
Abstract
beyondblue: the national depression initiative is a national, independent, non-profit organization funded by Australian national, state and territory governments. Its stated mission is to ‘Provide a national focus and community leadership to increase the capacity of the Australian community to prevent depression and respond effectively to it’ [1]. It has five priority areas: community awareness and destigmatization, consumer and carer support, prevention and early intervention, primary care training and support, and applied research [1]. The organization was started in October 2000 as a five-year initiative.
The organization is largely funded by the Australian and Victorian governments, with smaller contributions from South Australia, Tasmania, Queensland, Northern Territory and the Australian Capital Territory. The states of New South Wales and Western Australia have not contributed. There has also been financial and in-kind support from a number of non-government sources.
The purpose of this paper is to evaluate the effects of beyondblue's community awareness work. Similar national campaigns have been carried out in other countries, but there is only limited information on their effectiveness [2]. A major problem in trying to evaluate national campaigns is the absence of a control group, making it difficult to separate the effects of the campaign from other influences that are present in a community at the same time. For example, in the United Kingdom, the Defeat Depression Campaign was evaluated by repeat national surveys [3]. Changes were found in the public's awareness of depression as a medical condition and in their views about antidepressant medication as a treatment. However, it is impossible to know whether these changes would have occurred even without the campaign.
Using data from Australian national surveys of mental health literacy carried out in 1995 and 2003–04, we have reported that the public's recognition of depression has increased, and their beliefs about treatment have changed to be more like those of mental health professionals [4]. However, as for the repeat UK surveys, it is difficult to attribute these changes to any specific factors such as beyondblue. In the present paper, we have attempted to overcome this limitation by using the states that did not fund beyondblue as a control group for those that did, on the assumption that the former will have a lower exposure to beyondblue's messages. Our prediction was that there will be greater change in the high-exposure states and territories than in the lowexposure states.
Method
1995 baseline survey
The methods of the 1995 survey have been described previously [5]. Briefly, the Australian Bureau of Statistics carried out a household survey covering all private dwellings in urban and rural areas, excluding the sparsely populated areas, across all states and territories. Interviewers made at least five call-backs in urban areas and at least three in rural areas before a dwelling was classified as ‘non-contact’. Contact was made with 2531 households, with one person aged 18 years or over randomly sampled per household, and 2164 persons (85%) agreed to participate. Because a pilot study had shown reduced comprehension of the interview in persons aged more than 75 years, this age group was excluded, giving a sample of 2031 aged 18–74 years.
The interview was based on a vignette of a person with a mental disorder. On a random basis, respondents were shown a vignette of either a person with depression or one with schizophrenia. Respondents were also randomly assigned to receive either male (‘John’) or female (‘Mary’) versions of the vignette. Only the depression vignette, received by 1010 persons, is relevant here. This vignette (John version) was:
John is 30 years old. He has been feeling unusually sad and miserable for the last few weeks. Even though he is tired all the time, he has trouble sleeping nearly every night. John doesn't feel like eating and has lost weight. He can't keep his mind on his work and puts off making decisions. Even day-to-day tasks seem too much for him. This has come to the attention of his boss, who is concerned about John's lowered productivity.
After being presented with the vignette, respondents were asked two open-ended questions: ‘What would you say, if anything, is wrong with John/Mary?’ and ‘How do you think John/Mary could best be helped?’ Then followed a series of questions asking the respondent to rate the likely helpfulness of various interventions (rated as likely to be helpful, harmful or neither for the person in the vignette). The interventions were: a typical general practitioner (GP) or family doctor; a typical chemist (pharmacist); a counselor; a social worker; a telephone counseling service, such as Lifeline; a psychiatrist; a psychologist; help from close family; help from close friends; a naturopath or a herbalist; the clergy, a minister or priest; John/Mary tried to deal with his/her problems on his/her own; vitamins and mineral, tonics or herbal medicines; pain relievers, such as aspirin, codeine or Panadol; antidepressants; antibiotics; sleeping pills; antipsychotics; tranquillisers such as valium; becoming physically more active, such as playing more sport, or doing a lot more walking or gardening; reading about people with similar problems and how they have dealt with them; getting out and about more; attending courses or relaxation, stress management, meditation or yoga; cutting out alcohol altogether; psychotherapy; hypnosis; being admitted to a psychiatric ward of a hospital; undergoing electro-convulsive therapy (ECT); having an occasional alcoholic drink to relax; going on a special diet or avoiding certain foods. Next were questions asking about the likely result for the person in the vignette with and without ‘the sort of professional help you think is most appropriate’. The response options were: Full recovery with no further problems; Full recovery, but problems would probably re-occur; Partial recovery; Partial recovery, but problems would probably re-occur; No improvement; Get worse.
