
Abstract
The disability burden associated with the common mental disorders has been demonstrated cross-sectionally in primary care studies [1, 2], general population surveys [3–6] and longitudinal designs [7–10]. The Global Burden of Disease study [11] has also made a compelling case for the disability burden of mental disorders. That study found unipolar depression to be the leading cause of disability worldwide, with neuropsychiatric disorders collectively making up five of the 10 leading causes of disability.
A case has been made for the importance of using generic (rather than disorder-specific) measures of functioning that can evaluate the relative impact of different mental disorders and allow comparison across mental and physical disorders [4]. The information obtained from such measures is an important empirical underpinning for health-care policy concerned with resource allocation. Among generic measures, the SF-36 has often been used, although its usage entails problems of symptom-outcome overlap [3], difficulties with the interpretation of the principal component summary scores among those with physical and mental disorder comorbidity [12], and questionable validity of the summary scores among ethnic groups endorsing a non-Western model of health [13]. Other generic measures have been used such as days out of role and activities of daily living, but these lack the comprehensiveness of the multidimensional instruments.
The World Mental Health (WMH) Survey Initiative version of the World Health Organization Disability Assessment Schedule (WMH WHO-DAS) was developed from a preliminary version of WHO-DAS II for use in the WMH surveys. The WHO-DAS II is based on a conceptual model of disability that attempts to synthesize the opposing medical and social models of disability: the International Classification of Functioning, Disability and Health (ICF) [14]. The WHO-DAS II and the WMH variant measure disability in several domains: role impairment, mobility, self-care, social functioning, cognitive functioning and participation in society. Te Rau Hinengaro: The New Zealand Mental Health Survey is among the first of the WMH surveys to publish data from WMH WHO-DAS domains other than role impairment. This paper also comprises the first New Zealand data to be published on the disability associated with common mental disorders. The aims of the paper are to:
compare role impairment across mental disorder groups, controlling for comorbidity, and across types of comorbid disorder; provide a disability profile (including five WMH WHO-DAS domains) for different types of mental disorder and for selected physical disorders, with and without comorbidity.
Method
Sample
Te Rau Hinengaro: The New Zealand Mental Health Survey was a nationally representative household survey involving face-to-face interviews with 12 992 people aged 16 years and over. Interviews were conducted from October 2003 to December 2004 and the survey achieved a response rate of 73.3%. M5ori and Pacific ethnic groups were oversampled. The survey methods are explained in another paper in this issue [15].
Measures
Mental disorders
The interview used to assess mental disorder was version 15 of the WMH Composite International Diagnostic Interview (CIDI). Version 20 is now the CIDI 3.0 [16]. This ascertains lifetime disorder plus recency of episodes or symptoms, which allows 12 month and 1 month DSM-IV diagnoses to be derived. One-month diagnoses are reported here, by disorder group, with organic exclusions. Diagnoses were calculated with hierarchy (with the exception of substance abuse, which is reported whether or not there was dependence). The disorder groups included in this paper are:
Anxiety disorders: panic disorder, agoraphobia without panic, specific phobia, social phobia, generalized anxiety disorder, posttraumatic stress disorder, obsessive-compulsive disorder Mood disorders: major depressive disorder, dysthymia, bipolar disorder (I, II, and any with mania or hypomania) Substance use disorders: alcohol abuse, alcohol dependence, drug abuse, drug dependence
Everyone received Part 1 of the interview, but a long-form subsample (n = 7435) received additional sections (Part 2) [15], figure 1].
Chronic physical conditions
Participants in the long-form subsample were asked if they had ever had arthritis, rheumatism, chronic back or neck problems, frequent or severe headaches, other chronic pain, seasonal allergies, stroke, heart attack, or whether they had ever been told by a doctor they had heart disease, high blood pressure, asthma, tuberculosis, chronic lung disease, diabetes, ulcer, HIV/AIDS, epilepsy, cancer [17, table 1]. For problems that could have remitted (pain, seasonal allergies, high blood pressure, tuberculosis, diabetes or ulcer), participants were also asked if they still had the condition(s) in the past 12 months. The 12 month prevalence of chronic conditions reported here includes the enduring conditions and those others still present in the past 12 months. Similar conditions, or conditions that have similar risk factors, are grouped together and only the more prevalent conditions are reported.
