
Abstract
Research has documented significant comorbidity between mental disorders and chronic physical conditions. Several studies have documented the poorer physical health status of people with mental disorders relative to those without mental disorders [1–3]. As might be expected, this has a flow-on effect into premature mortality risk, which is higher for the population with mental disorders, after removing deaths owing to suicide [4]. A considerable body of research has also documented higher rates of mental disorder, in particular depression and anxiety, in people with medical disease compared with those without medical disease [5–8]. Comorbid mental disorders among the medically ill lead to greater role impairment [9, 10], higher treatment costs and lower treatment adherence [11]. Mental disorders also make an independent contribution to the mortality risk of the medically ill population, in particular depression among those with cardiovascular disease [12] and diabetes [13].
The occurrence of mental-physical comorbidity therefore has considerable individual and public health significance. The separation of mental health treatment services from treatment for physical disorders that is typical of Western industrialized countries makes it useful for each service setting to have information on the prevalence of mental-physical comorbidity in the population it primarily serves. This paper therefore aims to provide, for the New Zealand population, estimates of the prevalence of:
chronic physical conditions among those with 12 month mental disorder; key risk factors for chronic physical conditions among those with 12 month mental disorder; and 12 month mental disorder among those with chronic physical conditions.
Method
Sample
Te Rau Hinengaro: The New Zealand Mental Health Survey (NZMHS) was a nationally representative household survey involving face-to face interviews with 12 992 people aged 16 years and over. Interviews were conducted from October 2003 to December 2004 and the survey achieved a response rate of 73.3%. M5ori and Pacific ethnic groups were oversampled. A more detailed description of the survey methods is provided elsewhere [14, 15].
Measures
Mental disorders
The interview used to assess mental disorder was version 15 of the World Mental Health Composite International Diagnostic Interview (WMH-CIDI). Version 20 is now the CIDI 3.0 [16]. This ascertains lifetime disorder plus recency of episodes or symptoms, which allows 12 month and 1 month DSM-IV diagnoses to be derived. Twelvemonth diagnoses are reported here, with organic exclusions. Diagnoses were calculated with hierarchy (with the exception of substance abuse, which is reported whether or not there was dependence). The disorder groups included in this paper are:
Anxiety disorders: panic disorder, agoraphobia without panic, specific phobia, social phobia, generalized anxiety disorder, posttraumatic stress disorder, obsessive-compulsive disorder. Mood disorders: major depressive disorder, dysthymia, bipolar disorder (I, II and any with mania or hypomania). Substance use disorders: alcohol abuse, alcohol dependence, drug abuse, drug dependence.
The number of participants with eating disorders in the past 12 months was too small for the analyses in this paper. Everyone received Part 1 but a long-form subsample (n = 7435) received additional sections (Part 2) [14, figure 1].
Chronic physical conditions
Chronic physical conditions were screened for by asking participants in the long-form subsample if they had ever had arthritis, rheumatism, chronic back or neck problems, frequent or severe headaches, other chronic pain, seasonal allergies, stroke, heart attack, or whether they had ever been told by a doctor they had had heart disease, high blood pressure, asthma, tuberculosis, chronic lung disease, diabetes, ulcer, HIV/AIDS, epilepsy or cancer (Table 1). Prior research has demonstrated reasonable correspondence between self-reported chronic conditions such as diabetes, heart disease and asthma, and general practitioner medical records [17]. For problems that could have remitted participants were asked if they still had the condition/s in the past 12 months (Table 1). The 12 month prevalence of chronic conditions reported here includes the enduring conditions and those others still present in the past 12 months. Similar conditions, or conditions that have similar risk factors, are grouped together and only the more prevalent conditions are reported (see footnotes to Tables 2–4 for the grouping of conditions).