The rest of the interview is not relevant to the analyses reported here; it involved questions on knowledge of causes and risk factors, beliefs associated with stigma and discrimination, contact with people like those in the vignette, and the health of the respondent.
2003–04 survey
This survey was carried out by the company AC Nielsen following as closely as possible the methodology of the earlier survey. Households were sampled from 250 census districts covering all states and territories and metropolitan and rural areas. There were up to three callbacks to each household. To achieve a target sample of 4000 interviews with adults aged 18 years or over, visits were made to 28 947 households. The outcome of these visits was: no contact after repeated visits 14 630; vacant house or lot 306; refused 7815; person sampled within household temporarily unavailable 1132; no suitable respondent in household 287; did not speak English 383; incapable of responding 213; and unavailable for the duration of the survey 181. The interviews were carried out between November 2003 and February 2004.
The 2003–04 survey incorporated all the questions of the earlier survey, but also had some additional questions. Furthermore, respondents were randomly assigned to receive one of four vignettes. Most of the additional questions and vignettes were not used in the present analyses, so they are not described here. However, this survey did ask questions that are relevant to the awareness of beyondblue. These questions included: ‘Have you heard of any organizations related to depression?’; (if yes) ‘Can you tell me/remember the names of any of these organizations?’; ‘Have you heard of the organization called beyondblue: the national depression initiative?’; ‘And finally, have you heard of the organization called The Mellow Yellow Institute?’ The latter is a fictitious organization which was used as a control to assess what proportion of those recognizing beyondblue may have been false positives.
One difference between this and the earlier survey was that it included all adults aged 18+, including those aged 75 and over. To make the samples more comparable, the latter age group was dropped from the analyses reported here. This left 910 persons who received the depression vignette. However, the data on awareness of beyondblue were available on all participants in the survey, not just those receiving the depression vignette. Because we did not need to compare the awareness questions with the 1995 survey, we included all age groups, giving a sample of 3998 persons.
Statistical analysis
Data were pooled across male and female versions of the vignette, because analysis of the 1995 survey had shown that this variable made little difference to responses. Percentage responses for each vignette were compared for the high- and low-exposure states in 1995 and 2003–04. In 1995, there were 687 respondents in the highexposure states and 323 in the low-exposure states. In 2003–04, the respective numbers were 522 and 388.
Percentages were calculated applying survey weights to give better population estimates; 95% confidence intervals of these percentages were estimated using the Complex Samples procedure in SPSS 12.0. For the 2003–04 survey, we took account of the geographical clustering in the sample as well as the surveys weights in estimating confidence intervals. However, sample clustering information was not available for the 1995 survey. This means that the confidence intervals are more accurate for the 2003–04 survey and are likely to narrower than they should be for the 1995 survey. However, we found that taking account of the clustering had only a small effect on the confidence intervals for the 2003–04 survey, so that the 1995 confidence intervals are likely to be affected little by ignoring clustering.
Results
Awareness of beyondblue
Table 1 shows the percentage of respondents in each state and territory who spontaneously mentioned beyondblue as an organization related to depression. Mention was lower in New South Wales and Western Australia, the states that have not funded beyondblue, than in the other states and territories.