Disability
The WMH WHO-DAS was administered as a generic section to all participants in the long-form sample asking about disability in the past 30 days. In this study, the WMH WHO-DAS was scored to produce subscale scores for five domains:
Role impairment (Role): four items measuring the number of days the participant was completely unable to work or carry out their normal activities, or had to cut back on the amount or quality of activity, or had to apply extreme effort to perform at their usual level because of physical health, mental health, or substance use problems Understanding and communicating (Cognitive): four items recording difficulties with concentration, understanding, memory or learning Getting around (Mobility): three items measuring difficulties with standing for at least 30 minutes, moving around inside the house and walking distances of about one kilometre Self-care (Self-care): three items recording difficulties with washing the body, getting dressed, staying by oneself for a few days Getting along with others (Social): five items measuring difficulties in starting and maintaining conversation, dealing with unknown people, forming and maintaining friendships, controlling emotions around people
All domains were scored on a 0–100 scale with higher scores representing greater disability. Two scores were calculated for the Role domain. The ‘all health’ score was calculated from the four role impairment items: [(1.0 × days out of role + 0.5 × days cut down + 0.25 × days cut back on quality + 0.25 × days it took extreme effort)/30] × 100. The ‘attributed to mental health’ score was calculated from the three items asking the respondent how much of the reported impairment was due to mental health problems: [(1.0 × days out of role + 0.5 × days cut down + 0.5 × days it took extreme effort)/ 30] × 100. The remaining four domains were scored using a formula that weighted the number of days the individual reported disability out of the past 30 days by the severity of disability reported in a given domain.
Analysis
Estimates were weighted to take into account the probability of selection, to adjust for oversampling, to adjust for non-response and to post-stratify by age, sex and ethnicity to the 2001 census population. Mean WMH WHO-DAS role impairment scores are given for both the number of mental disorders and presence of disorders grouped by their comorbidity. Multiple regression was used to produce least squares estimates of the mean WMH WHO-DAS domain scores for mental disorders and for chronic physical conditions, adjusted for the differential age and sex distributions between those with and without the specified disorder. Analyses were carried out using SUDAAN 9.0.1. Taylor series linearization was used to approximate the variance of estimates [18].
Results
Role impairment among people with mental disorders
The role impairment scores in Tables 1 and 2 integrate days out of role with days of partially impaired performance. For example, an individual reporting three full days out of role, plus 9 days of cutting down out of the past 30 days, would score 25: [(1.0 × 3 + 0.5 × 9) × (100/30)] × 100.
Role impairment in the past month† in total, and attributed to mental health problems, by number of 1 month mental disorders‡§
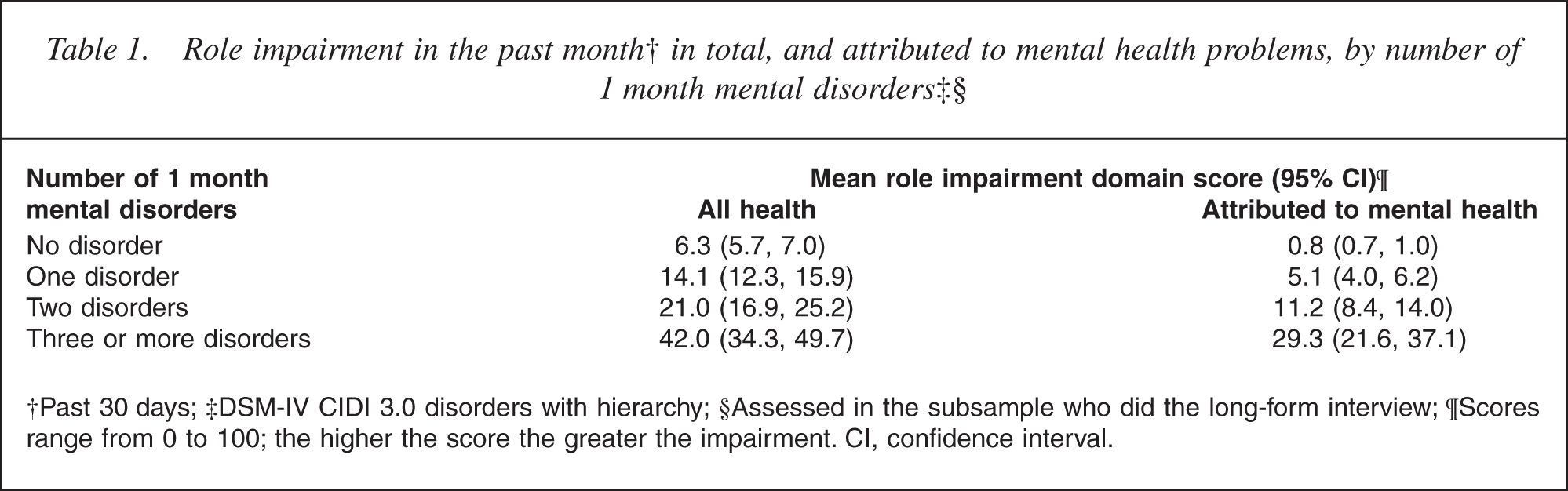
†Past 30 days; ‡DSM-IV CIDI 3.0 disorders with hierarchy; §Assessed in the subsample who did the long-form interview; ¶Scores range from 0 to 100; the higher the score the greater the impairment. CI, confidence interval.
