
Abstract
There is little debate that mental disorder comorbidity, that is, the occurrence of two or more disorders at the same time or within a given period (e.g. 12 months or lifetime), is a common phenomenon. The Epidemiologic Catchment Area Study [1] and the National Comorbidity Survey (NCS) [2] in the US found lifetime comorbidity rates of 54% and 56% respectively. The Australian National Mental Health Survey observed a 12 month comorbidity rate of around 39% [3]. Research from the European component of the World Mental Health (WMH) Survey Initiative has also documented substantial 12 month comorbidity [4].
While the existence of mental disorder comorbidity is in no doubt, there is nonetheless debate as to its signifi-cance. It is a moot point whether the development and ongoing refinement of psychiatric classification systems based on explicit diagnostic criteria have confirmed or created the comorbidity findings [5, 6]. Certainly the considerable increase in number of diagnostic categories from DSM-III to DSM-IV has increased the prevalence estimates of comorbid disorders [7]. However, it does not necessarily follow that the phenomenon of comorbidity lacks relevance. It is useful to consider 12 month and lifetime comorbidity separately, as they are important for different reasons.
Lifetime comorbidity can offer important opportunities for the secondary prevention of mental disorder. NCS data showed that later onset disorders are typically occurring to those who have already had at least one disorder [8]. They also showed that the experience of early onset disorders confers greater risk for the occurrence of a second later-onset disorder, and that these secondary later-onset disorders are frequently more persistent and severe than primary later-onset disorders [6].
Twelve-month comorbidity, this paper's focus, is important in the increased burden it places on individuals and on treatment services. Twelve-month comorbid disorders have been associated with more severe symptoms [9], a greater likelihood of suicide attempts [10] and greater disability [3, 11]. Comorbidity also increases the likelihood of treatment seeking [3,12] and frequently complicates treatment, leading to poor treatment response [13, 14].
This paper presents the first information on 12 month comorbidity for the New Zealand population. Such country-specific data may have implications for the configuration of mental health services. Although mental health service delivery in New Zealand varies regionally, recent years have seen a move towards specialized service delivery with separate services established for some disorder groups (e.g. anxiety disorders or substance use disorders). Findings on the prevalence and treatment implications of comorbid disorders need to be available to policy-makers concerned with mental health service planning.
This paper aims to:
describe the distribution and patterning of 12 month mental disorder comorbidity in the New Zealand population; and investigate the relationship between 12 month comorbid mental disorders and severity, suicidality and health sector use.
The disability associated with 1 month comorbid disorders is presented in another paper in this issue [15].
Method
Sample
Te Rau Hinengaro: The New Zealand Mental Health Survey (NZMHS) was a nationally representative household survey involving face-to-face interviews with 12 992 people aged 16 years and over. Interviews were conducted in late 2003 and throughout 2004 and the survey achieved a response rate of 73.3%. Both M5ori and Pacific ethnic groups were oversampled. The survey methods are described in more detail elsewhere [16, 17].
Measures
The interview used to assess mental disorder was version 15 of the WMH Survey Initiative Composite International Diagnostic Interview (CIDI) [18]. Version 20 is now the CIDI 3.0. This interview ascertains lifetime disorder plus recency of episodes or symptoms, which allows 12 month and 1 month DSM-IV diagnoses to be derived. Diagnoses are reported with organic exclusions. Diagnoses were calculated with hierarchy with the exception of substance use disorders. Abuse is reported whether or not there was dependence, but for disorder counts the presence of dependence and abuse was counted as one disorder for alcohol and for drugs. Although comorbidity research more typically calculates diagnoses without hierarchy, we have applied hierarchical rules because this better approximates a clinical approach to disorder count. Since one emphasis in this paper is on the relationship between comorbidity and treatment services, this approach is appropriate. The following hierarchy rules were applied:
Major depressive disorder: no mania or hypomania permitted.
Dysthymia: no major depression permitted in the first 2 years and no mania or hypomania permitted.
Generalized anxiety disorder (GAD): not diagnosed if it occurred exclusively within a mood disorder; if both posttraumatic stress disorder (PTSD) and GAD occurred within the 12 months and the PTSD duration was longer, GAD was not diagnosed.