Survey questions on chronic physical conditions in the New Zealand Mental Health Survey
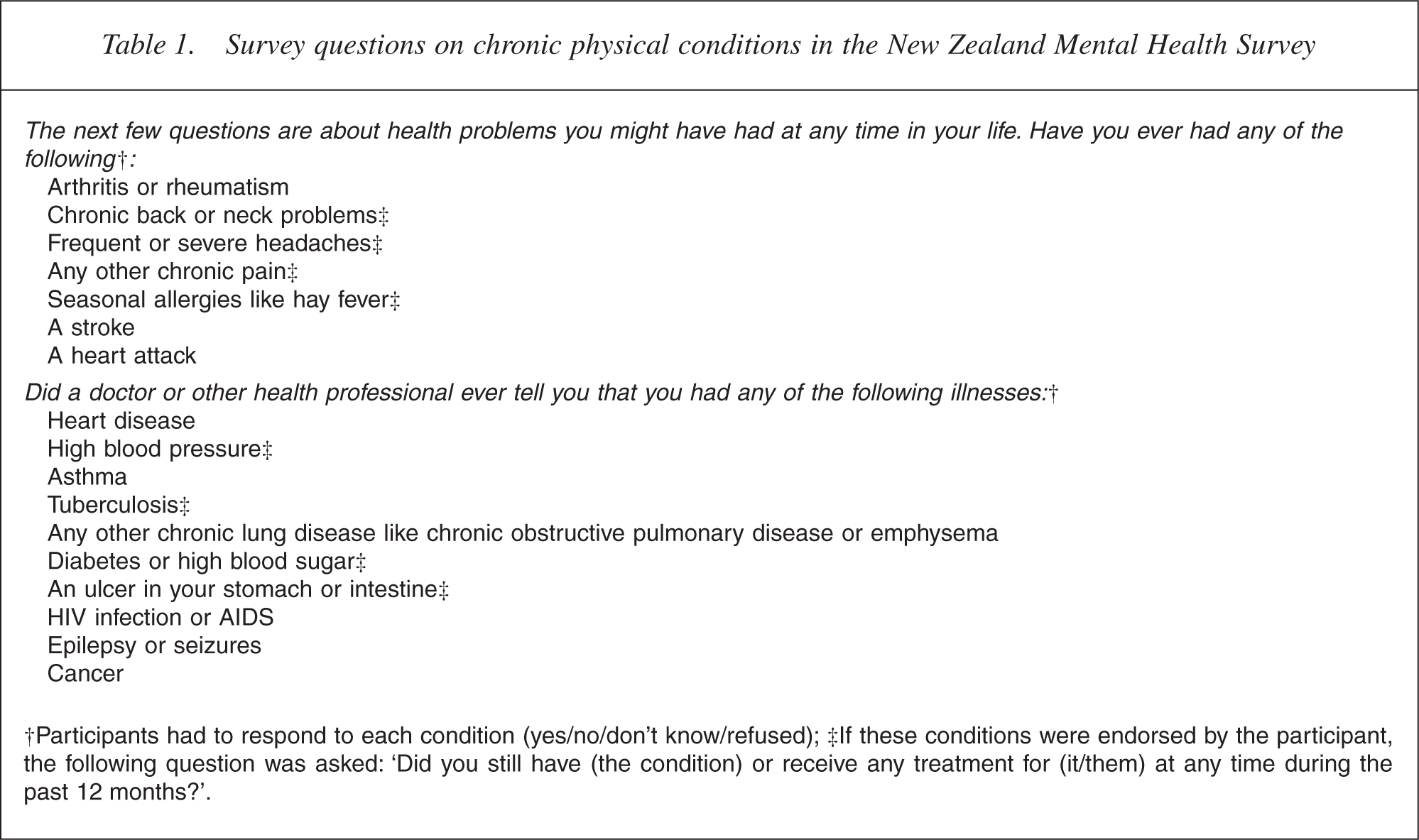
†Participants had to respond to each condition (yes/no/don't know/refused); ‡If these conditions were endorsed by the participant, the following question was asked: ‘Did you still have (the condition) or receive any treatment for (it/them) at any time during the past 12 months?’.