Role impairment in the past month† by 1 month single and comorbid disorders‡§
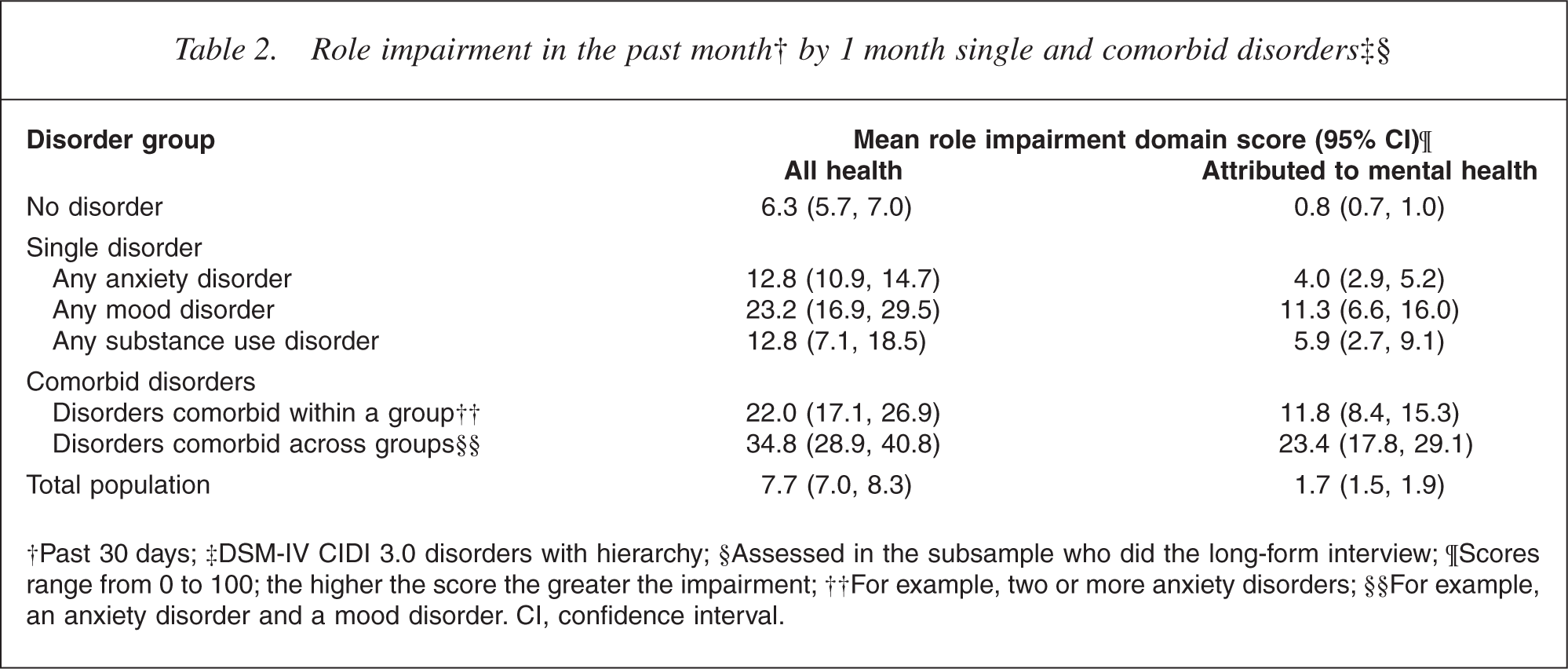
‡DSM-IV CIDI 3.0 disorders with hierarchy; §Assessed in the subsample who did the long-form interview; ¶Scores range from 0 to 100; the higher the score the greater the impairment; ††For example, two or more anxiety disorders; §§For example, an anxiety disorder and a mood disorder. CI, confidence interval.