Analysis
Estimates were weighted to take into account the probability of selection, to adjust for oversampling, to adjust for non-response, and to post-stratify by age, sex and ethnicity to the 2001 census population. Odds ratios were calculated to assess the degree of association between individual disorders in a series of logistic regression models containing one disorder as the independent variable and the other disorder as the dependent variable. Analyses were carried out in SUDAAN 9.0.1. Taylor series linearization [19] was used to approximate the variance of estimates. For prevalences with less than 30 events in the numerator, confidence intervals were calculated according to a method by Korn and Graubard [20].
Results
Distribution of mental disorder comorbidity
Table 1 shows the proportion of the population with one disorder (13%), two disorders (4.4%) and three or more disorders (3.3%), which indicates the spread of psychopathology in the population. The ‘Cases’ column shows that a little over a third (21.1% plus 15.9%) of those with any disorder had more than one disorder. The ‘Diagnoses’ column considers the total number of 12 month disorders occurring to participants, and shows the proportion of these occurring to people with one disorder, two disorders, and three or more disorders. Only 38.6% of 12 month disorders occurred to people with just one disorder, whereas the remaining 61.4% of disorders occurred to people with two or more disorders (who comprise 7.7% of the population). This tells us something about the concentration of psychopathology, in that the majority of disorders occur to those who already have a disorder (i.e. they are comorbid disorders [2]).
Distribution of 12 month comorbidity among the population, cases and diagnoses†
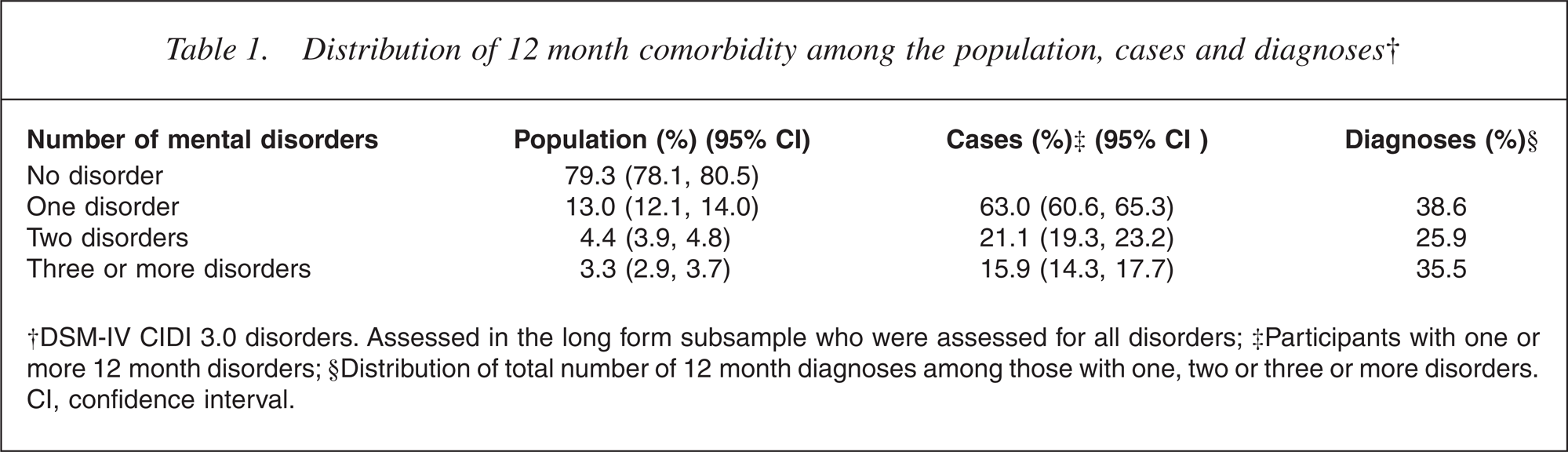
†DSM-IV CIDI 3.0 disorders. Assessed in the long form subsample who were assessed for all disorders; ‡Participants with one or more 12 month disorders; §Distribution of total number of 12 month diagnoses among those with one, two or three or more disorders. CI, confidence interval.