Prevalence of chronic physical conditions (experienced in the past 12 months) among people with 12 month mental disorder, adjusted for age†‡§
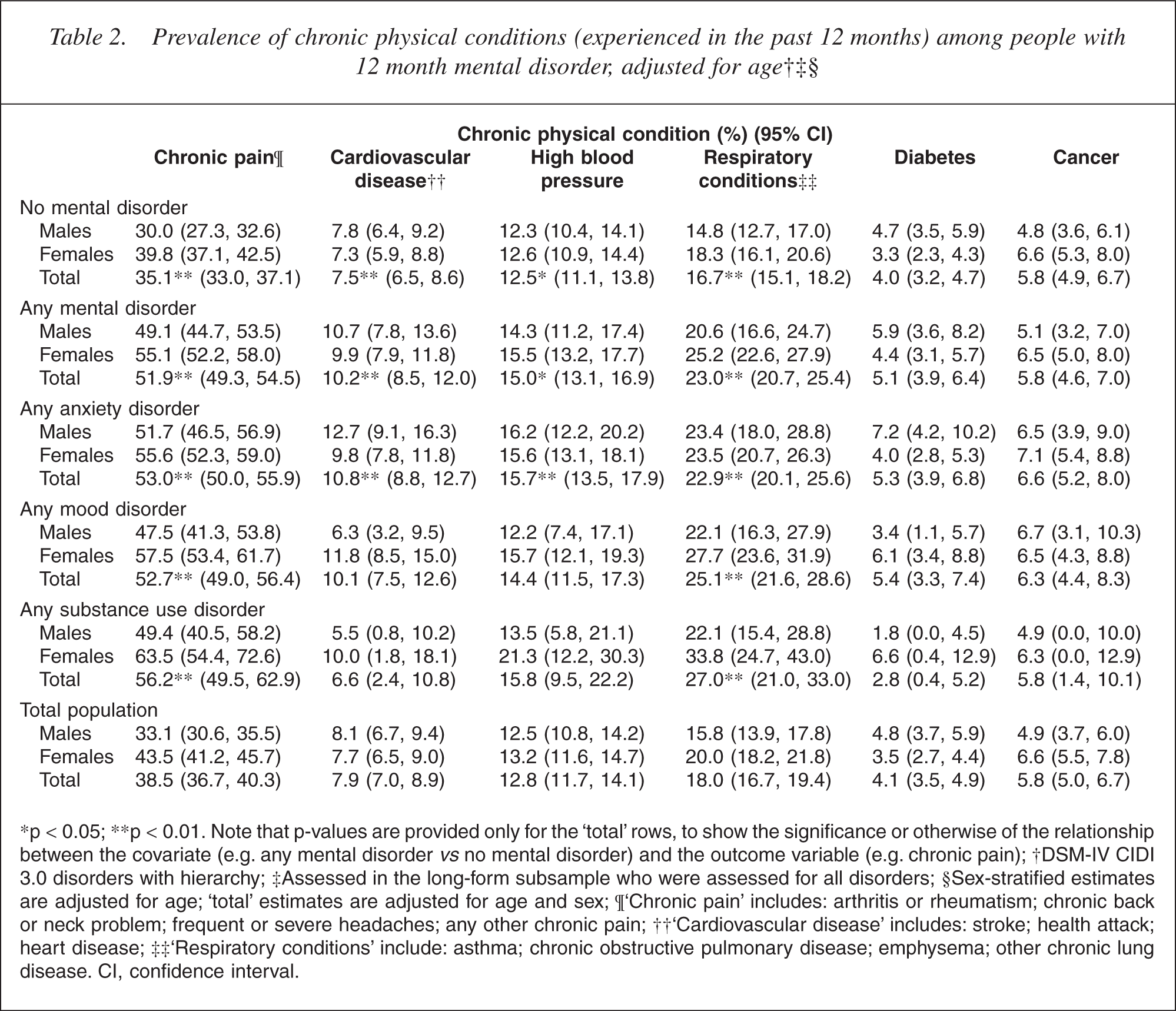
∗p <0.05; ∗∗p < 0.01. Note that p-values are provided only for the ‘total’ rows, to show the significance or otherwise of the relationship between the covariate (e.g. any mental disorder vs no mental disorder) and the outcome variable (e.g. chronic pain); †DSM-IV CIDI 3.0 disorders with hierarchy; ‡Assessed in the long-form subsample who were assessed for all disorders; §Sex-stratified estimates are adjusted for age; ‘total’ estimates are adjusted for age and sex; ¶‘Chronic pain’ includes: arthritis or rheumatism; chronic back or neck problem; frequent or severe headaches; any other chronic pain; ††‘Cardiovascular disease’ includes: stroke; health attack; heart disease; ‡‡ ‘Respiratory conditions’ include: asthma; chronic obstructive pulmonary disease; emphysema; other chronic lung disease. CI, confidence interval.