The mean score of 42 reported by those with three or more disorders therefore represents substantial disability. Table 1 shows a monotonic pattern of increasing role impairment with increasing number of mental disorders. As the number of mental disorders increases, the proportion of role impairment attributed to mental health problems also increases. Among people with only one disorder, mood disorders were associated with substantially more role impairment than anxiety or substance use disorders (Table 2). Consideration of the subgroup with single disorders avoids the potential confound of some mental disorders being more likely to be comorbid than others. People with mood disorders also attributed a greater proportion of their total role impairment to mental health problems relative to those with anxiety disorders, although the proportion was similar to that for substance use disorders.
Table 2 also provides an assessment of the role impairment associated with different types of mental disorder comorbidity. While this suggests that across-group comorbidity is more impairing than withingroup comorbidity, this is largely a function of the fact that those with multiple mood disorders were few in number relative to those with multiple anxiety disorders; in contrast, the majority of those with across-group comorbidity had a mood disorder (data not shown).
Disability profile for mental and physical disorders
Table 3 shows the other four domain scores in addition to the role impairment (‘all health’) score. The role impairment scores are generally higher than the other domain scores, due in part to the generic nature of the role impairment domain relative to the other more specific domains of functioning, but also to the scoring of the role impairment domain. High scores on any of the WMH WHO-DAS domains are rare, but this is particularly so with the four domains other than role impairment. For example, someone reporting mild impairment on one of these domains on five out of 30 days would score about 2; moderate impairment on five out of 30 days would score about 6; moderate impairment on 15 out of 30 days would score about 25.
WMH WHO-DAS domain scores associated with 1 month mental disorders† and chronic physical conditions‡
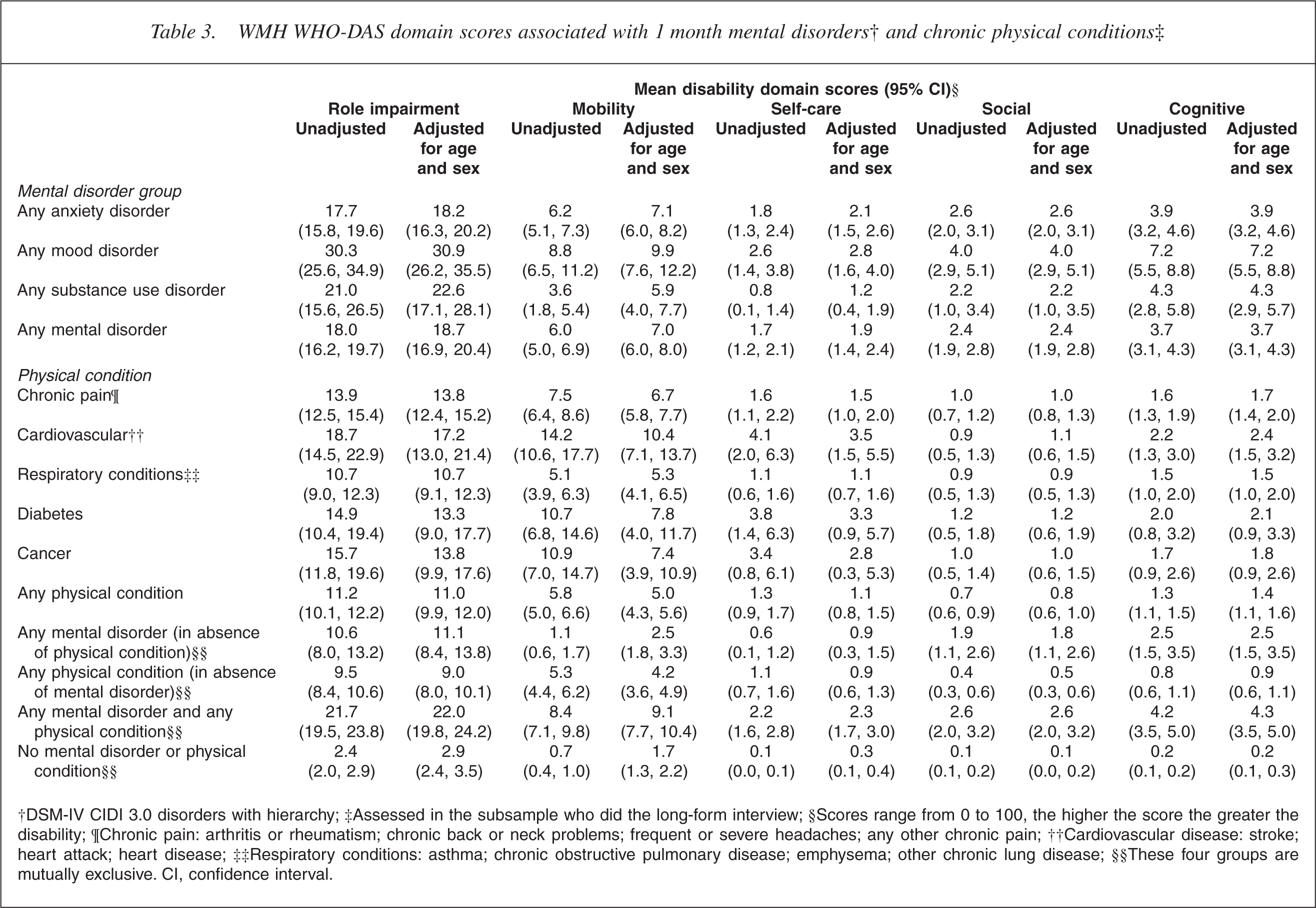
†DSM-IV CIDI 3.0 disorders with hierarchy; ‡Assessed in the subsample who did the long-form interview; §Scores range from 0 to 100, the higher the score the greater the disability; ¶¶Chronic pain: arthritis or rheumatism; chronic back or neck problems; frequent or severe headaches; any other chronic pain; ††Cardiovascular disease: stroke; heart attack; heart disease; ‡‡Respiratory conditions: asthma; chronic obstructive pulmonary disease; emphysema; other chronic lung disease; §§These four groups are mutually exclusive. CI, confidence interval.
Mood disorders were again associated with more disability, across domains, than anxiety or substance use disorders (here, comorbidity is not excluded). Looking at the four domains other than role impairment, self-care problems were least associated with mental disorders, and mobility appears the most affected. However, the scores for ‘any mental disorder in the absence of physical condition’ suggest that the mobility impairment associated with mental disorders in the upper part of the table may be partly a function of comorbid physical disorders.