Patterns of mental disorder comorbidity
Table 2 shows the overlap between mental disorder groups. Approximately half (49.6%) of those experiencing a 12 month mood disorder also experienced an anxiety disorder, but the proportion of those with anxiety disorders who had a comorbid mood disorder was considerably smaller (26.6%). The proportions of those with either anxiety or mood disorders who had a comorbid substance use disorder were smaller still. These figures reflect the relative prevalences of the disorder groups (i.e. large for anxiety and small for substance use), and the large number of anxiety disorders within the group; they are not a guide to the strength of association between disorder groups. The table gives a further illustration of the general phenomenon of mental disorder comorbidity: among those with any mood disorder 49.6% experienced an anxiety disorder compared with 14.8% of the general population.
Percentage with a comorbid 12 month mental disorder, by 12 month mental disorder group†
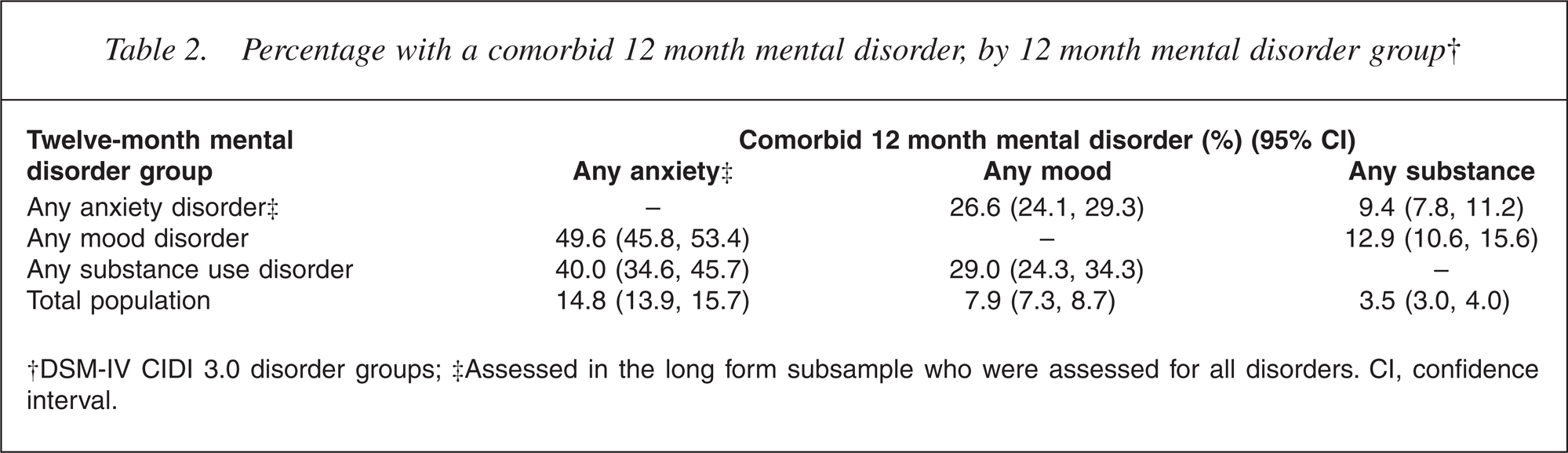
†DSM-IV CIDI 3.0 disorder groups; ‡Assessed in the long form subsample who were assessed for all disorders. CI, confidence interval.
Table 3 shows the association between two individual disorders. Within-group associations are highly variable for anxiety disorders, ranging from a non-significant association between GAD and PTSD (largely precluded by hierarchy rules) to the expected strong association between social phobia and agoraphobia. Within-group associations are not presented for mood disorders as these are largely precluded by hierarchy rules, and the interview presented additional complications for the interpretation of associations between dysthymia and major depression. Associations between alcohol and drug use disorders are the strongest in the table by a considerable margin, although these estimates are relatively imprecise.