Awareness of beyondblue in each state or territory: percent aware (and 95% CI)
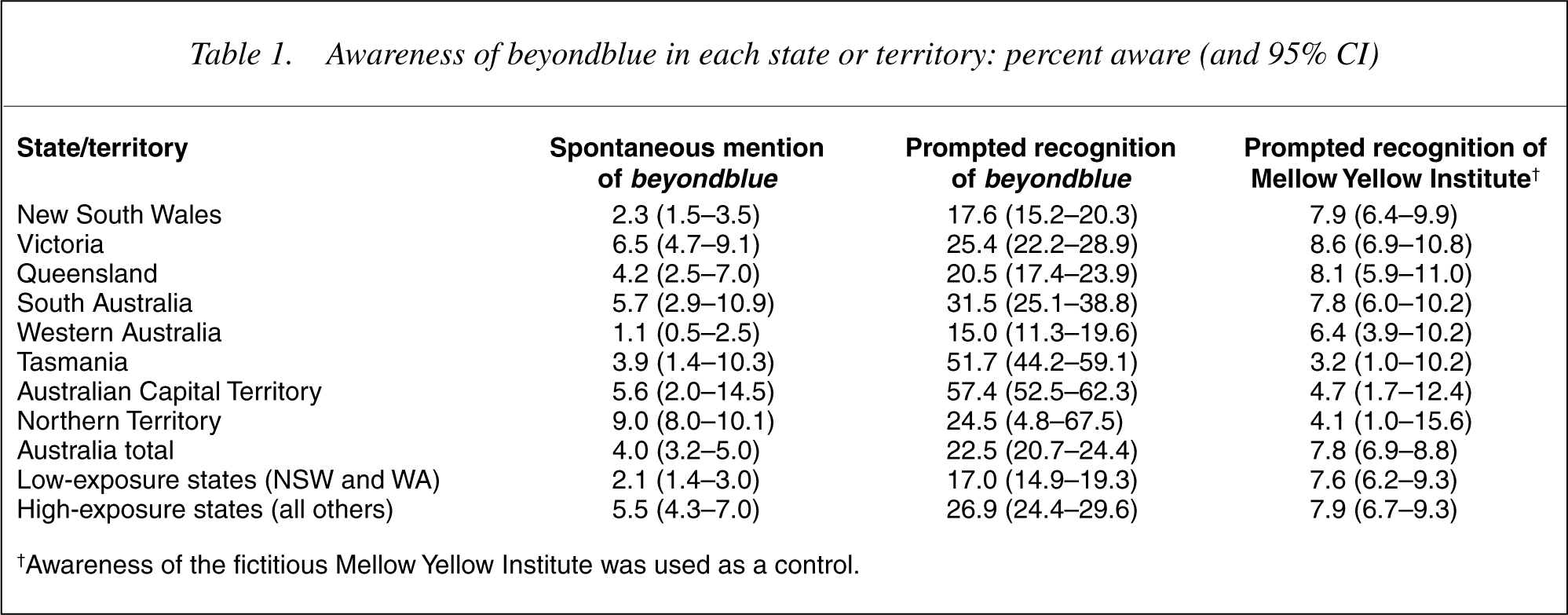
†Awareness of the fictitious Mellow Yellow Institute was used as a control.
Table 1 also shows recognition of beyondblue and of the fictitious Mellow Yellow Institute. While there were some large differences in recognition of beyondblue, with New South Wales and Western Australia again being lower, the recognition of the Mellow Yellow Institute showed very similar results across states and territories.
The bottom rows of Table 1 show the summary results for the lowand high-exposure states. Spontaneous mention was more than twice as great in the high-exposure states. For recognition, it is possible to subtract the percentage recognizing the Mellow Yellow Institute from the percentage recognizing beyondblue to get a more realistic estimate. This method produced 9.4% recognition in the low-exposure states compared to 19.0% in the high-exposure states, i.e. around twice as high in the latter.
To see if the high- and low-exposure states were matched sociodemographically, we compared them on age distribution and on level of education. There were no differences in age nor in the percentage with a degree or diploma.
Recognition of depression
Table 2 shows the percentages recognizing depression in the case vignette. Recognition increased greatly in both high- and low-exposure states over the 8-year period. Although the change was greater in the high-exposure states, this was attributable to a lower level of recognition in 1995 rather than a difference in 2003–04.