Among the physical disorders, cardiovascular disease was generally associated with the greatest impairment, with diabetes the next most disabling of those shown. Looking across the four specific domains, physical disorders were associated with most impairment in the mobility domain, followed by self-care.
In comparing people with ‘any mental disorder’ with people with ‘any physical condition’, without excluding comorbid conditions, mental disorders appear to be associated with more disability. However, after excluding comorbid conditions, mental and physical disorders appear similarly disabling on average, although physical disorders were associated with more disability in the mobility domain and mental disorders were associated with more disability in the social and cognitive domains, as might be expected.
The scores associated with the category of ‘any mental disorder plus any physical condition’ indicate that mental-physical comorbidity more than doubles the disability associated with mental disorders or physical conditions alone.
Discussion
The key findings are: mood disorders were associated with substantially more role impairment than anxiety or substance use disorders; experiencing multiple mental disorders at the same time was associated with major impairment of role functioning; mental disorders and chronic physical conditions were associated with similar degrees of disability, on average; the combination of mental and physical disorders was more disabling than either alone.
The finding that mood disorders were associated with greater disability across WMH WHO-DAS domains than other disorder groups is not a function of bipolar disorders as the impairment reported by those with bipolar disorders was similar to that reported by those with major depressive disorder (data available on request); nor is it a function of comorbid mental disorders, as the relative level of disability associated with depression was similar whether or not comorbidity was controlled for. The association of depression and disability has a long history in the literature, but whether mood disorders are more disabling than anxiety disorders is not clear-cut. Some have found this to be the case [3, 4, 9, 19] while others have not [2, 5, 6]. Sanderson and Andrews found that even mild depression was associated with more disability than any anxiety disorder, although that study used the SF-12 mental health summary score as the disability measure, which may have inflated disability scores because of its overlap with some symptoms of depression [4]. The European Study of the Epidemiology of Mental Disorders [6] used a role impairment measure similar to that used here and found that mood and anxiety disorders groups were associated with identical levels of impairment. However, that study analysed role impairment among 12 month disorders, which may underestimate the disability associated with disorders such as major depression, which are more episodic than anxiety disorders. (The much greater difference between 1 month and 12 month prevalence estimates for any mood disorder relative to any anxiety disorder is shown in [15, table 2].)