Prevalence of selected chronic physical condition risk factors (experienced in the past 12 months) by12 month mental disorder group, age adjusted†‡§
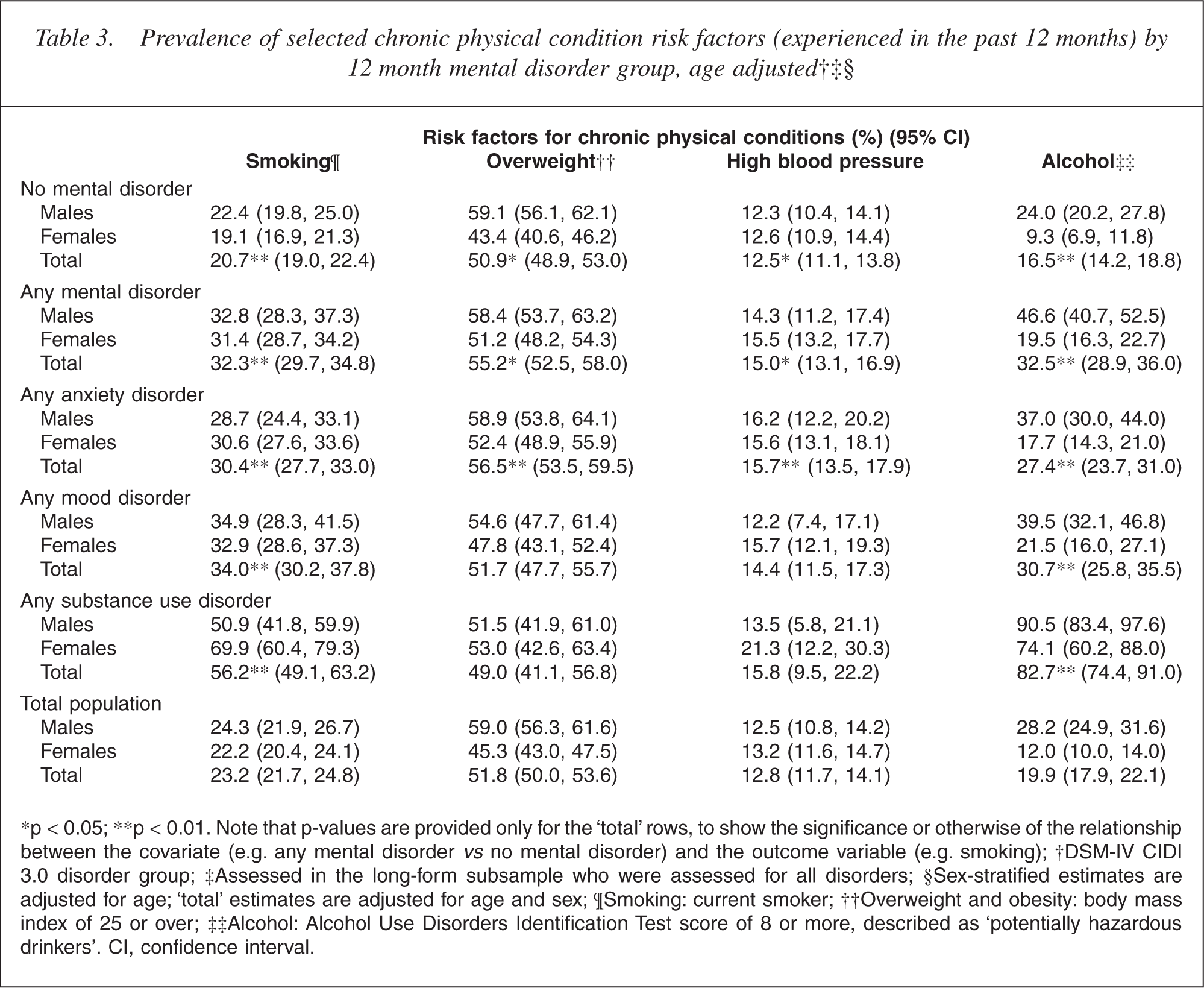
∗p <0.05; ∗∗p < 0.01. Note that p-values are provided only for the ‘total’ rows, to show the significance or otherwise of the relationship between the covariate (e.g. any mental disorder vs no mental disorder) and the outcome variable (e.g. smoking); †DSM-IV CIDI 3.0 disorder group; ‡Assessed in the long-form subsample who were assessed for all disorders; §Sex-stratified estimates are adjusted for age; ‘total’ estimates are adjusted for age and sex; ¶Smoking: current smoker; ††Overweight and obesity: body mass index of 25 or over; ‡‡Alcohol: Alcohol Use Disorders Identification Test score of 8 or more, described as ‘potentially hazardous drinkers’. CI, confidence interval.
