1% making a plan and 1.6% making an attempt. Mood disorders, anxiety disorders, eating disorders, and alcohol, drug and substance use disorders were all associated with increased rates of suicidal ideation, plan and attempt, with major depressive disorder having the strongest association with each type of suicidal behaviour. These findings confirm the association between mental disorders, and, particularly, mood disorders, and the risk of suicidal behaviours found in extensive New Zealand and international research. In particular, in this study, as in previous research mental disorders are consistently the strongest risk factor for suicidal behaviour [4, 12, 27, 28] and are more strongly associated with suicidal behaviour than socioeconomic factors. This evidence implies that a major approach to preventing and reducing suicidal behaviours lies in better identifying, treating and managing the mental disorders, particularly mood disorders and substance use disorders, associated with suicidal behaviours [4, 27, 28, 35].
Visits made to health professionals for suicidal behaviours
Individuals with suicidal behaviours need to have such behaviours, and the mental disorders with which they may be associated, treated and managed optimally, to reduce risk of further suicidal behaviour and because mental disorders require treatment in their own right [36]. However, in this survey, almost half of those who reported suicidal behaviours within the 12 months before interview made no visits to specialist mental health professionals or other health professionals in that period. In particular, less than one-third (31.5%) of those who attempted suicide received treatment from a psychiatrist. These findings are generally consistent with New Zealand and international research that suggests most people with suicidal behaviours and the mental disorders with which they are associated tend to be poorly treated or not to receive treatment at all [37–39]. The reasons for this are likely to include both patient failure to access treatment (e.g. because of stigmatization, lack of services, difficulty accessing services, a belief that the problem will resolve without treatment, a lack of awareness of the availability or efficacy of treatment) and physician failure to recognize, refer and adequately treat mental illness and suicidal behaviour.
Given the increased risk of suicidal behaviour in those with mental illness, these findings suggest that major approache s to reduce suicidal behaviour are likely to include:
public education programs aimed at improving the recognition of suicide risk and mental disorders, and translating increased knowledge and attitudinal changes about these conditions to behavioural changes, including improved help-seeking, and increased compliance with medication and treatment regimes [40, 41]; programs focusing on educating physicians and primary health-care workers about recognizing, treating and managing depression, substance use disorders and suicidal behaviours [42, 43]; integrated care networks that provide long-term mental health care and support for people with mental disorders to prevent suicide [35].
Footnotes
Acknowledgements
The New Zealand Mental Health Survey was funded by the Ministry of Health, Alcohol Liquor Advisory Council and Health Research Council of New Zealand, and conducted in conjunction with the World Health Organization World Mental Health (WMH) Survey Initiative. We thank the WMH staff for assistance with instrumentation, fieldwork and data analysis. These activities were supported by the US National Institute of Mental Health (R01MH070884), the John D and Catherine T. MacArthur Foundation, the Pfizer Foundation, the US Public Health Service (R13-MH066849, R01-MH069864 and R01 DA016558), the Fogarty International Center (FIRCA R01-TW006481), the Pan American Health Organization, Eli Lilly and Company, Ortho-McNeil Pharmaceutical, Inc., GlaxoSmithKline, and Bristol-Myers Squibb. The WMH publications are listed at ![]() .
.
Other members of the research team are K Scott, J Baxter, TK Kingi, R Tapsell, S Foliaki, D Schaaf, MH Durie, C Tukuitonga and C Gale.
We thank the Kaitiaki Group and Pacific Advisory Group for their input and support for this survey and we thank all the participants.