Bivariate associations (odds ratios) of DSM-IV 12 month mental disorders,† with hierarchy
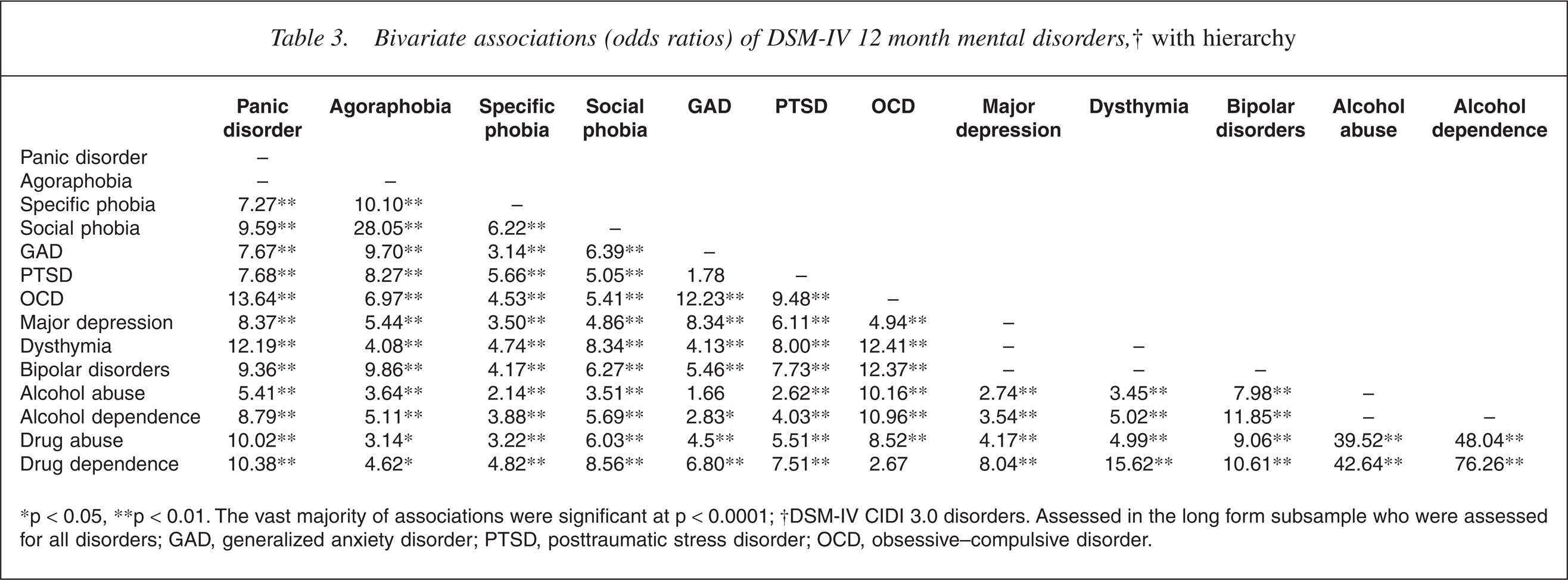
∗p < 0.05, ∗∗p < 0.01. The vast majority of associations were significant at p < 0.0001; †DSM-IV CIDI 3.0 disorders. Assessed in the long form subsample who were assessed for all disorders; GAD, generalized anxiety disorder; PTSD, posttraumatic stress disorder; OCD, obsessive–compulsive disorder.
Notable across-group associations (in terms of strength of association) include those between bipolar disorders and substance use disorders; panic disorder and drug use disorders; obsessive–compulsive disorder (OCD) and alcohol use disorders; OCD and mood disorders (particularly bipolar disorders and dysthymia).
Relationships between mental disorder comorbidity and severity and suicidal behaviour
The comparison of the 11.7% classified as serious cases among those with one disorder with the 59.6% classified as serious among those with three or more disorders, indicates a clear association between increasing number of disorders and case severity (Table 4).