Prevalence of 12 month mental disorders among people with selected chronic physical conditions(experienced in the past 12 months)†‡§
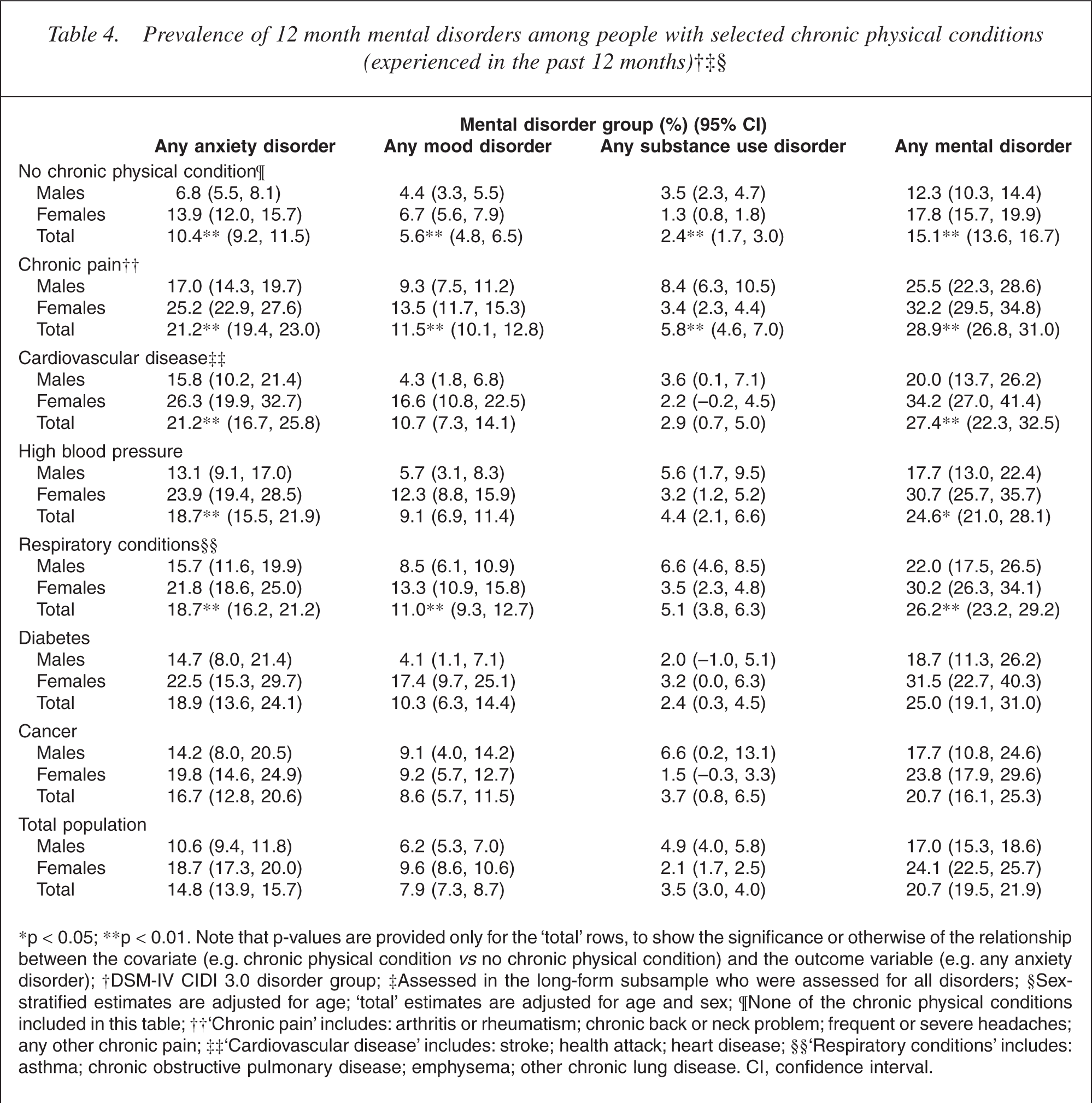
∗p <0.05; ∗∗p < 0.01. Note that p-values are provided only for the ‘total’ rows, to show the significance or otherwise of the relationship between the covariate (e.g. chronic physical condition vs no chronic physical condition) and the outcome variable (e.g. any anxiety disorder); †DSM-IV CIDI 3.0 disorder group; ‡Assessed in the long-form subsample who were assessed for all disorders; §Sex-stratified estimates are adjusted for age; ‘total’ estimates are adjusted for age and sex; ¶None of the chronic physical conditions included in this table; ††‘Chronic pain’ includes: arthritis or rheumatism; chronic back or neck problem; frequent or severe headaches; any other chronic pain; ‡‡‘Cardiovascular disease’ includes: stroke; health attack; heart disease; §§ ‘Respiratory conditions’ includes: asthma; chronic obstructive pulmonary disease; emphysema; other chronic lung disease. CI, confidence interval.