In sum, we believe this study offers evidence that mood disorders are associated with more disability than other mental disorder groups, although it remains a possibility that some individual anxiety disorders may be as disabling as mood disorders. This finding may be viewed with some scepticism since research has found that individuals high in ‘negative affectivity’, a trait-like tendency to experience negative mood states, give exaggerated reports of health complaints relative to objective indicators of health status [20]. This has led negative affectivity to be viewed as a confounding factor in research relying on self-reported outcomes [21, 22], and has raised doubts about the validity of self-reported disability in depressed individuals [23, 24]. Other researchers, observing that the degree of self-reported social disability by depressed individuals abates once depressive symptoms have been relieved, indicating no sustained social impairment, have also concluded that depressed individuals ‘over-report’ their degree of disability [25].
These concerns about whether self-reported disability in depression is (i) accurately reported and (ii) real impairment, may be eased by viewing the issue through the framework of the ICF. In the ICF model, impairments represent temporary or permanent problems in function (or structure), including psychological functions. In this view, a mood disorder represents a disruption in aspects of psychological functioning (the impairment), resulting in activity and participation limitations (the disability). As others have suggested, the psychological functions affected are likely to be several, at least involving systems of motivation, cognition and emotional regulation [26]. This pervasiveness of psychological dysfunction has implications for all domains of functioning measured by instruments such as the WMH WHO-DAS. The impairments associated with some physical conditions, by contrast, may be less pervasive and the resulting activity limitations more circumscribed. In this model, it is not that the depressed individual's symptoms lead them to make a pessimistic assessment of their capabilities while the reality is otherwise; rather, it is the pessimistic perspective that disables them, along with the anhedonia and other psychological dysfunction (see also [9]).
The set of results comparing mental and physical disorders contains few surprises, given previous studies on the topic. But given the differences in study population, methodology, diagnoses and disability measure across studies, that is perhaps the most surprising thing in itself. The current results replicate some specific findings observed previously, such as that cardiovascular disease is the most disabling of the common chronic medical conditions [1]. They also replicate more general findings that, once comorbidity is excluded, mental disorders are at least as disabling as chronic physical conditions, and the two in combination are at least twice as disabling as either alone [1, 9, 26, 27].
This study has several strengths. It is a populationbased survey with a substantial sample size, good response rate and the capacity to generate DSM-IV disorder diagnoses. One-month diagnoses were used, generating more accurate assessments of associated disability. However, the sampling frame did not include people in institutions, making it likely that some people with severe disorders are underrepresented. It is also the case that the assessment of chronic physical conditions in this survey was self-reported, and although other research has demonstrated a reasonable correspondence between selfreported physical disease and medical records [28], the negative affectivity research noted above may suggest a potential problem with this methodology. However, although negative affectivity has been correlated with self-reported physical symptoms, it is not correlated with self-reported diagnosed chronic diseases [29]. Participants reported most physical conditions included here on the basis of diagnoses they had received. The chronic pain category is an exception, and is probably the most susceptible to the influence of emotional disorders on reports of prevalence.
The WMH WHO-DAS disability measure has strengths and weaknesses. Its strengths, in terms of its comprehensiveness, conceptual framework and assessment of functioning rather than symptomatology, have been noted above. A clear weakness is that its psychometric qualities have been inadequately assessed. However, the current results for specific domains are as one would expect intuitively and the general thrust of the findings is similar to that obtained previously, so they offer some initial validation of the measure.
Footnotes
Acknowledgements
Te Rau Hinengaro: The New Zealand Mental Health Survey (NZMHS) was funded by the Ministry of Health, the Alcohol Advisory Council of New Zealand and the Health Research Council of New Zealand. The survey was carried out in conjunction with the World Health Organization World Mental Health (WMH) Survey Initiative. We thank the WMH staff for assistance with instrumentation, fieldwork and data analysis. These activities were supported by the US National Institute of Mental Health (R01-MH070884), the John D and Catherine T MacArthur Foundation, the Pfizer Foundation, the US Public Health Service (R13-MH066849, R01-MH069864, and R01-DA016558), the Fogarty International Center (FIRCA R01-TW006481), the Pan American Health Organization, Eli Lilly and Company, Ortho-McNeil Pharmaceutical, Inc, GlaxoSmithKline, and Bristol-Myers Squibb. The WMH publications are listed at ![]() .
.
Other members of the NZMHS Research Team are J Baxter, J Kokaua, TK Kingi, R Tapsell, S Foliaki, D Schaaf, MH Durie, C Tukuitonga and C Gale.
We thank the Kaitiaki Group and Pacific Advisory Group for their input and support for this survey and we thank all the participants.