Percentage in each category of severity, by number of 12 month mental disorders†
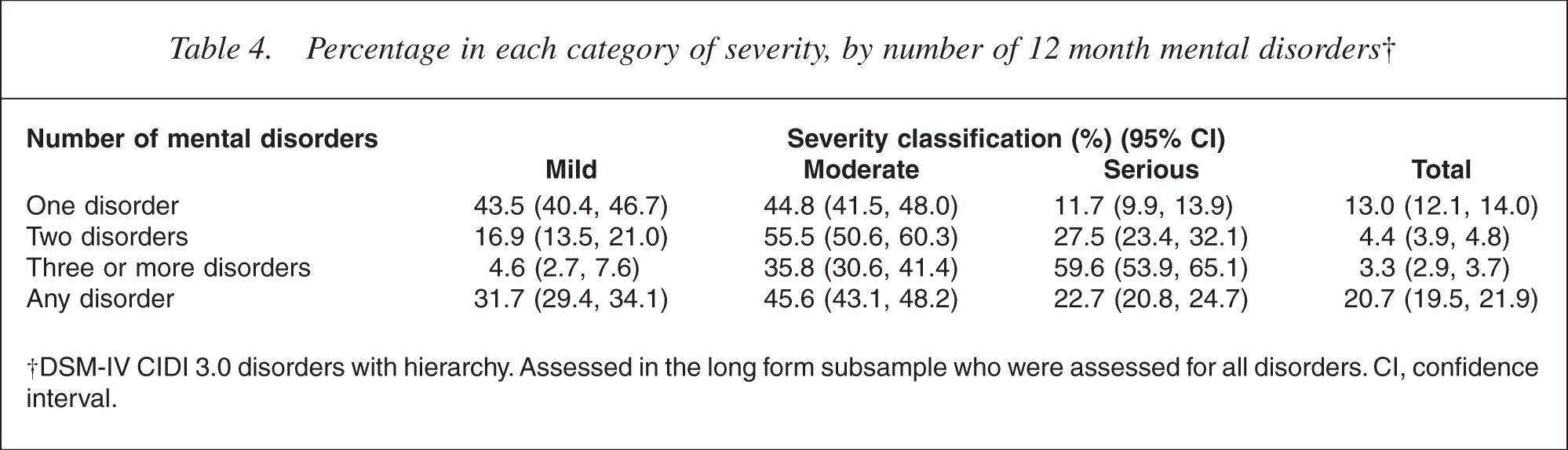
†DSM-IV CIDI 3.0 disorders with hierarchy. Assessed in the long form subsample who were assessed for all disorders. CI, confidence interval.
A clear relationship also exists between an increasing number of disorders and suicidal ideation, plans and attempts (Table 5). This is particularly noticeable with suicide attempts, where the proportion with three or more disorders attempting suicide (5.6%) exceeds the proportion of suicide attempters among those with one disorder (0.3%) 18-fold.
Suicidality, by number of 12 month mental disorders†
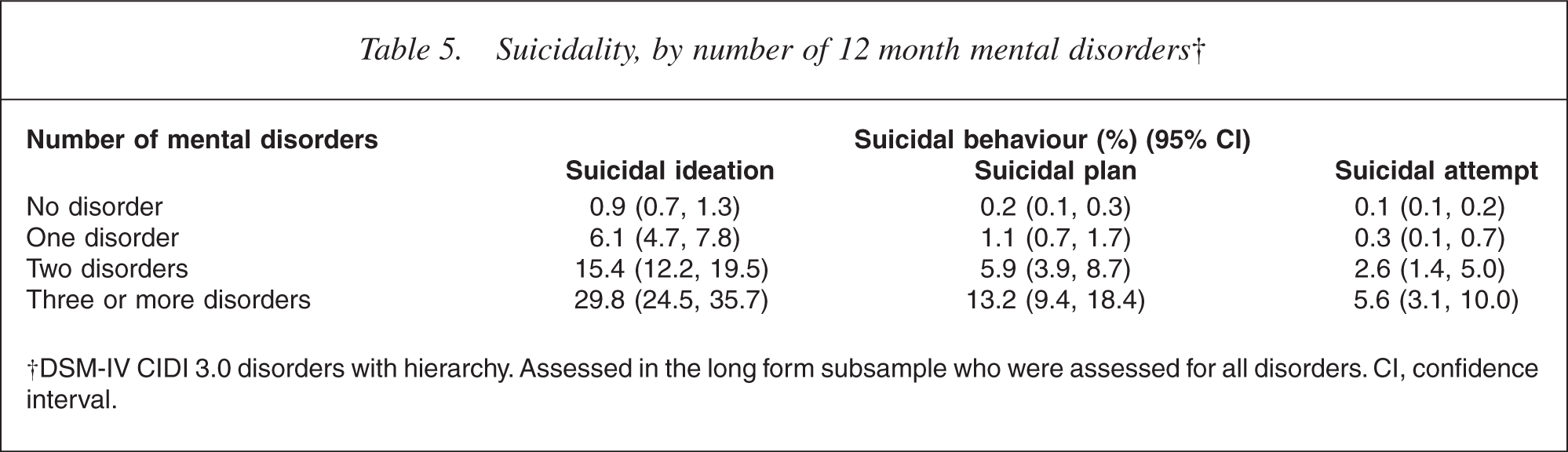
†DSM-IV CIDI 3.0 disorders with hierarchy. Assessed in the long form subsample who were assessed for all disorders. CI, confidence interval.