Recognition of depression in a case vignette

Treatment beliefs
Table 3 shows the percentages rating various interventions as likely to be helpful for the person in the depression vignette. Ratings of likely helpfulness increased over the 8-year period for most interventions, while the ratings for dealing with the problem alone decreased. However, there was differential change between the high- and low-exposure states for a number of interventions. The most striking results are for counsellor, phone counselling, antidepressants, tranquillizers and sleeping pills. All of these interventions showed a greater increase in helpfulness ratings in the high-exposure states. By contrast, dealing with the problem alone showed a greater decrease in helpfulness ratings in the high-exposure states. There was also a trend in the opposite direction for the helpfulness of a chemist (pharmacist), with the lowexposure states showing a greater increase.
Percentage of population rating various interventions as likely to be helpful for depressed depression
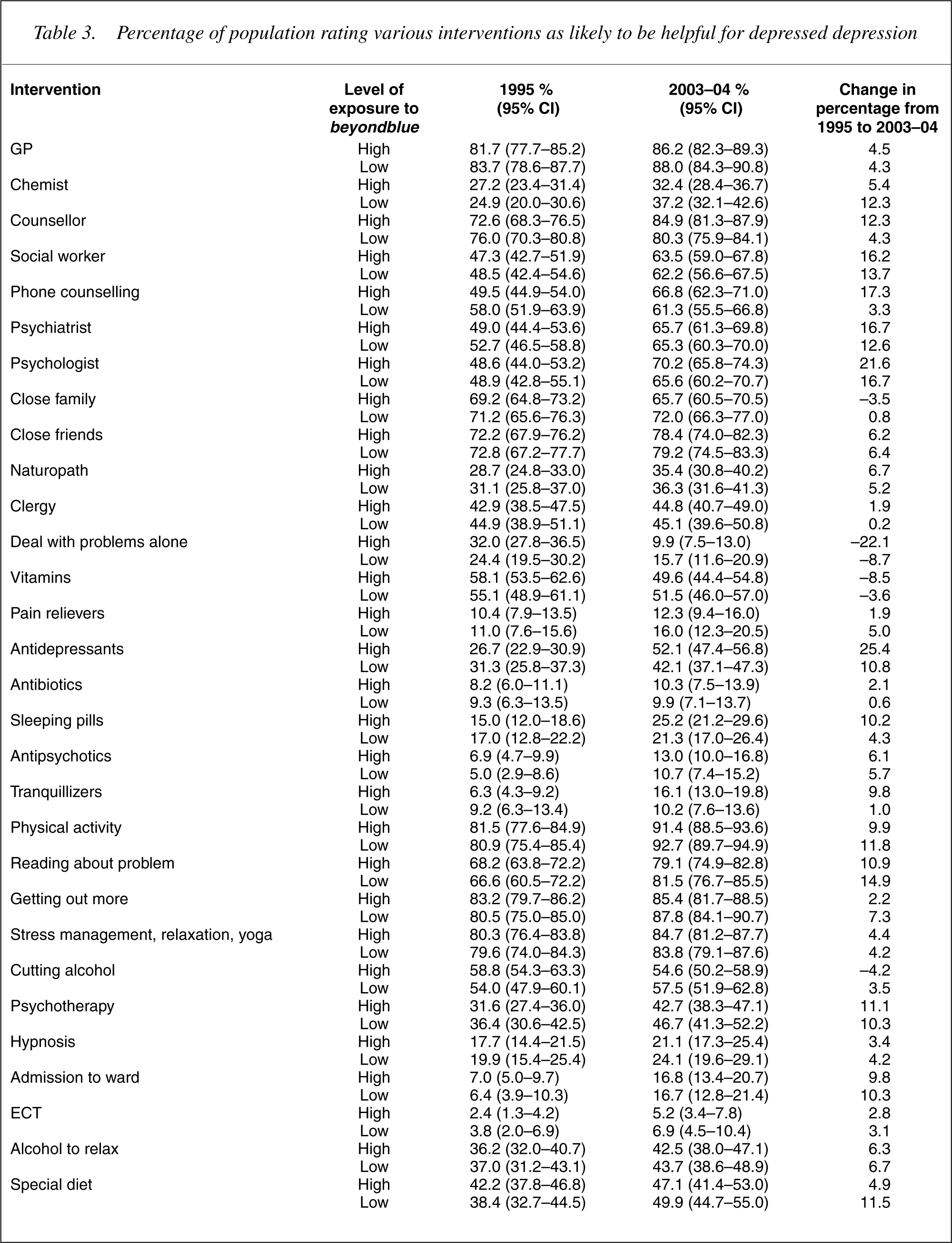
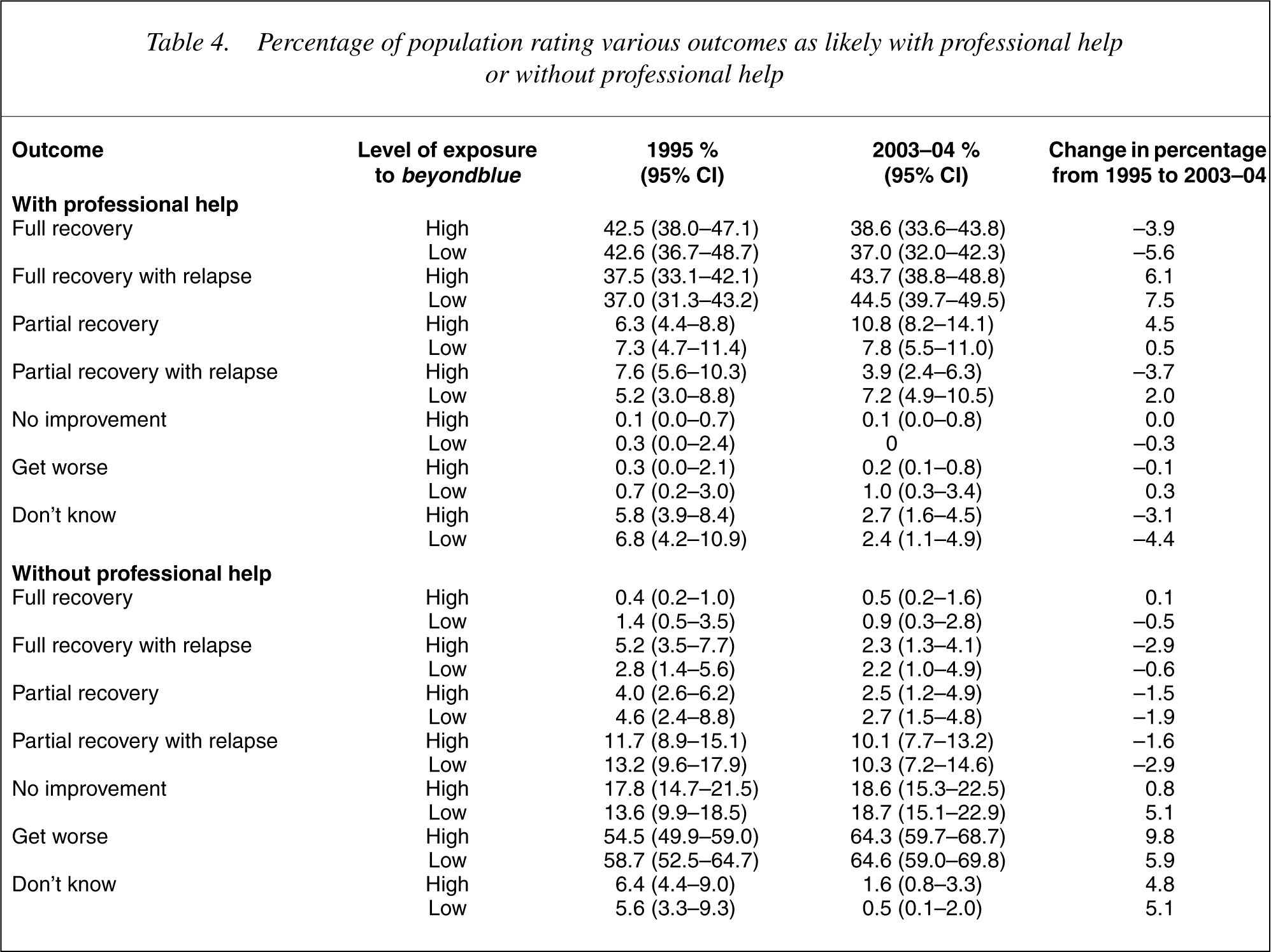
Table 4 shows the results on beliefs about outcomes with and without professional help. There were no large changes and what changes were found did not differ greatly between the high- and lowexposure states.