Analysis
Estimates were weighted to take into account the probability of selection, to adjust for oversampling, to adjust for non-response, and to post-stratify by age, sex and ethnicity to the 2001 census population. Logistic regression models were used to generate adjusted prevalence estimates (predictive marginals) that controlled for the differential age and sex distribution of those with and without the specified disorder. Analyses were carried out using SUDAAN 9.0.1. Taylor series linearization was used to approximate the variance of estimates [18]. For prevalences with less than 30 events in the numerator, confidence intervals were calculated according to a method by Korn and Graubard [19].
Results
Physical disease status of people with mental disorders
As Table 2 shows, people with any mental disorder, relative to those no mental disorder, had higher prevalences of several chronic physical conditions, namely chronic pain (51.9% vs 35.1%) (p < 0.0001), cardiovascular disease (10.2% vs 7.5%) (p < 0.005), high blood pressure (15.0% vs 12.5%) (p < 0.02) and respiratory conditions (23.0% vs 16.7%) (p < 0.0001). Cancer was equally prevalent in those with and without mental disorders (5.8% vs 5.8%).
Sex differences in the prevalence of chronic physical conditions were generally consistent across the populations with and without mental disorders. There were however, two significant interactions involving sex. Females with mood disorder had nearly twice the prevalence of cardiovascular disease as corresponding males, but there was no such sex difference in cardiovascular disease prevalence among those without mood disorder (p < 0.02). The same pattern occurred for diabetes (p < 0.03).
Table 3 shows higher prevalences of current smoking (32.3% vs 20.7%) (p < 0.0001), overweight/obesity (55.2% vs 50.9%) (p = 0.01), high blood pressure (15.0% vs 12.5%) (p < 0.02), and hazardous alcohol use (32.5% vs 16.5%) (p < 0.0001) among people with any mental disorder compared with people without mental disorder. The finding for alcohol use is inflated by the ‘any mental disorder’ category including people with diagnosed substance use disorders, most of whom have alcohol use disorders. However, the prevalence of hazardous alcohol use was still significantly higher among people with mood disorders (p < 0.0001) and anxiety disorders (p < 0.0001) compared with people without.
The prevalence of being overweight or obese was higher among females with any mental disorder (51.2%) than females without mental disorder (43.4%), but the same relationship did not occur for males (58.4% vs 59.1%). This significant interaction (p < 0.02) can be expressed another way: in both the population with and without mental disorder females had lower prevalence of overweight/obesity than males, but the sex difference narrows in the population with any mental disorder (and disappears altogether in the population with substance use). Table 3 also shows a wider sex difference in the total population estimates of overweight/obesity than observed in surveys which have used objective measures of height and weight rather than self-report [20]. This suggests a small degree of underestimation of weight by women and overestimation of weight (or height) by men in this survey. But such biased estimates are unlikely to explain the interaction between sex and mental disorder for overweight/obesity noted above.
Mental health status of people with chronic physical conditions
Table 4 shows the same mental-physical comorbidities as Table 2, but with chronic physical conditions as denominator. The same significant relationships therefore occur across both Tables 2 and 4, the point of difference being in the patterns of prevalence. Table 4 shows that the prevalence of mental disorder in the population with chronic physical conditions is generally in the range of 25–29% compared with 15.1% among those without chronic physical conditions. In Table 4, the significant relationships between sex, mood disorder and cardiovascular disease/diabetes noted earlier manifest themselves as a wider sex difference (females higher) in the prevalence of mood disorder among those with either cardiovascular disease or diabetes relative to those without those chronic physical conditions.