Relationship between mental disorder comorbidity and health sector service use
People with more disorders are more likely to access health services of all kinds (Table 6). However, the greatest impact of mental disorder comorbidity is on the use of mental health services, psychiatric services in particular. Some 16.8% of people with three or more disorders visited a psychiatrist in the past 12 months, which is more than five times the percentage (3.1%) of people with one disorder who visited a psychiatrist. By contrast, the proportion of people with three or more disorders who accessed general medical care for a mental health visit (45.1%) was a little over twice the proportion of people with one disorder (21.8%) who accessed general medical care for a mental health visit.
Percentage using health services for a mental health visit in past 12 months, by number of 12 month disorders†
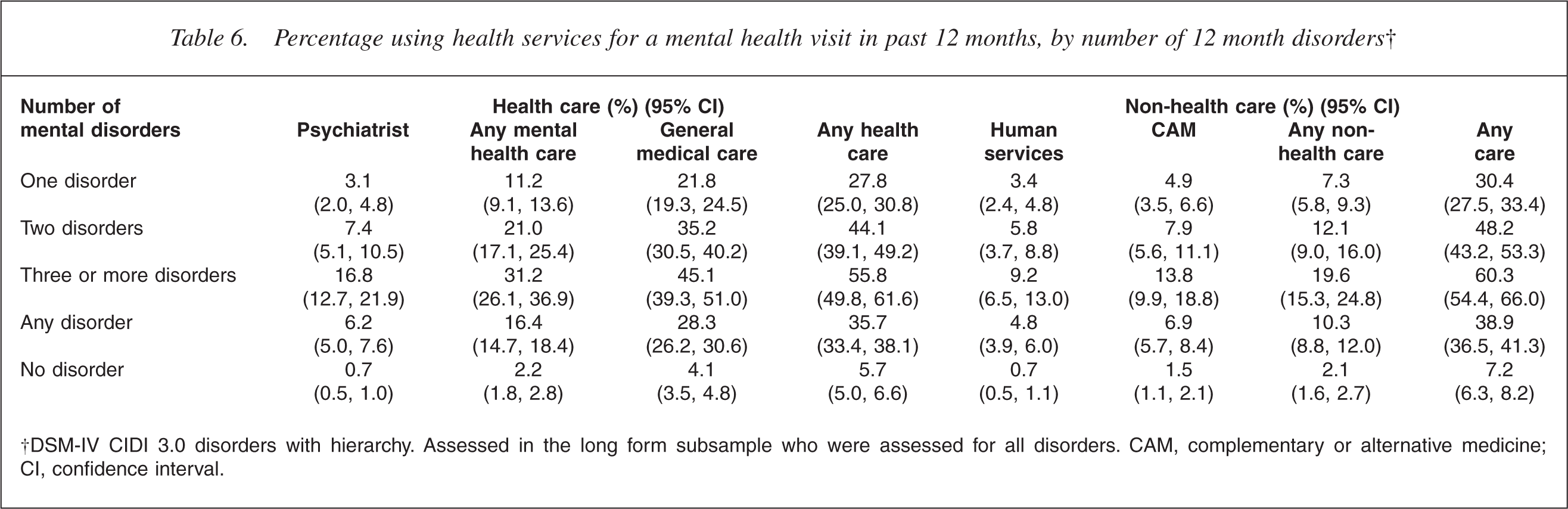
†DSM-IV CIDI 3.0 disorders with hierarchy. Assessed in the long form subsample who were assessed for all disorders. CAM, complementary or alternative medicine; CI, confidence interval.