Percentage of population rating various outcomes as likely with professional help or without professional help
Discussion
The basic assumption behind the present analysis is that the states and territories that funded beyondblue would have a greater exposure to its messages than the states that did not. This assumption was supported by the finding that awareness of beyondblue was approximately twice as high in the states and territories that funded the organization.
We found that the high-exposure states had a greater increase in belief in the helpfulness of several interventions (counsellor, phone counselling, antidepressants and tranquillizers) than the low-exposure states. Conversely, the high-exposure states showed a greater decrease in the belief that it is helpful to deal with depression alone. These changes can be usefully judged in terms of professionals' beliefs about interventions for depression. During the late 1990s we surveyed national samples of psychiatrists, clinical psychologists and GPs using the same depression vignette [6]. We found that there was a professional consensus that the depressed person would be helped by seeing a GP, psychiatrist, clinical psychologist, taking antidepressants, receiving counselling and cognitive-behaviour therapy. The professionals were also against dealing with depression on one's own. Exposure to beyondblue appears to have brought the public closer to professionals in beliefs about antidepressants and counselling, as well as about the value of help-seeking in general. Public belief in GPs was very high even in 1995, so there was not much room for beyondblue to have an impact in this area. Belief in psychiatrists and psychologists increased nationally over the 8-years period, and tended to increase more in the high-exposure states, but the difference was not large. We did not specifically ask the public about cognitivebehaviour therapy, only about psychotherapy in general, based on the assumption that they would not be able to clearly differentiate different types of psychotherapy.
A surprising finding was the increase in belief about tranquillizers and sleeping pills in the high-exposure states. Perhaps this is a spill-over from the increase in belief in antidepressants, with some members of the public unable to differentiate the various classes of medication. However, despite this increase, belief in antidepressants is much more common in the population than belief in tranquillizers or sleeping pills for depression, which is consistent with professional views.
The impact of beyondblue is likely to be larger than the present results indicate, for two reasons. The first is that the low-exposure states did have some exposure to beyondblue, probably through some national media coverage. We did not have any nonexposed regions, which would have provided the ideal control. The second reason is that beyondblue is a five-year initiative, whereas our second survey was carried out after only 3 years of exposure. The effect could arguably be greater after the full 5 years.
The present analyses have some limitations which must be acknowledged. The questions asked in the surveys were not specifically designed to assess the messages that beyondblue has tried to communicate, so some effects might be missed. Also, there may have been methodological differences between surveys, which produced some of the changes found, although use of low-exposure states as controls helps in this regard. There were also some baseline differences between the high- and low-exposure states, which means that they were not always matched to start with. Finally, it is possible that the states and territories that funded beyondblue may have had other programs which affected knowledge and attitudes to depression. We have no information on whether such programs were more likely in the high-exposure states. On the other hand, the study has considerable strengths, with baseline data available well before beyondblue started, and having a control population for comparison.
Finally, it is important to note that although beyondblue contributed financially to have some questions added to the 2003–4 survey, this organization had no involvement in the design of the present evaluation, the analysis of the data or in the interpretation of the results.
Conclusion
The data are consistent with beyondblue having had a positive effect on some beliefs about depression treatment, most notably counselling and medication, and about the value of help-seeking in general. These findings suggest that national awareness campaigns may be effective in improving community mental health knowledge. The data also demonstrate the potential value of population monitoring of mental health literacy.
Footnotes
Acknowledgements
The 1995 survey was carried out with funding from a National Health and Medical Research Council Unit Grant. The 2003–04 survey was carried out as part of the Australia-Japan Partnership, a cross-national study of mental health literacy in both countries. This survey was funded by the Australian Department of Health and Ageing, a National Health and Medical Research Council Program Grant, and beyondblue: the national depression initiative. We thank our colleagues involved in the 1995 survey and Kelly Blewitt for research assistance with the 2003–04 survey.