Discussion
Three main findings emerged from this study. First, people with mental disorders carry a significantly higher burden of physical disorder than age-matched people without mental disorders. Two-thirds (67.7%) of the population with mental disorder have at least one of the chronic physical conditions included here compared with half the population (52.9%) without mental disorders (data available on request). Second, around a quarter (25.9%) of people with chronic physical conditions have a comorbid mental disorder compared with 15.1% of the population without chronic physical conditions. Third, there are significant relationships between some mental disorders and each of obesity, cardiovascular disease and diabetes that occur for women, but not for men.
The findings of poorer physical health among those with mental disorders and poorer mental health status among those with physical disease are consistent with research cited earlier, and point to a reliable relationship between mental and physical disorder. In this paper only concurrent reports are presented, so the direction of the relationship cannot be determined, but evidence exists for both pathways from physical illness to mental disorder [8, 21] and from mental disorder to physical illness [21, 22].
The finding that the prevalence of overweight/obesity was higher among females with mental disorder but not among corresponding males has been hypothesized [23], but not frequently investigated. The two population studies that have done so both found a relationship between obesity and depression for women, but not men [24, 25]. Interestingly, no other study to our knowledge has investigated the relationship between mental disorders other than depression, with sex and obesity, and the findings in the current study are stronger for anxiety and substance disorders than for mood disorders. However, these findings distinguishing between mental disorder groups are tentative as comorbidity was not controlled for in the analyses. It should also be noted that underweight and normal weight individuals were combined in these analyses and if there is a non-linear relationship between body mass index and mental disorders this would have the effect of attenuating the associations obtained. The results reported here may therefore be a conservative depiction of the true association.
The relationships between cardiovascular disease/diabetes and mood disorder that occur in females in this study (or more particularly, the absence of any corresponding relationships for males) should be also treated with caution as they were not anticipated. Nonetheless, the finding for diabetes is not entirely without precedent. A meta-analysis of 42 studies on the prevalence of depression in diabetes [26] concluded that the odds of depression in diabetes were twice that of the non-diabetic group, but did not differ by sex. However, two studies have found a greater-than-expected sex differential in depression prevalence in diabetes [27, 28].
In the case of cardiovascular disease, the little research that is informative on the issue indicates that the general population female : male ratio for depression of around 2:1 is preserved in those with heart disease [29, 30]. But surprisingly few studies address this question directly, and the morbidity and mortality outcomes of women with heart disease-depression comorbidity may be worse than for men [31], so sex differences in the depression-cardiovascular disease relationship may warrant further exploration.
Given the public health significance, and the interdependence of cardiovascular disease, diabetes, mental disorder and obesity in New Zealand, as in other developed countries, the finding that their comorbidity is particularly prevalent among females may be of considerable importance, should it be replicated. These results concerning the prevalence of mental-physical comorbidity as a whole should be borne in mind by clinicians working in both mental health and medical services. The findings underscore the challenge of providing for the concurrent mental and physical health needs of service users within the context of a health system where specialist mental health and medical services function largely independently of each other.
Footnotes
Acknowledgements
Te Rau Hinengaro: The New Zealand Mental Health Survey (NZMHS) was funded by the Ministry of Health, the Alcohol Advisory Council of New Zealand and the Health Research Council of New Zealand. The survey was carried out in conjunction with the World Health Organization WMH Survey Initiative. We thank the WMH staff for assistance with instrumentation, fieldwork and data analysis. These activities were supported by the US National Institute of Mental Health (R01-MH070884), the John D and Catherine T MacArthur Foundation, the Pfizer Foundation, the US Public Health Service (R13-MH066849, R01-MH069864, and R01-DA016558), the Fogarty International Center (FIRCA R01-TW006481), the Pan American Health Organization, Eli Lilly and Company, Ortho-McNeil Pharmaceutical, Inc., GlaxoSmithKline, and Bristol-Myers Squibb. WMH publications are listed at ![]() .
.
Other members of the NZMHS research team are: J Baxter, J Kokaua, TK Kingi, R Tapsell, S Foliaki, D Schaaf, MH Durie, C Tukuitonga and C Gale.
We thank the Kaitiaki Group and the Pacific Advisory Group for their input and support for this survey and we thank all the participants.