Discussion
The NZMHS found that 12 month mental disorder comorbidity is common in New Zealand, occurring among 37% of 12 month cases. The most common comorbidity is between mood and anxiety disorders. The strongest associations are between alcohol and drug use disorders, which showed a very high likelihood of cooccurrence within the 12 month timeframe. Substance use disorders also showed substantial associations with some anxiety disorders (especially panic disorder and OCD) and with some mood disorders (especially bipolar disorders). OCD showed close associations with some other anxiety disorders and with bipolar disorders. Comorbidity was strongly related to case severity, suicidal behaviour (especially suicide attempt) and health sector use (especially mental health sector use).
With the exception of the bivariate associations, these results correspond to those of prior research. The Australian National Mental Health Survey found 39% of people with 12 month disorders had more than one disorder (also applying hierarchy rules); the figure for New Zealand is 37%. The frequent comorbidity between anxiety and mood disorders is well established in other countries where the relative prevalence of anxiety and mood disorders is similar [6]. The association of comorbidity with suicidal intent observed in the current study gives cross-sectional support for Vollrath and Angst's finding [10] of an increased prevalence of completed suicides among those with comorbid panic and depression. The association of comorbidity and service utilization found here replicates the findings of studies cited earlier.
The bivariate associations in this study are often very different from those reported in other research, but this is largely due to our application of hierarchy rules, which makes comparisons difficult. It is interesting that in the hierarchy-free analyses of other surveys stronger associations have typically been found between anxiety and mood disorders than between substance use disorders and either anxiety or mood disorders [5, 21]. This was not the case in the NZMHS, where associations between substance use disorders and specific anxiety and mood disorders were some of the stronger ones obtained. Such relationships may be important from a clinical perspective.
Differences in bivariate associations across studies will also reflect differences in the interview. It is notable that other research has often found that OCD does not show elevated odds ratios with other anxiety disorders [21]. By contrast, both the NZMHS and the US component of the WMH surveys, the NCS Replication, found strong associations between OCD and other anxiety disorders (panic disorder, GAD, PTSD) [22]. Comorbidity patterning is therefore sensitive to changes in the CIDI, reducing consistencies in disorder associations across studies.
In general terms, mental disorder comorbidity is clearly a robust phenomenon, which is associated with serious consequences for the individual and treatment services. These data show that the majority of mental health service users have comorbid disorders. At the same time, the service provision framework in New Zealand allows for the operation of separate services for specific disorder groups. Definite advantages are associated with a disorder-specific approach to service provision, but it is not clear how well such an approach deals with the clinical reality of mental disorder comorbidity.
Footnotes
Acknowledgements
The New Zealand Mental Health Survey was funded by the Ministry of Health, the Alcohol Advisory Council of New Zealand and the Health Research Council of New Zealand. The survey was carried out in conjunction with the World Health Organization WMH Survey Initiative. We thank the WMH staff for assistance with instrumentation, fieldwork and data analysis. These activities were supported by the US National Institute of Mental Health (R01-MH070884), the John D and Catherine T Mac-Arthur Foundation, the Pfizer Foundation, the US Public Health Service (R13-MH066849, R01-MH069864, and R01-DA016558), the Fogarty International Center (FIRCA R01-TW006481), the Pan American Health Organization, Eli Lilly and Company, Ortho-McNeil Pharmaceutical, Inc., GlaxoSmithKline, and Bristol-Myers Squibb. WMH publications are listed at ![]() .
.
Other members of the NZMHS Research Team are J Baxter, J Kokaua, TK Kingi, R Tapsell, S Foliaki, D Schaaf, MH Durie, C Tukuitonga and C Gale.
We thank the Kaitiaki Group and Pacific Advisory Group for their input and support for this survey and we thank all the participants.